Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
The canine transmissible venereal tumor by m. i. mello martins, f. ferreira de souza and c. gobello; a1233.0405
In: Recent Advances in Small Animal Reproduction, Concannon P.W., England G., Verstegen III J. and Linde-Forsberg C. (Eds.). International Veterinary Information Service, Ithaca NY (www.ivis.org), 25-Apr-2005; A1233.0405
The Canine Transmissible Venereal Tumor: Etiology, Pathology, Diagnosis and
Treatment M. I. Mello Martins1, F. Ferreira de Souza2 and C. Gobello3
1,2 Laboratory of Small and Exotic Animal Reproduction, Department of Animal Reproduction and Veterinary Radiology,
Faculty of Veterinary Medicine and Animal Science, UNESP Botucatu, Botucatu, Brazil.1Department of Veterinary Clinics, University of Londrina State (UEL), Londrina, Brazil. 3Faculty of Veterinary Science, National University of La Plata, La Plata, Buenos Aires, Argentina.
Introduction
Transmissible venereal tumor (TVT), also known as infectious sarcoma, venereal granuloma, transmissible lymphosarcoma or Sticker tumor, is a benign reticuloendothelial tumor of the dog that mainly affects the external genitalia (Fig. 1 and Fig. 2) and occasionally the internal genitalia (Fig. 3a, Fig. 3b, and Fig. 3c). As it is usually transmitted during coitus [1] it mainly occurs in young, sexually mature animals [2]. TVT also affects wild canids [3]. Transmissible venereal tumor cells contain an abnormal number of chromosomes ranging from 57 to 64 and averaging 59, in contrast to the normal 78 of the species. Surface antigen characteristics suggest that all TVTs arose from a single original canine tumor [2]. The capacity of immunologic response of the host has a main role in the expansion of such tumors [4] with an increase in severity seen in immunologically compromised animals.
Figure 1. A cauliflower like transmissible venereal tumor protruding from the vulva in a 4 year old crossbreed bitch. - To view this image in full size go to the IVIS website at www.ivis.org . -
Figure 2. Transmissible venereal tumor on the glands penis of a 6 year old, crossbreed dog. - To view this image in full size go to the IVIS website at www.ivis.org . -
Figure 3a. Transmissible venereal tumor in the cranial vagina of a 3 year old, crossbreed bitch. Abdominal radiography showing a mass. - To view this image in full size go to the IVIS website at www.ivis.org . -
Figure 3b. Transmissible venereal tumor in the cranial vagina of a 3 year old, crossbreed bitch. During the surgery. - To view this image in full size go to the IVIS website at www.ivis.org . -
Figure 3c. Transmissible venereal tumor in the cranial vagina of a 3 year old, crossbreed bitch. Excised genital tract. - To view this image in full size go to the IVIS website at www.ivis.org . -
Although TVT has a cosmopolitan distribution, it is most frequently encountered in tropical and subtropical zones [2]. In South America it is commonly found in urban areas with large populations of free-roaming dogs. The current review is based on the experience of the authors in Brazil and Argentina, and on relevant publications [1-44].
Etiopathology
Canine TVT was initially described by Novinsky in 1876, who demonstrated that the tumor could be transplanted from one susceptible host to another by inoculating it with tumoral cells [5]. Cytoplasmatic inclusions found in the tumoral cells caused this neoplasia to be attributed to a viral agent by some authors [6], although the tumor could not consistently be transmitted by cell free extracts [1]. Presently, the consensus view is that TVT arise from allogenic cellular transplants [5] and that the abnormal cells of the neoplasm are the vectors of transmission. The exfoliation and transplantation of neoplastic cells during physical contact provide the main mode of transmission onto genital mucosa, and also onto nasal or oral mucosa, during mating or licking of affected genitalia, respectively [7,8]. The implantation of the tumor is facilitated by the presence of any mucosal lesion or by the loss of mucosal integrity [9].
The tumor growth appears 15 to 60 days after implantation. TVTs can either grow slowly and unpredictably for years or be invasive and eventually become malignant and metastasize [10,11]. TVTs are immunogenic tumors, and it has been demonstrated that the immune system of the host has a main role in inhibiting tumor growth and metastasis [4,7]. In young dogs or dogs with a compromised immune system, tumors may have a greater tendency to metastasize [12]. In one study metastases were more frequent in males (16%) than in females (2%) [44]. Metastases have been reported in less than 5 - 17 % of cases [2,5]. They have been described in subcutaneous tissue, skin, lymph nodes, eyes, tonsils, liver, spleen, oral mucosa, hypophysis, peritoneum, brain, and bone marrow [11,13-16] (Fig. 4 and Fig. 5). Extragenital lesions have been reported to occur both in isolation and in association with the genital lesions [5]. However, one report suggests that most if not all instances are secondary to genital lesions in that in over 500 cases neoplastic foci on genitalia could always be detected in cases where extragenital lesions were present [44]. Although, spontaneous remission has been described in experimental transplantation it has not been confirmed in natural cases [5,9].
Figure 4. Penile transmissible venereal tumor with inguinal lymphoid node metastasis. - To view this image in full size go to the IVIS website at www.ivis.org . -
Figure 5. Transmissible venereal tumor protruding through anus (top) and vulva (below) in a 2 year old, crossbreed bitch. - To view this image in full size go to the IVIS website at www.ivis.org . -
Immunological studies have demonstrated that the tumor is transplanted through barriers of main histocompatibility complexes (MHC) [17]. Immunocomplexes have been found in serum samples of dogs with TVT [18]. Tumor cells in the rapid growth phase do not express type I and II MHC antigens, while 30% to 40% of cells in the initial regression phase
express both antigens. This difference may be responsible for the additional immune response of the host, accelerating the regression of the tumor [12,17].
Differences in cell types have also been found between stages of tumor progression. Tumors in progressive growth have round cells with microvilli while regressing tumors present transitional rather fusiform cells. Moreover, regressing tumors have a high number of T lymphocytes [19,20]. It is thought that substances secreted by the lymphocyte infiltrate are responsible for the tumor’s regression by inducing cellular differentiation [12,20,21].
Gross and Microscopic Characteristics
Small pink to red, 1 mm to 3 mm diameter nodules can be observed 2 or 3 weeks after transplantation. Initial lesions are superficial dermoepidermal or pedunculated. Then, multiple nodules fuse together forming larger, red, hemorrhagic, cauliflower-like, friable masses. The masses can be 5 cm to 7 cm in diameter which then progress deeper into the mucosa as multilobular subcutaneous lesions with diameters that can exceed 10 - 15 cm. Tumors bleed easily and while becoming larger, normally ulcerate and become contaminated [22].
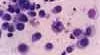
Cytological examination reveals the typical round to slightly polyhedral cells, with rather eosinophilic vacuolated thin cytoplasm and a round hyperchromatic nucleus with a nucleolus and a moderate number of mitotic figures [23]. The nucleus to cytoplasmic ratio is large (Fig. 6a and Fig. 6b).
Figure 6a. Transmissible venereal tumor cells. Nuclear pleomorphism, chromatin condensation and cytoplasmatic vacuoles. - To view this image in full size go to the IVIS website at www.ivis.org . -
Figure 6b. Canine transmissible venereal tumor cells. Note the mitotic activity in the cell near the center of the image, as evidenced by the irregular shaped nuclear material which appears to be in mitotic prophase or metaphase. - To view this image in full size go to the IVIS website at www.ivis.org . -
Histologically, TVTs are made up of a homogenous tissue with a compact mass of cells that are mesenchymal in origin and the borders of which cannot easily be differentiated [2,5,24]. There is frequently an infiltration of lymphocytes, plasma cells and macrophages [25]. TVTs should be differentiated from mastocytomas, histiocytomas or malignant lymphomas [5].
Diagnosis
Clinical signs vary according to the localization of the tumors. Dogs with genital localization have a hemorrhagic discharge. In males, lesions usually localize cranially on the glans penis, on preputial mucosa or on the bulbus glandis. Tumoral masses often protrude from the prepuce [26] and phimosis can be a complication [30]. The discharge can be confused with urethritis, cystitis, or prostatitis [2]. The involvement of regional lymph nodes is frequent in males with large tumors.
In bitches the tumors are of similar gross appearance as in male dogs and can be localized in the vestibule and/or caudal vagina, protruding from the vulva and frequently causing a deformation of the perineal region. Only very rarely, however, do they interfere with micturition. A considerable hemorrhagic vulvar discharge may occur and can cause anemia if it persists. The discharge can attract males and the condition of the bitch can be mistaken for estrus by the owners. Infrequently, TVTs can localize in the uterus [22]. In cases with extra genital localization of the TVT, clinical diagnosis is usually more difficult because TVTs cause a variety of signs depending on the anatomical localization of the tumor, e.g., sneezing, epistaxis, epiphora, halitosis and tooth loss, exophthalmos, skin bumps, facial or oral deformation along with regional lymph node enlargement [2].
Definitive diagnosis is based on physical examination and cytological findings typical of TVT in exfoliated cells obtained by swabs, fine needle aspirations or imprints of the tumors [5,11,27].
Treatment
Several treatments including surgery, radiotherapy, immunotherapy, biotherapy and chemotherapy have been applied for TVT. Surgery has been used extensively for the treatment of small, localized TVTs, although the recurrence rate can be as high as 50 - 68% in cases of large invasive tumors [2,24,28,29]. Contamination of the surgical site with TVT cells is also a source of recurrence [44]. Transmissible venereal tumors are radiosensitive and orthovoltage as well as cobalt have been used for this purpose [2,9,30].
Biotherapy studies have also been reported. The intratumoral application of Calmette-Guérin's bacillus (BCG) was used for
three weeks with sporadic success [8]. Recurrences have been described after immunotherapy using Staphylococcus protein A, BCG or a vaccine made from tumoral cells [2,42]. Biotherapy has unfortunately also resulted in a high rate of recurrence [5,9,42].
Chemotherapy has been shown to be the most effective and practical therapy, with vincristine sulfate being the most frequently used drug [31]. Vincristine (Oncovin®, Lily), is administered weekly at a dose of 0.5 to 0.7 mg/m2 of body surface area or 0.025 mg/kg, IV [7,24]. The involution of the lesions is gradual, although it is particularly noticeable and significant at the beginning of the treatment. Complete remission usually takes 2 to 8 injections [27,31] and occurs in more than 90% of the treated cases (unpublished observation). A cure rate approaching 100% is achieved in cases treated in the initial stages of progression, especially in cases of less than 1 year duration, and independent of the presence or not of metastases [44]. In cases of longer duration, longer periods of therapy are required, and the cure rate is lower [44]. Side effects can be expected. Cytostatic agents, such as vincristine, can cause myelosuppression and gastrointestinal effects resulting in leukopenia and vomiting in 5 to 7% of the patients. Paresis has also been described as a side effect due to peripheral neuropathy [31,32]. A complete white blood cell count is, therefore, recommended prior to each administration. When the white blood cell count is below 4,000 mm3 further administration should be delayed 3 to 4 days and the dose of vincristine can be reduced to 25% of the initial dose [1]. The most frequent complication of vincristine treatment is the occurrence of local tissue lesions caused by extravasation of the drug during IV application resulting in the development of necrotic lesions with crusts (Fig. 7a and Fig. 7b).
Figure 7a. Necrotic skin lesion caused by perivascular leakage of vincristine sulfate. Seven days after application. - To view this image in full size go to the IVIS website at www.ivis.org . -
Figure 7b. Necrotic skin lesion caused by perivascular leakage of vincristine sulfate. Fifteen days after application. - To view this image in full size go to the IVIS website at www.ivis.org . -
Other chemotherapeutic agents indicated for TVT treatment include cyclophosphamide (5 mg/kg, PO, for 10 days as a single drug therapy or given in association with prednisolone, 3 mg/kg, for 5 days); also, weekly vinblastine (0.1 mg/kg, IV during 4 to 6 weeks), methotrexate (0.1 mg/kg, PO, every other day) or a combination of the 3 drugs. However, there is no apparent advantage in the combination of chemotherapy over using vincristine alone [5,9,13,21].
Resistant cases can be treated with doxorubicin (Adriamycin®, Adria Lab, 30 mg/m2, IV, with 3 applications every 21 days) [5,43]. When total disappearance of the tumor cannot be achieved by chemotherapy, electro-cauterization or cryo-cauterization can be useful [2,9]. After therapy, small remnant lesions can disappear spontaneously after 1 or 2 weeks (unpublished observations). In cases that fail to resolve with chemotherapy, radiotherapy has been reported to yield good results [44].
Effects of Vincristine Treatment on Spermatogenesis
Spermatogenesis can be temporarilly or permanently altered by the administration of cytotoxic drugs [33,34]. Drug-altered spermatogenesis may not return to normal for one or more spermatic cycles [35]. It is known that vincristine reduces human fertility [30]. Studies in laboratory animals have shown that vincristine damages the DNA of germ cells thereby reducing the rate of development of these cells [36]. Vincristine can cause cytoplasmic protein precipitation, which in turn interferes with microtubule formation [33]. Little information is available on the long-term effects of vincristine on male dog fertility and most of the studies only have described semen quality during treatment [30,37].
In one study, 8 mature dogs were unilaterally orchidectomized and treated with vincristine 0.025 mg/kg given intravenously for 7 weeks. Then the remaining testis was excised. Histological evaluation on both testes revealed mild to moderate degeneration in the second testicle [34]. In the same study, semen was collected from 6 male dogs before, during and for up to 120 days after the same therapeutic protocol. An increase in sperm mid-piece and tail abnormalities, decrease in sperm motility and decrease in sperm concentration were found between weeks 2 to 4, 3 to 4 and 9 to 11, respectively, after the beginning of the treatment [34]. In another report in which a German shepherd was given vincristine sulphate 0.025 mg/kg intravenously for 3 weeks, treatment caused high teratozoospermia and total asthenozoospermia with unchanged libido, during 4 weeks of evaluation [37].
In a third study, 17 mature dogs were observed during vincristine treatment (0.6 mg/m2 per week for 4 weeks) during which complete regression of the tumors was achieved. Semen was evaluated before the beginning of the treatment, 3 days after each injection and 15 days after the last injection. Semen quality transiently deteriorated during the treatment but had returned to normal by 15 days after the last injection. The dogs had a normal GnRH response after each semen collection and retained normal libido during and after treatment [38]. This would appear to have been an epidydimal effect of the drug treatment.
Considering that in dogs spermatogenesis takes approximately 62 days, and the transport through the epididymis requires 15 days [39,40], long-term studies are required to define the effect of vincristine on semen quality and its effect on the fertility of stud dogs. A recent study described the effect of vincristine in a male Boxer with a genital TVT. The dog was and treated with vincristine intravenously at 0.5 - 0.7 mg/m2 of body surface area per week for 6 weeks and until complete regression of the tumor. Libido, testicular size and consistency were not altered either during or after treatment. Total sperm count decreased to low values (<200 x106), during weeks 4 and 5 and then increased to higher than pre-treatment values (440 x106). Percentages of progressive motility and morphological abnormalities remained within normal range and the dog sired a normal litter within one year after treatment [41]. Such results show that gonadal response to treatment varies among individuals.
Conclusions
TVT is the most prevalent neoplasia of the external genitalia of the dog in tropical and sub-tropical areas. The most frequent owner’s complaint is the hemorrhagic discharge. Diagnosis is based on typical physical and cytological findings. Weekly IV vincristine administration has been shown to be the most effective and practical therapy. Further experimental studies, carried out in larger groups of dogs, are necessary to investigate the changes in semen quality during vincristine treatment, and its long term effects on spermatogenesis and fertility. Until sufficient information on fertility effects becomes available, clinicians and owners must balance the potential benefits to the patient and the interest in using the animal for breeding.
Acknowledgements The authors thank Prof. Dr. Constantin Boscos (Clinic of Obstetrics and Artificial Insemination, Faculty of Veterinary Medicine, Aristotle University of Thessaloniki, Thessaloniki, Greece), for access to unpublished information on TVT and the text of his presentation on CVT at the 2004 WSAVA Congress in Rhodes, Greece [44]. References
1. Calvet CA. Transmissible venereal tumor in the dog. In: Kirk RW, ed. Current veterinary therapy VIII. Philadelphia: WB Saunders Co, 1983; 413-415.
2. Rogers KS. Transmissible venereal tumor. Comp Contin Educ Pract Vet 1997; 19(9):1036-1045.
3. Dominguez-Tejerina JC, Peña V, Anel L, et al. Tumor Venéreo transmisible. Arch Reprod Anim 1996; (1):42-47.
4. Cohen D. The biological behavior of TVT in immunosuppressed dogs. Eur J Cancer 1973; 3:163-164.
5. Richardson RC. Canine transmissible veneral tumor. Comp Contin Educ Pract Vet 1981; 3:951-956.
6. Cockrill JN, Beasly JN. Ultra structural characteristics of canine transmissible veneral tumor various stages of growth and regression. Am J Vet Res 1975; 36(5):677-681.
7. Cohen D. The canine transmissible venereal tumor: A unique result of tumor progression. Adv Cancer Res 1985; 43:75-112.
8. Johnston SD. Performing a complete canine semen evaluation in a small animal hospital. Vet Clin North Am Small An Pract 1991; 21(3):545-551.
9. Vermooten MI. Canine transmissible venereal tumor (TVT): a review. J S Afr Vet Assoc 1987; 58(3):147-150.
10. Lombard CH, Cabanie P. Le sarcome de Sticker. Rev Med Vet 1968; 119(6):565-586.
11. Moulton JE. Tumor of genital systems. In: Moulton JE, ed. Tumors in domestic animals. 2.ed. California: University of California, 1978; 326-330.
12. Yang TJ. Immunobiology of a spontaneously regressive tumor, the canine transmissible venereal sarcoma (Review). Anticancer Res 1988; 8:93-96.
13. Brown NO, MacEwen EG. Calvert CA. Transmissible venereal tumor in the dog. California Vet 1981; 3:6-10.
14. Krouger D, Grey RM, Boyd JW. An unusual presentation of canine transmissible venereal tumor. Canine Pract 1991; 16(6):16-21.
15. Tinucci-Costa M. Tumor venéreo canino - um caso de localização em ouvido externo. In: Anais do 14? Encontro de Pesq Vet 1992; 128.
16. Tinucci-Costa M, Souza FF de, Léga E, et al. A punção de medula é importante no prognóstico do tumor venéreo transmissível canino. J Braz Pathol Suppl 1997; 33:143.
17. Yang TJ, Chandler JP. Dependent expression of MHC antigens on the canine transmissible venereal sarcoma. Br J Cancer 1987; 55:131-134.
18. Palker TJ, Yang TJ. Detection of immune complexes in sera of dogs with canine transmissible veneral sarcoma (CTVS) by conglutinin-binding assay. J Comp Pathol 1985; 95:247-258.
19. Hill DL, Yang TJ, Wachtel A. Canine transmissible venereal sarcoma: tumor cell and infiltrating leukocyte ultra structure at different growth stages. Vet Pathol 1984; 21:39-45.
20. Yang TJ, Roberts RS, Jones JB. Quantitative study of lymphoreticular infiltration into canine transmissible venereal sarcoma. Virchows Arch B Cell Pathol 1976; 20:197-204.
21. Yang TJ, Palker TJ, Harding MW. Tumor size, leukocyte adherence inhibition and serum levels of tumor antigen in dogs with the canine transmissible venereal sarcoma. Cancer Immunol Immunoth 1991, 33:255-256.
22. Aprea, A N, Allende M G, Idiard R. Tumor Venéreo Transmisible Intrauterino: descripción de un caso. Vet Argentina XI 1994; 103:192-194.
23. Tasqueti UI, Martins MIM, Boselli CC, et al. Um caso atípico de TVT com deslocamento cranial de vagina. Anais do XX Congresso da ANCLIVEPA 1999; 38.
24. Johnson CA. Infecções genitais e tumor venéreo transmissível. In: Nelson RW, Couto CG, eds. Fundamentos de Medicina Interna de Pequenos Animais. Rio de Janeiro: Guanabara Koogan, 1994; 525.
25. Tinucci-Costa M. Tumor venéreo transmissível: estudos imunohistoquímicos e de transplantações xenogênicas e alogênicas. Ph D Thesis Faculty of Medicine. San Pablo University, Ribeirão Preto, 1999; 144.
26. Higgins DA. Observations on the canine transmissible venereal tumor as seen in the Bahamas. Vet Rec 1966; 79(3):67-71.
27. Daleck CLM, Ferreira HI, Daleck CR, et al. Novos estudos sobre o tratamento do tumor venéreo transmissível canino. Ars Vet 1987; 3(2):203-209.
28. Bradley RL. Tumores vulvovaginais. In: Borjab, MJ, ed. Técnicas atuais em cirurgia de pequenos animais. 3ed. São Paulo: Ed Roca, 1996; 385-387.
29. Weir EC, Pond MJ, Duncan JR, et al. Extragenital located TVT tumor in the dog. Literature review and case reports. J Am Anim Hosp Assoc 1987; 14:532-536.
30. Mc Evoy GK. American Hospital Formulary Service Drug information. In: Bethesda, MD. American Society of Hospital and Pharmacists; 1987.
31. Calvet CA, Leifer CE; McEwen EG. Vincristine for the treatment of Transmissible Venereal Tumor in the dog. J Am Vet Med Assoc 1982; 181(2):163-164.
32. Withrow SJ, McEwen EG. Small animal clinical oncology. 2 ed. Philadelphia: WB Saunders Co, 1996.
33. Rosenthal RC. Clinical application of Vinea alkaloids. J Am Vet Med Assoc 1981; 179(11):1084-1086.
34. Daleck CR, Francheschini PH, Padilha Filho JG, et al. Análise histológica de testículos e sêmen de cães submetidos a administração de sulfato de vincristina. Braz J Vet Res Anim Sci 1995; 32(1):51-56.
35. Freshman, J.M. Drugs affecting fertility in the male dog. In: Kirk RW ed. Current Veterinary Therapy X. Philadelphia: WB Saunders, 1989; 1224-1227.
36. Zhang Y, Sun K. Unscheduled DNA synthesis induced by the antitumor drug vincristine in germ cells of the male mice. Mutat Res 1992; 281(1):25-29.
37. Bueno R, Costa EP, Guimarães JD, et al. Infertilidade associata a espermatogenesis imperfecta no cao- Relato de um caso. Rev Bras Reprod Anim 1999; 23(3):460-461.
38. Saratsis Ph, Ypsilantis P, Tselkas K. Semen quality during vincristine treatment in dogs with transmissible venereal tumor. Theriogenology 2000; 53:1185-1192.
39. Amann RP. Detection of alteration in testicular and epididymal function in laboratory animals. Environment Health Perspective 1986; 170:149.
40. Feldman EC, Nelson RW eds. Clinical and Diagnostic Evaluation of the Male Reproductive Tract. In: Canine and Feline Endocrinology and Reproduction 2ed. Philadelphia: W.B Saunders, 1996; 673-690.
41. Gobello C, Corrada Y. Effects of vincristine treatment on semen quality in a dog with a TVT. J Small Anim Pract 2002; 43:416-417.
42. Amber EI, Henderson RA, Adeyanju JB, et al. Single-drug chemotherapy of canine transmissible veneral tumor with cyclophosphamide, methotrexate, or vincristine. J Vet Intern Med 1990; 4(3):144-147.
43. Souza FF de, Tinucci-Costa M, Faria Jr D, et al. Doxorubicin treatment for recurrent canine transmissible veneral tumor. In: Proceedings of the XXIII Congress of the World Small Anim Vet Assoc 1998; 772.
44. Boscos, CM, Ververidis, HN. Canine TVT: Clinical findings, diagnosis and treatment. Sci.Proc WSVA-FECAVA-HVMS World Congress, Rhodes, Greece, 2004; (2):758-761.
All rights reserved. This document is available on-line at www.ivis.org. Document No. A1233.0405.
Blood Recipient Stories Suzi's story: "I was the recipient of a blood transfusion two years ago. Our baby girl was delivered two months early by paramedics in the back of an ambulance as we were on our way to the hospital. Once we got to the hospital, I had some compli-cations and was taken into surgery the next day. Before my surgery I was given a blood transfusion. I was releas
Siemens Healthcare Diagnostics, the leading clinical diagnostics company, is committed to providing clinicians with the vital information they need for the accurate diagnosis, treatment and monitoring of patients. Our comprehensive portfolio of performance-driven systems, unmatched menu offering and IT solutions, in conjunction with highly responsive service, is designed to streamline workflow, en




 In: Recent Advances in Small Animal Reproduction, Concannon P.W., England G., Verstegen III J.
In: Recent Advances in Small Animal Reproduction, Concannon P.W., England G., Verstegen III J. 

 Figure 3c. Transmissible venereal tumor in the cranial vagina of a 3 year old, crossbreed bitch. Excised genital tract. - To view this image in full size go to the IVIS website at www.ivis.org . -
Although TVT has a cosmopolitan distribution, it is most frequently encountered in tropical and subtropical zones [2]. In South America it is commonly found in urban areas with large populations of free-roaming dogs. The current review is based on the experience of the authors in Brazil and Argentina, and on relevant publications [1-44].
Etiopathology
Figure 3c. Transmissible venereal tumor in the cranial vagina of a 3 year old, crossbreed bitch. Excised genital tract. - To view this image in full size go to the IVIS website at www.ivis.org . -
Although TVT has a cosmopolitan distribution, it is most frequently encountered in tropical and subtropical zones [2]. In South America it is commonly found in urban areas with large populations of free-roaming dogs. The current review is based on the experience of the authors in Brazil and Argentina, and on relevant publications [1-44].
Etiopathology 
 express both antigens. This difference may be responsible for the additional immune response of the host, accelerating the regression of the tumor [12,17].
Differences in cell types have also been found between stages of tumor progression. Tumors in progressive growth have round cells with microvilli while regressing tumors present transitional rather fusiform cells. Moreover, regressing tumors have a high number of T lymphocytes [19,20]. It is thought that substances secreted by the lymphocyte infiltrate are responsible for the tumor’s regression by inducing cellular differentiation [12,20,21].
Gross and Microscopic Characteristics
express both antigens. This difference may be responsible for the additional immune response of the host, accelerating the regression of the tumor [12,17].
Differences in cell types have also been found between stages of tumor progression. Tumors in progressive growth have round cells with microvilli while regressing tumors present transitional rather fusiform cells. Moreover, regressing tumors have a high number of T lymphocytes [19,20]. It is thought that substances secreted by the lymphocyte infiltrate are responsible for the tumor’s regression by inducing cellular differentiation [12,20,21].
Gross and Microscopic Characteristics 
 three weeks with sporadic success [8]. Recurrences have been described after immunotherapy using Staphylococcus protein A, BCG or a vaccine made from tumoral cells [2,42]. Biotherapy has unfortunately also resulted in a high rate of recurrence [5,9,42].
Chemotherapy has been shown to be the most effective and practical therapy, with vincristine sulfate being the most frequently used drug [31]. Vincristine (Oncovin®, Lily), is administered weekly at a dose of 0.5 to 0.7 mg/m2 of body surface area or 0.025 mg/kg, IV [7,24]. The involution of the lesions is gradual, although it is particularly noticeable and significant at the beginning of the treatment. Complete remission usually takes 2 to 8 injections [27,31] and occurs in more than 90% of the treated cases (unpublished observation). A cure rate approaching 100% is achieved in cases treated in the initial stages of progression, especially in cases of less than 1 year duration, and independent of the presence or not of metastases [44]. In cases of longer duration, longer periods of therapy are required, and the cure rate is lower [44]. Side effects can be expected. Cytostatic agents, such as vincristine, can cause myelosuppression and gastrointestinal effects resulting in leukopenia and vomiting in 5 to 7% of the patients. Paresis has also been described as a side effect due to peripheral neuropathy [31,32]. A complete white blood cell count is, therefore, recommended prior to each administration. When the white blood cell count is below 4,000 mm3 further administration should be delayed 3 to 4 days and the dose of vincristine can be reduced to 25% of the initial dose [1]. The most frequent complication of vincristine treatment is the occurrence of local tissue lesions caused by extravasation of the drug during IV application resulting in the development of necrotic lesions with crusts (Fig. 7a and Fig. 7b).
Figure 7a. Necrotic skin lesion caused by perivascular leakage of vincristine sulfate. Seven days after application. - To view this image in full size go to the IVIS website at www.ivis.org . -
Figure 7b. Necrotic skin lesion caused by perivascular leakage of vincristine sulfate. Fifteen days after application. - To view this image in full size go to the IVIS website at www.ivis.org . -
Other chemotherapeutic agents indicated for TVT treatment include cyclophosphamide (5 mg/kg, PO, for 10 days as a single drug therapy or given in association with prednisolone, 3 mg/kg, for 5 days); also, weekly vinblastine (0.1 mg/kg, IV during 4 to 6 weeks), methotrexate (0.1 mg/kg, PO, every other day) or a combination of the 3 drugs. However, there is no apparent advantage in the combination of chemotherapy over using vincristine alone [5,9,13,21].
Resistant cases can be treated with doxorubicin (Adriamycin®, Adria Lab, 30 mg/m2, IV, with 3 applications every 21 days) [5,43]. When total disappearance of the tumor cannot be achieved by chemotherapy, electro-cauterization or cryo-cauterization can be useful [2,9]. After therapy, small remnant lesions can disappear spontaneously after 1 or 2 weeks (unpublished observations). In cases that fail to resolve with chemotherapy, radiotherapy has been reported to yield good results [44].
Effects of Vincristine Treatment on Spermatogenesis
three weeks with sporadic success [8]. Recurrences have been described after immunotherapy using Staphylococcus protein A, BCG or a vaccine made from tumoral cells [2,42]. Biotherapy has unfortunately also resulted in a high rate of recurrence [5,9,42].
Chemotherapy has been shown to be the most effective and practical therapy, with vincristine sulfate being the most frequently used drug [31]. Vincristine (Oncovin®, Lily), is administered weekly at a dose of 0.5 to 0.7 mg/m2 of body surface area or 0.025 mg/kg, IV [7,24]. The involution of the lesions is gradual, although it is particularly noticeable and significant at the beginning of the treatment. Complete remission usually takes 2 to 8 injections [27,31] and occurs in more than 90% of the treated cases (unpublished observation). A cure rate approaching 100% is achieved in cases treated in the initial stages of progression, especially in cases of less than 1 year duration, and independent of the presence or not of metastases [44]. In cases of longer duration, longer periods of therapy are required, and the cure rate is lower [44]. Side effects can be expected. Cytostatic agents, such as vincristine, can cause myelosuppression and gastrointestinal effects resulting in leukopenia and vomiting in 5 to 7% of the patients. Paresis has also been described as a side effect due to peripheral neuropathy [31,32]. A complete white blood cell count is, therefore, recommended prior to each administration. When the white blood cell count is below 4,000 mm3 further administration should be delayed 3 to 4 days and the dose of vincristine can be reduced to 25% of the initial dose [1]. The most frequent complication of vincristine treatment is the occurrence of local tissue lesions caused by extravasation of the drug during IV application resulting in the development of necrotic lesions with crusts (Fig. 7a and Fig. 7b).
Figure 7a. Necrotic skin lesion caused by perivascular leakage of vincristine sulfate. Seven days after application. - To view this image in full size go to the IVIS website at www.ivis.org . -
Figure 7b. Necrotic skin lesion caused by perivascular leakage of vincristine sulfate. Fifteen days after application. - To view this image in full size go to the IVIS website at www.ivis.org . -
Other chemotherapeutic agents indicated for TVT treatment include cyclophosphamide (5 mg/kg, PO, for 10 days as a single drug therapy or given in association with prednisolone, 3 mg/kg, for 5 days); also, weekly vinblastine (0.1 mg/kg, IV during 4 to 6 weeks), methotrexate (0.1 mg/kg, PO, every other day) or a combination of the 3 drugs. However, there is no apparent advantage in the combination of chemotherapy over using vincristine alone [5,9,13,21].
Resistant cases can be treated with doxorubicin (Adriamycin®, Adria Lab, 30 mg/m2, IV, with 3 applications every 21 days) [5,43]. When total disappearance of the tumor cannot be achieved by chemotherapy, electro-cauterization or cryo-cauterization can be useful [2,9]. After therapy, small remnant lesions can disappear spontaneously after 1 or 2 weeks (unpublished observations). In cases that fail to resolve with chemotherapy, radiotherapy has been reported to yield good results [44].
Effects of Vincristine Treatment on Spermatogenesis  34. Daleck CR, Francheschini PH, Padilha Filho JG, et al. Análise histológica de testículos e sêmen de cães submetidos a administração de sulfato de vincristina. Braz J Vet Res Anim Sci 1995; 32(1):51-56.
35. Freshman, J.M. Drugs affecting fertility in the male dog. In: Kirk RW ed. Current Veterinary Therapy X. Philadelphia: WB Saunders, 1989; 1224-1227.
36. Zhang Y, Sun K. Unscheduled DNA synthesis induced by the antitumor drug vincristine in germ cells of the male mice. Mutat Res 1992; 281(1):25-29.
37. Bueno R, Costa EP, Guimarães JD, et al. Infertilidade associata a espermatogenesis imperfecta no cao- Relato de um caso. Rev Bras Reprod Anim 1999; 23(3):460-461.
38. Saratsis Ph, Ypsilantis P, Tselkas K. Semen quality during vincristine treatment in dogs with transmissible venereal tumor. Theriogenology 2000; 53:1185-1192.
39. Amann RP. Detection of alteration in testicular and epididymal function in laboratory animals. Environment Health Perspective 1986; 170:149.
40. Feldman EC, Nelson RW eds. Clinical and Diagnostic Evaluation of the Male Reproductive Tract. In: Canine and Feline Endocrinology and Reproduction 2ed. Philadelphia: W.B Saunders, 1996; 673-690.
41. Gobello C, Corrada Y. Effects of vincristine treatment on semen quality in a dog with a TVT. J Small Anim Pract 2002; 43:416-417.
42. Amber EI, Henderson RA, Adeyanju JB, et al. Single-drug chemotherapy of canine transmissible veneral tumor with cyclophosphamide, methotrexate, or vincristine. J Vet Intern Med 1990; 4(3):144-147.
43. Souza FF de, Tinucci-Costa M, Faria Jr D, et al. Doxorubicin treatment for recurrent canine transmissible veneral tumor. In: Proceedings of the XXIII Congress of the World Small Anim Vet Assoc 1998; 772.
44. Boscos, CM, Ververidis, HN. Canine TVT: Clinical findings, diagnosis and treatment. Sci.Proc WSVA-FECAVA-HVMS World Congress, Rhodes, Greece, 2004; (2):758-761.
All rights reserved. This document is available on-line at www.ivis.org. Document No. A1233.0405.
34. Daleck CR, Francheschini PH, Padilha Filho JG, et al. Análise histológica de testículos e sêmen de cães submetidos a administração de sulfato de vincristina. Braz J Vet Res Anim Sci 1995; 32(1):51-56.
35. Freshman, J.M. Drugs affecting fertility in the male dog. In: Kirk RW ed. Current Veterinary Therapy X. Philadelphia: WB Saunders, 1989; 1224-1227.
36. Zhang Y, Sun K. Unscheduled DNA synthesis induced by the antitumor drug vincristine in germ cells of the male mice. Mutat Res 1992; 281(1):25-29.
37. Bueno R, Costa EP, Guimarães JD, et al. Infertilidade associata a espermatogenesis imperfecta no cao- Relato de um caso. Rev Bras Reprod Anim 1999; 23(3):460-461.
38. Saratsis Ph, Ypsilantis P, Tselkas K. Semen quality during vincristine treatment in dogs with transmissible venereal tumor. Theriogenology 2000; 53:1185-1192.
39. Amann RP. Detection of alteration in testicular and epididymal function in laboratory animals. Environment Health Perspective 1986; 170:149.
40. Feldman EC, Nelson RW eds. Clinical and Diagnostic Evaluation of the Male Reproductive Tract. In: Canine and Feline Endocrinology and Reproduction 2ed. Philadelphia: W.B Saunders, 1996; 673-690.
41. Gobello C, Corrada Y. Effects of vincristine treatment on semen quality in a dog with a TVT. J Small Anim Pract 2002; 43:416-417.
42. Amber EI, Henderson RA, Adeyanju JB, et al. Single-drug chemotherapy of canine transmissible veneral tumor with cyclophosphamide, methotrexate, or vincristine. J Vet Intern Med 1990; 4(3):144-147.
43. Souza FF de, Tinucci-Costa M, Faria Jr D, et al. Doxorubicin treatment for recurrent canine transmissible veneral tumor. In: Proceedings of the XXIII Congress of the World Small Anim Vet Assoc 1998; 772.
44. Boscos, CM, Ververidis, HN. Canine TVT: Clinical findings, diagnosis and treatment. Sci.Proc WSVA-FECAVA-HVMS World Congress, Rhodes, Greece, 2004; (2):758-761.
All rights reserved. This document is available on-line at www.ivis.org. Document No. A1233.0405.