Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Sm full programme & abstracts 2011.indd
1971 - 2011 British Society for Antimicrobial Chemotherapy SPRING MEETING 2011 Wednesday 23 March Hall 5, The ICC, Birmingham Celebrating 40 Years of Achievement Programme & poster abstracts CPD ACCREDITED EXHIBITORS
The Society is grateful for the support it has received from industry
and wishes to acknowledge the following companies:
Exhibitors Sponsors Contents Programme 3 Posters The treatment of glue ear using high dose antibiotics and mucolytics - In-vitro
Al-Zahid S, Daniel M, Ashraf W, Fortnum H, Fergie N, Shakesheff K, Birchall JP, Bayston R
Susceptibility testing by the agar diff usion method and the eff ect of nisin on mupirocin-resistant MRSA
Boyan B. Bonev1, Alan Cockayne2, Erin Brown1, David C. Griffi
Biological profi ling of new vancomycin derivatives with potent activity against superbugs
Cooper, M, Ramu, S., Cheng, M., Daud, N.H., Huang, J.X., Gong, Y. & Butler, M.S. Clinical experience with daptomycin for the treatment of bacteraemia in the United Kingdom: 2007-2011
Gonzalez-Ruiz A, Galloway A, on behalf of the UK EU-CORE group
Current Clinical Use of Daptomycin in the UK from the European Cubicin® Outcomes Registry and Experience (EU-CORE), 2007-2010 Gonzalez-Ruiz A, Galloway A, Seaton RA, Sarma J, Guleri A on behalf of the UK EU-CORE group Treatment of infective endocarditis with daptomycin: 3 year UK registry experience
Gonzalez-Ruiz A and Guleri A on behalf of the UK EU-CORE group
Treatment of osteoarticular infections with daptomycin: UK Experience
Gonzalez-Ruiz A and Seaton RA on behalf of the UK EU-CORE group
Treatment of skin and soft tissue infections with daptomycin: UK Experience
Gonzalez-Ruiz A, Seaton RA and Sarma J on behalf of the UK EU-CORE group
Clostridium diffi orthopaedic problem? A comparison of empirical antibiotic prescribing in Infectious Diseases Units in Sheffi eld, UK and Rome, Italy
Johnson E*, Prtak L, Di Bella S, Petrosillo N
Audit of infection control practices for the control of multi-drug resistant gram-negative bacilli
Jones Dr, L; Price, J; Davies, D; Dr Lewis, A and Dr Berry, N
Is Helicobacter pylori antibiotic resistance surveillance needed and how can it be delivered? A feasibility study in three UK centres. Lasseter G,1 Shaw I,2 Lawson, A,3 D’Arcy S,4 Glocker E,5 and McNulty C1 e-Bug: Evaluation of a hygiene and prudent antibiotic use educational pack in the Czech Republic, France and England
Lecky DM1, Weinberg J2, Verlander N3, Touboul P4 and Benes J5 and McNulty CAM1 on behalf of the e-Bug working group
Evaluation of a Novel AmpC Detection Method Kit to Detect all Types of AmpC Production On-line survey of Medicines Managers to determine how antibiotic stewardship is being promoted in Primary Care Trusts 11 McNulty CAM1, Guise T2, Turner K1, Hand K3, Howard P4, Dryden M5, Cooke J6 Partnership Programme to reduce Health Care Associated Infections (HCAIs) in a Developing Country An analysis of bacteraemia caused by gram negative Extended Spectrum Beta Lactamase producers (ESBLp) at Darent 13 Valley Hospital Patel R*, Bassi P†, Enayat M**, Cotter L†, Gonzalez-Ruiz A† Point Prevalence Survey of Antibiotic Use in Trusts in the North West of England 14 Shatwell J, Oates K Surveillance of antimicrobial use and resistance in Scotland – monitoring the impact of national antimicrobial stewardship 15 Wiuff , C. Malcolm, W., Wilson, J., Cromwell, T., Bennie, M. and Eastaway, A., on behalf of the Scottish Antimicrobial Prescribing Group Epidemiology of Stenotrophomonas maltophilia bacteraemia in a tertiary hospital (Wythenshawe Hospital experience) 16 Zhou A.Y & I. A. Hassan
British Society for Antimicrobial Chemotherapy
SPRING MEETING 2011 Wednesday 23 March The ICC, Birmingham Celebrating 40 Years of Achievement PROGRAMME 0900 - 0940 Session one: National methods and surveillance Chair: Professor Ian Phillips, Malaga
BSAC antimicrobial susceptibility testing - from Stokes to European harmonization
Antimicrobial resistance surveillance, improving relevance and outputs
Professor Alasdair MacGowan, Bristol
Antimicrobial stewardship - a tool for improving outcomes?
Resistance in farm animals - implications for animal and public health
Jeff Jones, Veterinary Laboratories AgencySession two: Challenges and prospects: what now for multi-drug resistant infections? Chair: Professor Richard Wise, Birmingham
Multi-drug resistant Escherichia coliProfessor Peter Hawkey, BirminghamThe Garrod Lecture:
My 40 years - from penicillin-binding proteins to molecular epidemiology
Session three: 20th - 21st century practice Chair: Professor Laura Piddock, Birmingham
Antimicrobial chemotherapy in practice from 20th to 21st century - throughout my
Professor Alasdair Geddes, BirminghamSession four: What next for antimicrobial therapy?
A view from industry, antibiotics - past, present and prospects for the future?
Richard Bax, TranScrip Partners, ReadingProfessor Laura Piddock, BirminghamBSAC Spring Meeting 2011 Poster Abstracts The treatment of glue ear using high dose antibiotics and mucolytics - In-vitro Al-Zahid S, Daniel M, Ashraf W, Fortnum H, Fergie N, Shakesheff K, Birchall JP, Bayston R University of Nottingham
Background: Recent evidence that otitis media with eff usion (OME) is the result of a biofi lm infection may explain the high rate of recurrence after conventional treatment with grommets.
Objectives: We aimed to test the in-vitro effi
cacy of antibiotics (Clindamycin and Rifampicin) and mucolytics
(N-acetylcysteine) in eradicating middle ear biofi lms using an OME biofi lm model in the laboratory.
Design and methods: Staphylococcus aureus biofi lms of an OME origin were grown on silicone discs. Biofi lms were exposed to various combinations of N-acetylcysteine, Rifampicin and Clindamicin for diff erent time periods. Antibiotic concentrations of 100 and 1000 MIC were used (MIC; minimum inhibitory concentration needed to inhibit bacteria in free planktonic state). 5 times the MIC of N-acetylcysteine was used.
Results: It took 3 weeks to eradicate biofi lms using antibiotics even at 1000MIC. N-acetylcysteine alone took 7 days to eradicate biofi lms. However, combination therapy of N-acetylcysteine with 1000MIC of Clindamycin + Rifampicin eradicated biofi lms in 24 hours.
Conclusion: Combination therapy of N-acetylcysteine with antibiotics seems to be eff ective in eradicating biofi lms. Delivering combination therapy by controlled-release biodegradable polymers directly into the middle ear is now being explored as a potential novel strategy to combat OME. Susceptibility testing by the agar diff usion method and the eff ect of nisin on mupirocin-resistant MRSA Boyan B. Bonev1, Alan Cockayne2, Erin Brown1, David C. Griffi 1School of Biomedical Sciences, University of Nottingham; 2School of Molecular Medical Sciences, University of Nottingham
Abstract: Objectives: A theoretical description of the agar diff usion assay is discussed that takes into consideration loss of antibiotic during diff usion and provides higher accuracy of the MIC determined from the assay. The method is tested on a number of widely used compounds, as well as on lanthionine antibiotic nisin. The tolerance of some clinical strains of MRSA to mupirocin is also discussed and the ability of nisin to inhibit growth of high-level (MIC ≥ 256 mg/L) mupirocin-resistant MRSA strains (MupR-MRSA) is assessed.
Methods: Agar diff usion assays are discussed and used on model organism, B. subtilis. Broth dilution technique is also used to assess the tolerance of MRSA strains to mupirocin.
Results: A theory for analysis of antibiotic diff usion in solid media is described, in which we consider possible interactions of the test antibiotic with the solid medium or partial antibiotic inactivation during diff usion. This is particularly relevant to the analysis of diff usion of hydrophobic or amphipathic compounds, including nisin. The model is based on a generalized diff usion equation, which includes the existing theory as a special case and contains an additional, dissipative term. MupR-MRSA were inhibited by concentrations of nisin similar to those inhibiting MSSA. Furthermore, nisin/mupirocin combinations were highly synergistic against MupR-MRSA.
Conclusions: The accuracy of interpretation of data obtained by the agar diff usion method benefi ts from consideration of the dissipative nature of the diff usion process with nisin as a particular example. Further studies are warranted to assess the use of nisin in combination with mupirocin for decolonisation of MupR-MRSA. Biological profi ling of new vancomycin derivatives with potent activity against superbugs Cooper, M, Ramu, S., Cheng, M., Daud, N.H., Huang, J.X., Gong, Y. & Butler, M.S. Institute for Molecular Biosciences, The University of Queensland
The lack of treatments available to treat various multi-drug resistant bacteria is one of the most pressing health issues currently facing humankind. In particular, serious problems have been encountered when treating the ‘ESKAPE’ pathogens (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa and Enterobacter species), which are responsible for most hospital-based infections.1
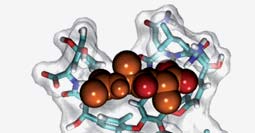
Our group has been developing new vancomycin derivatives for the treatment of community-acquired and nosocomial Gram-positive complicated skin and skin structure infections (cSSSI) and pneumonia (CAP/NP) caused in particular by Staphylococcus aureus, Enterococcus sp. and Streptococcus pneumoniae. Our initially synthesised compounds are 10- to 100-fold more active than vancomycin, are bactericidal and act by additional modes of action. This poster will describe the initial microbiological evaluation of these compounds against a series of multi-drug resistance pathogens, as well as presenting data that shows these compounds to have favourable in vitro cytotoxicity, haemolysis and human plasma stability. In addition, we will present preliminary results from our mode of action studies, which include bacterial membrane permeability assays, binding studies using UV absorbance and isothermal titration calorimetry, and microscopy.
Figure 1: Vancomycin binding to Ac-D-Ala-D-Ala subunit of Lipid II
References:1. Boucher H. W.; Talbot, G. H.;, Bradley J. S.; Edwards, J. E.;, Gilbert D.;, Rice LB.;, et al. Bad Bugs, No Drugs: No ESKAPE! An Update from the Infectious Diseases Society of America. Clin. Infect. Dis. 2009, 48, 1-12. Clinical experience with daptomycin for the treatment of bacteraemia in the United Kingdom: 2007-2010 Gonzalez-Ruiz A, Galloway A, on behalf of the UK EU-CORE group
Background: Daptomycin (DAP) was fi rst licensed in the UK in 2006 for the treatment of complicated skin and soft tissue infections (cSSTIs) and Staphylococcus aureus bacteraemia (SAB) with or without infective endocarditis (IE). Since that time data on the use of DAP has been collected in the patient registry European Cubicin® Outcomes Registry and Experience (EU-CORESM).
Methods: A retrospective, non-interventional records review of pts with bacteraemia receiving DAP from 13 participating UK institutions for the fi rst three reporting periods of EU-CORE, Sep 2007 to Aug 2010. Effi
Results: 9 of the 13 centres treated116 pts with bacteraemia. 58% were male. The mean age of pts was 60 years. The majority of pts (97%) had signifi cant underlying diseases. 52% of pts had received prior antibiotics of which 50% had received β-lactams/β-lactam combinations. 68% of pts received concomitant antibiotics whilst on DAP. The most frequently isolated pathogens were coagulase-negative staphylococci (28%) and S. aureus (24%). The initial dose of DAP was 6 mg/kg in 69% of pts and 4 mg/kg in 17%. Mean time to clinical improvement was 4 days. Mean duration of therapy was 8.5 days. Overall clinical outcomes were success (defi ned as ‘cure or improved’) in 66%, failure in 16% and non-evaluable in 18% of pts. Adverse events regardless of study drug relationship were reported in 33% of pts, (38/116). 8 pts discontinued therapy because of an adverse event.
Conclusions: DAP has an important role as fi rst-line therapy for Gram-positive bacteraemia, and may also be eff ective when other antibiotics have failed. These data may support the use earlier use of DAP in pts with suspected Gram-positive bacteraemia, with cSSTIs or endocarditis, prior to blood culture results being obtained. Current Clinical Use of Daptomycin in the UK from the European Cubicin® Outcomes Registry and Experience (EU-CORE), 2007-2010 Gonzalez-Ruiz A, Galloway A, Seaton RA, Sarma J, Guleri A on behalf of the UK EU-CORE group
Background: Daptomycin (DAP), the fi rst in class of cyclic lipopeptide antibiotics, received marketing authorisation in Europe in Jan 2006.
Objective: To describe the current “real world” clinical experience with DAP in the UK.
Methods: A retrospective, non-interventional records review of pts receiving DAP in 13 institutions for the fi rst three reporting periods of EU-CORE, Sep 2007 to Aug 2010. Effi
cacy was evaluated by the investigator at end of DAP therapy.
Results: Out of 485 pts 54% were male. The mean age of pts was 62.5 years. The majority of pts (90%) had signifi cant underlying diseases. Primary infections were bacteraemia 22%, complicated skin and soft tissue infections (SSTI) 21%, uncomplicated SSTI 16%, endocarditis 12%, foreign body/prosthesis 10% and osteomyelitis 7%. DAP was used as second-line therapy in 69% of pts, following therapy with β-lactams (in 21%) or glycopeptides (6%). 59% of pts received concomitant antibiotics. DAP was used empirically in 50% of pts and MRSA infection was suspected in 20% of pts. Primary cultures were obtained for 90% of pts. The most frequent species were S. aureus (28%), and coagulase-negative staphylococci (12%). The initial dose of DAP was 6 mg/kg in 51% of pts and 4 mg/kg in 34%. Outpatient DAP therapy was received by 24% of pts. Overall clinical outcomes were success, defi ned as ‘cure or improved’, in 74%, failure in 10% and non-evaluable in 16% of pts. Adverse events regardless of study drug relationship were reported in 23% of pts, (113/485).
Conclusions: This report confi rms results from randomized trials. It demonstrates the benefi ts of DAP in the treatment of a wide range of infections, including a large proportion of older pts with signifi cant comorbidities. DAP therapy was eff ective and safe achieving high overall success rates. The most frequently treated infections were those for which DAP is indicated (bacteraemia and cSSTIs).
Treatment of infective endocarditis with daptomycin: 3 year UK registry experience Gonzalez-Ruiz A and Guleri A on behalf of the UK EU-CORE group
Objectives: We present the data from the fi rst 3 years of DAP use for the treatment of infective endocarditis (IE) in the UK.
Methods: 8 of the 13 UK institutions participating in the European Cubicin® Outcomes Registry and Experience (EU-CORESM) had treated patients (pts) with IE. Data were collected on demographics, antibiotic usage, microbiological and clinical outcomes and adverse events from pts treated between January 2006 and August 2010. Pts were categorised by severity and the anatomical site of the primary infection. All pts had received at least one dose of DAP. Outcomes were assessed by investigators as cured, improved, failure and non-evaluable.
Results: Of 66 pts (mean age of 60 yrs), 88% had signifi cant underlying disease. The majority (73%) were male and had left-sided IE (61%). Prior antibiotics had been received by 82% pts. DAP was used empirically in 30% of cases. Cultures were obtained for the primary infection in 96% pts. Staphylococcus aureus was the most frequent isolate (30%) followed by coagulase-negative staphylococci (11%). Mean duration of therapy was 21 days and 64% of pts received concomitant antibiotics. DAP 6 mg/kg 24h was the most frequently used dose (71%). Clinical outcomes were success, defi ned as ‘cure plus improved’ (74%), failure (6%) and non-evaluable (20%). Mean time to clinical improvement was 6 days. Adverse events (AE) were reported regardless of study drug relationship. 11% of pts discontinued therapy because of an AE.
Conclusions: Despite the number of prior antibiotic failures and multiple comorbidites in these pts, the overall clinical success rate in this UK population was 74%. From this series, there is emerging evidence that DAP is being used to treat infections caused by other Gram-positive species that are of increasing importance in IE, particularly where treatment options may be limited. These data add to the body of evidence for the effi
Treatment of osteoarticular infections with daptomycin: UK Experience Gonzalez-Ruiz A and Seaton RA on behalf of the UK EU-CORE group
Objective: To describe the UK specifi c clinical experience in patients with osteoarticular infections (including osteomyelitis and septic arthritis) treated with daptomycin (DAP) since marketing authorisation in January 2006. These data were taken from the 13 UK institutions participating in the European Cubicin® Outcomes Registry and Experience (EU-CORESM).
Methods: Data were collected on patient demographics, antibiotic usage, microbiological and clinical outcomes and adverse events from pts treated with DAP between January 2006 and August 2010. All pts included in the registry received at least one dose of DAP. Outcomes were assessed by investigators as cured, improved, failure and non-evaluable. All adverse events were recorded.
Results: Of 77 pts (mean 65 years), 75% had underlying disease, 44% had foreign body infections and 20% temporary or permanent prostheses. Prior antibiotics (predominantly beta-lactams or glycopeptides) were used in 82%. DAP was used after culture results in 71%. S. aureus (42%), S. epidermidis (13%) and coagulase-negative staphylococci (8%) were most frequently isolated. Mean duration of therapy was 10.5 days. 6 mg/kg 24h was the most frequently used dose, 44% had concomitant antibiotics and 55% received DAP as outpatients. Success (cure or improved) was observed in 91%, failure 3% (7% non-evaluable). 9% discontinued therapy because of an adverse event.
Conclusions: Overall clinical success rate of 91% in a complex pre-treated population demonstrates the utility of DAP in the management of osteoarticular infections. These data add to the evidence that DAP is a useful addition particularly in the outpatient setting, for the management of orthopaedic-related infections where other long-term treatment options may be limited.
Treatment of skin and soft tissue infections with daptomycin: UK Experience Gonzalez-Ruiz A, Seaton RA and Sarma J on behalf of the UK EU-CORE group
Objective: To describe the UK specifi c clinical experience in patients with complicated skin and soft tissue infections (cSSTIs) treated with daptomycin (DAP) since marketing authorisation in January 2006. These data were taken from all UK institutions (13) participating in the European Cubicin® Outcomes Registry and Experience (EU-CORESM).
Methods: EU-CORE is a retrospective, non-interventional records review evaluating outcomes of patients (pts) treated with DAP in Europe. Data were collected on patient demographics, antibiotic usage, microbiological and clinical outcomes and adverse events from pts treated with DAP between January 2006 and August 2010. All pts included in the registry received at least one dose of DAP. Outcomes were assessed by investigators as cured, improved, failure and non-evaluable. All adverse events were recorded.
Results: Data from 189 pts were collected from 12 of the 13 UK centres. 1 centre did not enter any pts with cSSTIs. All pts were included in the safety population. The majority pts (90%) had signifi cant underlying disease. 75% of pts had received prior antibiotics. 62% pts received an initial dose of 4 mg/kg, and 29% received 6 mg/kg. 50% of pts received concomitant antibiotics. Clinical outcomes were success (defi ned as ‘cure plus improved’) (78%), failure (9%) and non-evaluable (12%). The most frequently isolated pathogen was S. aureus (60/189) with none confi rmed as MRSA. Serious adverse events were reported regardless of study drug relationship and were experienced by 16% of pts. 7 pts (4%) discontinued therapy because of an adverse event.
Conclusions: DAP was used to treat a range of cSSTIs. DAP was frequently used as second-line therapy and also as concomitant antimicrobial therapy. The overall clinical success rate in this UK population was 78%. Clostridium diffi cile – an orthopaedic problem?
Houston R, Oates KCountess of Chester NHS Foundation Trust
Introduction: An outbreak of Clostridium diffi
cile was declared in the Trust in March 08. This led to a review of antibiotic
policies including antibiotic prophylaxis in orthopaedic surgery. The existing orthopaedic policy used intravenous (IV) cefuroxime 1.5g at induction followed by up to 2 post-operative doses. The Department of Health document “Clostridium diffi
cile infection: how to deal with the problem” recommended minimising use of broad-spectrum agents
such as cephalosporins, especially in elderly patients, and limiting surgical prophylaxis to a single dose. In May 09 the local policy for orthopaedic prophylaxis in trauma patients was changed to single doses of IV teicoplanin plus IV gentamicin.
Aim: To assess if the change in policy for prophylactic antibiotics used in orthopaedic surgery had reduced rates of Clostridium diffi
cile infection (CDI) in orthopaedic trauma patients.
Method: Cases of CDI from April 2008 to September 10 were reviewed. The numbers of cases reported on the orthopaedic trauma ward in the 12 months before and after the change in antibiotic policy were compared.
Results: In the 12 months prior to the change in antibiotic policy (May 08 to April 09), 22 cases of CDI were reported in patients on the orthopaedic trauma ward, compared to no cases in the 12 months following the policy change. In 16 months since the change in policy there have been a total of 4 cases of CDI reported on the orthopaedic trauma ward. There were no cases of CDI reported for patients on the elective orthopaedic ward in the data reviewed in the time period (April 08 to September 10).
Conclusion: There has been a signifi cant reduction in the rate of CDI in the elderly orthopaedic trauma patient group. This is likely to be attributable to a combination of improved hand hygiene, increased staff awareness of issues around CDI and regular audit of cleaning standards on wards but antibiotic prescribing is key. The policy in elective orthopaedic patients was left unchanged and IV cefuroxime (up to 3 doses of 1.5g) continues to be used for prophylaxis in these patients. As this group of patients is younger than the trauma group and there were no cases of CDI reported in this group from April 08 to date it is felt that a change in antibiotic policy is not necessary. This would need to be reviewed if an increase in CDI was observed in this patient group. A comparison of empirical antibiotic prescribing in Infectious Diseases Units in Sheffi eld, UK and Rome, Italy.
Johnson E*, Prtak L, Di Bella S, Petrosillo N Sheffi eld Teaching Hospitals Foundation Trust & National Institute of Infectious Diseases, Spallazani Hospital, Rome, Italy
Objectives: In the UK, concerns over Clostridium diffi
cile are limiting use of some antibiotics but this is not necessarily
mirrored in Europe. We prospectively compared usage of antibiotics prescribed in Infectious Diseases Units over the same 2 week period in Sheffi
Methods: We collected antibiotic prescribing data for all patients admitted to the above Infectious Diseases units from 18th to 29th October 2010. Data was collected concurrently by an independent observer and included diagnosis, number of antibiotics and course length. All patients were followed to completion of antibiotic course where possible.
eld had a higher throughput of patients in the 2-week period (53 vs 30). However, a similar percentage of
patients received antibiotics (70% in Sheffi
eld, 66% in Rome). The groups were similar in age but diff ered in ethnicity. The
commonest reason for antibiotics in both groups was a respiratory source. In Sheffi
was suspected meningitis or cellulitis (6 and 5 patients respectively) with relatively fewer in Rome (1 and 0). The median number of days of antibiotics was the same in both groups (12 days) but the range of antibiotics in Sheffi
from 5 to > 90 days i.e. ongoing treatment; compared with 3 to 35 days in Rome. There were more deep site infections such as pulmonary abscesses, discitis, infected DVTs in Sheffi
eld which may explain this. The commonest empirical
antibiotics for any type of infection in Rome were 3rd generation cephalosporins, mainly ceftriaxone, compared to Sheffi
eld in which co-amoxiclav was preferentially used except where meningitis was suspected (6 patients). Sheffi
also had a far higher usage of amoxicillin, benzylpenicillin and fl ucloxacillin, which were not prescribed at all in Rome during this short study.
Conclusion: Antibiotic stewardship and bacterial resistance rates are known to vary across Europe. Although small, our ‘snapsnot’ shows a clear diff erence in empirical antibiotic choice. In the UK, more penicillin-based antibiotics are prescribed, in preference to 3rd generation cephalosporins perhaps refl ecting concerns about Clostridium diff risk. Furthermore, decreasing MRSA rates in the UK may explain the higher usage of fl ucloxacillin. It remains to be seen if prescribing practice in Italy will mirror these changes over the coming years. Audit of infection control practices for the control of multi-drug resistant gram-negative bacilli Dr Jones, L; Price, J; Davies, D; Dr Lewis, A and Dr Berry, N Public Health Wales Microbiology Abertawe Bro Morgannwg University Health Board, Singleton Hospital, Sgeti, Swansea,
Introduction: Multi-drug resistant gram negative bacteria (MDR GNB) can cause signifi cant morbidity and mortality and spread can occur in hospitals. Unlike for Clostridium diffi
cile and MRSA there are no national infection control guidelines
Aims: To investigate advice given to ward staff regarding control of MDR GNB by infection control nurses (ICNs), compliance with advice given and the reporting to ICNs by the microbiology laboratory.
Defi nitions: MDR GNB were defi ned as Enterobacteriaceae resistant to 1st, 2nd and 3rd generation cephalosporins or Pseudomonas aeruginosa and Acinetobacter sp resistant to at least 3 antibiotics of diff erent classes they are not intrinsically resistant to.
Methods: Over 4 weeks all MDR GNB reported to ICNs were identifi ed and advice given documented. Wards were contacted 24-72 hrs later to record extent of adherence to advice and reasons for non-compliance. Datastore was searched for all MDR GNB isolates authorised over the period audited.
Results: 20 patients were included. Most isolates were ESBL producing E.coli, the rest being other Enterobacteriaceae and a single Pseudomonas aeruginosa. ICNs advised isolation of all patients. 11 patients (55%) were isolated. If patients were not isolated cubicles were usually already occupied by patients with infections. Risk factors for spread of infection or vulnerable close contacts were identifi ed for 15 patients, but only documented in 8 cases by ICNs. Standard infection control precautions and adherence to trust policy for MDR GNB was advised in all cases. Nurses reported following all aspects of advice in most cases. The major exception was for a patient where the ward staff were unaware the patient was infected with a MDR GNB. 46 MDR GNB were authorised over the audit period according to a datastore search. 28 (61%) were notifi ed to ICNs. Average time from receipt of specimen to reporting to ICNs was 3.7 days.
Conclusions: Adherence rates to most ICN advice were high. Isolation was not possible in many cases but this was expected given limited isolation facilities. The main area for improvement identifi ed was speed and reliability of reporting of isolates. Given limited resources and lack of consensus at local and national level a debate is needed as to the best way to approach the control of infections for MDR GNB. Is Helicobacter pylori antibiotic resistance surveillance needed and how can it be delivered? A feasibility study in three UK centres. Lasseter G,1 Shaw I,2 Lawson, A,3 D’Arcy S,4 Glocker E,5 and McNulty C1 1Primary Care Unit, HPA, Gloucestershire Hospitals NHS Trust, UK. 2Endoscopy Unit, Gloucestershire Hospitals NHS Trust, UK. 3Helicobacter Reference Unit, Centre for Infections, HPA, Colindale, London, UK. 4Public Health Wales Microbiology Bangor, Ysbyty Gwynedd, Bangor, UK. 5. Division of Infection and Immunity, School of Life and Medical Sciences, University College London, London, UK
Helicobacter pylori eradication requires a proton pump inhibitor plus two antibiotics: amoxicillin, clarithromycin or metronidazole. Treatment failures are increasing and alternatives are Tetracyclines, Quinolones and Rifabutin.
We determined the feasibility of H. pylori antimicrobial resistance surveillance, using gastric antral biopsy specimens from routine endoscopies in the 3 centres still doing culture: Gloucester, Bangor and the Helicobacter Reference Unit (HRU). European standard methods were used for culture and susceptibility by E-tests.
Biopsy specimen culture positivity was low in the primary referral centres: Gloucester 72/1307 (6%), Bangor 60/910 (7%) compared to 109/339 (32%) referred mainly post treatment failure to the HRU. Resistance rates were signifi cantly higher in Bangor and HRU isolates than Gloucester. Metronidazole: HRU 88%, Bangor 43%, Glos 22% (p<0.01); Clarithromycin: HRU 68%, Bangor 18%, Glos 3% (p<0.003); Levofl oxacin: HRU 17%, Bangor 13%, Glos 1% (p<0.01); Rifabutin: HRU 0%, Bangor 0%; Rifampicin: Glos 4%; Amoxicillin: HRU 3%, Bangor 2%, Glos 1%; Tetracycline: HRU 1%, Bangor 2%, Glos 3%.
Patient details and antibiotic history collected retrospectively by paid endoscopy staff was poor. Consequently a dedicated researcher completed all data collection.
Ongoing diagnostic susceptibility testing in treatment failures and surveillance is essential as primary resistance varies signifi cantly between centres and is high post treatment. In treatment failure Metronidazole and Clarithromycin should be avoided, but Amoxicillin, Tetracycline and Rifabutin can be used without culture as resistance is low. Including centres of greater deprivation and thus higher prevalence could decrease the numbers of specimens needed to support H.pylori surveillance. To obtain antibiotic history a researcher is required. Molecular based surveillance could be an alternative to allow centralisation, but is expensive and is only available for Clarithromycin and Levofl oxacin. e-Bug: Evaluation of a hygiene and prudent antibiotic use educational pack in the Czech Republic, France and England. * Lecky DM1, Weinberg J2, Verlander N3, Touboul P4 and Benes J5 and McNulty CAM1 on behalf of the e-Bug working group 1 Primary Care Unit, Health Protection Agency, Gloucester Royal Hospital, England, 2 City University, London, England 3 Health Protection Agency, Colindale, London, 4 Hopital l’Archet 1, Nice, France, 5. Bulovka University Hospital, Prague, Czech Republic
Objectives: To measure the eff ectiveness of the e-Bug pack in improving children’s knowledge in 4 key areas - Introduction to Microbes, Transfer of Infection, Treatment of Infection and the Prevention of Infection, when used within the National Curriculum in England, France and the Czech Republic.
Methods: Teaching, using the e-Bug pack, was given by junior and senior school teachers. 1358 students across 45 junior schools and 1636 students across 46 senior schools took part in the evaluation.
Qualitative data was obtained via, teacher focus groups, qualitative teacher questionnaire on each topic and qualitative student questionnaire on each topic.
Quantitative questionnaires were completed by all students at three diff erent time points to assess students•
Data collected from all three countries was combined and analyses was performed in STATA, version 10, using xtlogit and xtreg commands for the dichotomous and continuous outcomes, respectively, for the fi rst set and xtmelogit and xtmixed, respectively, for the second set.
Results: A signifi cantly higher percentage of students taught using e-Bug increased and retained their knowledge, as opposed to students who were taught using other resource materials, at both Junior and Senior school level.
Qualitative data demonstrated that students in both age groups preferred the more interactive ‘hands on’ activities and group work activities were preferred by the majority of schools.
Conclusions: Although the draft pack can be viewed as a success there is a need to modify various sections of both the junior and senior schools packs to make them more appealing
The data from this evaluation have been used to further improve the packs. The e-Bug packs have been translated into associated partner languages and the full e-Bug resource (packs, game and website) will be offi
Evaluation of a Novel AmpC Detection Method Kit to Detect all Types of AmpC Production. Mather, B., Smith, L. Whiston Hospital, Warrington Road, Prescot, Merseyside
Resistance to extended-spectrum cephalosporins is increasing in prevalence due to the production of AmpC beta-lactamase enzymes by members of the family Enterobacteriaceae. These enzymes are cephalosporinases capable of hydrolysing β-lactam antibiotics, leading to multiple antibiotic resistances, leaving few therapeutic options. They have arisen through acquisition of a plasmid-mediated ampC gene, or hyper-production of a chromosomally encoded AmpC enzyme. Chromosomal AmpC may be present in Enterobacteriaceae and can be induced or expressed due to a mutation that leads to the derepression of the chromosomal ampC gene.
Organisms expressing these enzymes have been associated with false in-vitro susceptibility to cephalosporins posing a problem for clinical microbiologists due to phenotypic tests being misleading, resulting in misreporting. AmpC production can often go undetected, risking therapeutic failure in patients who consequently receive inappropriate antibiotics.
Methods for the detection of AmpC are limited. Screening for cefoxitin resistance can be useful for initial AmpC detection, but the reliability of this is questionable. Therefore there is a requirement for a simple diagnostic test for confi rmation of AmpC production.
The aim of the study was to evaluate a novel AmpC detection disc test, based on a combination disc method which incorporates cefpodoxime as a screening agent, an AmpC inhibitor, an inducer compound, and clavulanic acid as an inhibitor against the activity of ESBLs. A collection of 16 strains producing known AmpC and/or ESBL enzymes, and a panel of 187 cefoxitin-resistant clinical isolates were tested.
Results showed the disc test method was correlative with the known strains. Out of the 187 clinical isolates 79% were positive for AmpC by disc test method, 10% negative, and 11% as indeterminable and likely ESBL-positive. The discs may prove to be a useful tool for the clinical laboratory. A simple, accurate and cost eff ective diagnostic test will lead to improved reporting and appropriate antibiotic therapy for patients. On-line survey of Medicines Managers to determine how antibiotic stewardship is being promoted in Primary Care Trusts McNulty CAM1, Guise T2, Turner K1, Hand K3, Howard P4, Dryden M5, Cooke J6 1Health Protection Agency Primary Care Unit, Gloucester, 2British Society for Antimicrobial Chemotherapy, Birmingham 3Southampton University Hospitals NHS Trust, 4Leeds Teaching Hospitals NHS Trust, 5Winchester & Eastleigh Healthcare NHS Trust, 6School of Pharmacy and Pharmaceutical Sciences, University of Manchester
BSAC, the Health Protection Agency and ARHAI are keen to promote appropriate and prudent use of antimicrobials in community settings.
Methods: In July 2010 PCT medicines managers in England were invited to participate via email and directed by a link to questions on Survey Monkey. Non-responders were phoned in September 2010.
Results: 108 medicines managers responded, but as some covered more than one PCT the results represent 117/147, 79% of PCTs. 54% of PCTs had an antimicrobial committee, 62% had an antimicrobial audit strategy, 29% had an antimicrobial training strategy, and 23% had a substantive primary care antimicrobial prescribing advisor. Nearly all PCTs (95%) reported antimicrobial use back to practices and 64% of practices undertook annual audit. All PCTs had evidence-based antimicrobial community guidance suggesting antimicrobial choice, dose and duration; 73% gave guidance on delayed prescribing. 79% of respondents used a National antimicrobial template to develop their guidance; 92% adapted the HPA guidance and of these 70% found it very useful. However, only 6 respondents reported the HPA guidance was easy to fi nd on the internet. 59% of respondents referred to Clinical Knowledge Summaries and NICE to develop their guidance and of these 36% found the CKS and 28% found NICE very useful. Very few respondents used the infection Specialist Library or the Map of Medicine.
Conclusions: Although all PCTs have community antimicrobial guidance in place and nearly all feed antimicrobial use back to GP practices, there is an opportunity to improve antimicrobial use in primary care as 73% do not have an antimicrobial training strategy and a third have no defi ned audit strategy. The HPA guidance should be supported, as 92% of PCTs use this National template to develop their local guidance, but its accessibility should be improved. Partnership Programme to reduce Health Care Associated Infections (HCAIs) in a Developing Country Oates K, Walker S: Countess of Chester NHS Foundation Trust
Introduction: The World Health Organisation (WHO) African Partnership for Patient Safety (APPS) was launched in 2009. It is a programme based existing relationships and extending them to manage patient safety. The Countess of Chester Hospital is one of 3 English Hospitals partnered with an African hospital in the fi rst wave Of APPS. The Countess of Chester Hospital is paired with COU Kisiizi Hospital, Uganda, a not for profi t non-government hospital in rural location in Uganda.
The APPS project identifi es twelve key action areas for Patient Safety. Each partnership is to initially focus on 4 action areas for the fi rst 2 years with the other areas being tackled further on in the project. All partnerships will focus on reduction of HCAI as a priority. The action areas for the Kisiizi/Chester link are:1.
Minimise risks associated with HCAIs, through many avenues, including hand hygiene and compliance
monitoring, starting local production of alcohol based hand rub (ABHR), monitoring systems for HCAI
reduction, antibiotic use including surgical prophylaxis and setting up an Infection Control Committee (ICC)
Reviewing healthcare waste management systems
Implementing the WHO Safe Surgery Checklist
Aim: To introduce a Partnership Programme to reduce Health Care Associated Infections in a Developing Country.
Results: Baseline results showed an HCAI prevalence of 6% hospital wide. In addition, baseline audit showed overall compliance of 41% with hand hygiene standards, based on the WHO 5 moments for hand hygiene. Spread of the programme was attempted in many ways. The Kisiizi APPS launch was held, this engaged patients, many staff from Kisiizi and senior staff from local hospitals promoting the patient safety message and the programme at Kisiizi. The launch also including a song composed by a local choir and a performance by a traditional dance group to promote the importance of hand hygiene in everyday situations.
Conclusions: The programme will continue and further outcome measures will be recorded, with the aim of driving improvements in patient safety. The long term core objectives of the APPS programme include building and strengthening partnerships between hospitals in Africa & Europe (focussing on patient safety), implementing patient safety improvements in each partnership hospital and facilitating spread of patient safety improvements across all 46 African nations committed to the programme.
An analysis of bacteraemia caused by gram negative Extended Spectrum Beta Lactamase producers (ESBLp) at Darent Valley Hospital Patel R*, Bassi P†, Enayat M**, Cotter L†, Gonzalez-Ruiz A† Departments of Pharmacy*, Critical Care** and Microbiology†, Darent Valley Hospital, Dartford & Gravesham NHS Trust, Kent
Introduction: Inappropriate antibiotic treatment for bacteraemia caused by ESBLp is associated with higher mortality rates (60% vs. 20%)1. Mortality due to severe sepsis is between 28%-50%2.
Our 2 years bacteraemia surveillance shows that the prevalence of ESBLp was 20.2%. A retrospective analysis of local bacteraemia surveillance data from 1/10/2007-30/9/2009 was conducted to investigate the impact of gentamicin resistance, our current empirical aminoglycoside, and the appropriateness of empirical treatment for ESBLp infections on:•
Scientifi c fi ndings: Overall coliform bacteraemia’s (321) mortality and gentamicin resistance rates were 42.4% (136/321) and 16.2 % (52/321) respectively. Infection with a gentamicin resistant micro-organism increased the overall risk of death by 10.7% and within 30 days by 9.6%.
A total of 65 ESBLp cases were found (20.2%). 53.8% (35/65) of these cases were gentamicin resistant. From these, 35 cases 57.1% (20/35) died, 65% (13/20) within 30 days.
Of the 62 patients with ESBL producing gram negative bacteraemia reviewed further, 35 were gentamicin resistant and 27 gentamicin sensitive. In both the resistant and the sensitive groups there were 15 survivors. There were 20 deaths in the resistant group and 12 in the sensitive group. Patients in the resistant group accounted for a total of 1371 bed days (estimated cost £606,400) and patients in the sensitive group accounted for a total of 643 bed days (estimated cost £228,600). This included both ITU and general ward bed day costs.
Discussion: LOS may be reduced due to an early mortality associated with inappropriate and/or delayed therapy; it is also possible that such therapy may actually prolong the LOS, and thus the costs, of a hospitalization before resulting in death.
It seems that appropriate antimicrobial therapy has a positive eff ect on survival, particularly when and aminoglycoside is administered empirically.
We understand that LOS may be infl uenced by other factors such as demographics, co-morbidities, pathogenicity of infecting micro-organism and timing of empirical treatment. We are in the process of analysing these variables.
The fi ndings showed that LOS is almost double in patients with gentamicin resistance and there is a clear signifi cant diff erence in cost of hospitalisation (£377,800) between patients infected with susceptible and resistant micro-organisms.
Conclusion: We have replaced gentamicin with amikacin, for which we did not fi nd any resistant isolates, as empirical treatment for septic patients at an excess cost of approximately £50,000/year. This provides a potential cost benefi t of approximately £138,900/year.
References:1. Tumbarello et al. Predictors of Mortality in Patients with Bloodstream Infections Caused by Extended-Spectrum-β-Lactamase-Producing Enterobacteriaceae: Importance of Inadequate Initial Antimicrobial Treatment, AAC June 20072. Dellinger, Levy and Carlet et al. Surviving Sepsis Campaign, Crit Care Med 2008. Point Prevalence Survey of Antibiotic Use in Trusts in the North West of England Shatwell J, Oates K Stockport NHS FT & Countess of Chester NHS FT, North West Antibiotic Pharmacists’ Group
Introduction: In trusts throughout the North West of England, antibiotic pharmacists complete snapshot, point prevalence audits to obtain information about antibiotic prescribing. Information obtained includes percentage of patients on antibiotics, percentage of antibiotics prescribed with course length documented, rates of compliance with allergy documentation and data on the types of antibiotics used and the indications they were prescribed for.
Compare antibiotic use between diff erent trusts
Compare use of restricted antibiotics between trusts
Assess any correlation between total antibiotic prevalence and the rate of Clostridium diffi
Assess any correlation between class of antibiotics prescribed and rate of CDI
Methods: The data was collected by individual trusts on one day during March 2010. This was then collated and analysed.
Results and Discussion: 19 Trusts submitted data. On average only 48% of antibiotics had course lengths documented and there was 93% compliance with allergy documentation on drug charts.
Mean prevalence of antibiotics was 28% (range 22-39) The results show no obvious correlation between CDI rates and ‘good’ antibiotic prescribing (in terms of overall rates of prescribing and rates of prescribing of antibiotics considered high risk for CDI). This does not necessarily mean that there is no relationship between the two as many factors infl uence CDI, such as infection control, cleaning and GP prescribing. The CDI rates compared were HPA published yearly rates per 10000 bed days, April 09 to March 10. As this audit was completed in March 10, the yearly CDI rates may not be representative of the time the audit was completed.
The limitations of this data are that trusts diff er hugely in terms of size and speciality which can aff ect antibiotic usage and types. The other main limitation is that the audit is only a snap shot and may not be representative of usual antibiotic usage.
Conclusions: Despite the lack of correlation between CDI rates and ‘good’ antibiotic prescribing this data is useful for individual trusts to compare themselves with others locally. It is also interesting to demonstrate the large spread of antibiotic usage and prevalence across just one region. Surveillance of antimicrobial use and resistance in Scotland – monitoring the impact of national antimicrobial stewardship Wiuff , C. Malcolm, W., Wilson, J., Cromwell, T., Bennie, M. and Eastaway, A., on behalf of the Scottish Antimicrobial Prescribing Group (SAPG) National Services Scotland (NSS): Health Protection Scotland (HPS), Glasgow, Scotland and Information Services Division (ISD), Edinburgh, Scotland
As part of national strategy an antimicrobial stewardship programme, coordinated by SAPG, aimed at enhancing the quality of antimicrobial prescribing and clinical outcomes while minimising the harmful eff ects associated with antimicrobials (including resistance development, healthcare associated infections and adverse reactions) was introduced in Scotland in 2008.
The objective of this study is to provide national baseline data on antimicrobial use and resistance obtained in 2008, and to assess the potential early impact of the Scottish antimicrobial stewardship programme in 2009.
Information on the use of antibacterials in primary care was obtained from a database (‘PRISMS’) of all NHSScotland prescriptions dispensed in the community maintained by ISD, which includes all prescriptions dispensed in the community.
The antimicrobial resistance surveillance system for Scotland is modelled on the EARS-net protocol. Antimicrobial susceptibility data on bacteraemias of key organisms were extracted from a database (‘ECOSS’) hosted by HPS which receives data from the laboratories.
Quantitative information on antibacterials used in primary care and antimicrobial resistance in key organisms associated with bacteraemia in 2008 was used to set the baseline for Scotland.
In 2009 the overall use of systemic antibacterials (items/1000/day) was 1.6% lower than in 2008. In particular, reductions in the use of co-amoxiclav (14.7%), fl uoroquinolones (7.1%) and cephalosporins (21.2%) were observed in 2009 relative to 2008.
In 2008, resistance to nearly all clinically important classes of antibiotics was reported for the Gram-negative bacteraemias. In 2009, no major increases in resistance were observed among the Gram-negative organisms (E. coli, K. pneumoniae, P. aeruginosa). Resistance to third generation cephalosporins in E. coli had decreased signifi cantly since 2008. Among the Gram-positive organisms vancomycin resistance in E. faecium increased from 17% to 28% from 2008 to 2009.
This report sets the baseline against which emerging trends in antimicrobial use and resistance can be monitored as the Scottish antimicrobial stewardship programme progresses – and provide an early indication that the stewardship programme is having a positive impact on the quality of prescribing in primary care in Scotland.
Epidemiology of Stenotrophomonas maltophilia bacteraemia in a tertiary hospital (Wythenshawe Hospital experience) A.Y Zhou & I. A. Hassan University Hospital of South Manchester Foundation Trust, Wythenshawe Hospital Manchester.
Background: Stenotrophomonas maltophilia is a nosocomial gram negative bacillus which can cause opportunistic infections. Although infection with this organism is still relatively uncommon, the prevalence has been increasing recently especially in patients with co-morbidities. We present our experience of a 5-year retrospective review of bacteraemia due to Stenotrophomonas maltophilia from the University Hospital of South Manchester between 1st January 2004 and 31st December 2009.
Objective: This review was done to gain further understanding of the epidemiology of Stenotrophomonas maltophilia bacteraemia in the UK, including risk factors and outcome.
Methods: Records of all positive blood cultures with Stenotrophomonas maltophilia between 1/1/2004 – 31/12/2009 were obtained from our Lab information system (Telepath).
A case note review of all the patients with positive blood cultures was done & data extracted on a standard proforma including demographic details, clinical features & outcome of the cases.
University Hospital of South Manchester is a 900-bed tertiary hospital that provides services including heart and lung transplants, regional burns, adult cystic fi brosis and 2 intensive care units.
Results: A total of 47 patients were found to have positive blood cultures. 24 (51%) of these patients were males. The results of 40 patients with complete data will be presented & the 7 patients who had incomplete data will not be discussed further.
The most common contributing risk factors included the presence of venous/arterial lines (21%), surgery (16%), prolonged hospital stay (15%), immunosupression and respiratory support (both 11.5%). 12 patients (30%) had cardiovascular pathologies and 6 patients (15%) had pre-existing malignancies.
The source of bacteraemia was most likely due to venous lines (31%) and respiratory tract infections (28%). Nearly 1/3 of patients had multiple sources of infections. The majority of patients (97.5%) had no past history of Stenotrophomonas maltophilia infection. 27 patients (67.5%) fully recovered from the episode of Stenotrophomonas maltophilia bacteraemia. 13 patients died, out of which only 2 deaths were thought to be directly related to the bacteraemia.
Conclusion: Recent data suggests that the prevalence of infection with Stenotrophomonas maltophilia is rising. Our review also suggests that although Stenotrophomonas maltophilia bacteraemia generally occurs in debilitated patients, the outcome is good if managed appropriately. Measures such as prompt venous line removal can prevent the persistence of the bacteraemia as well as relapses. A large prospective study will be required in the UK to determine the epidemiology & impact of infection with this organism. Organising Secretariat Esme Hewings British Society for Antimicrobial Chemotherapy Griffi
53 Regent PlaceBirminghamB1 3NJT: 0121 236 1988F: 0121 212 [email protected]
U nited S tates B ankruptcy C ourt Chambers of Christopher S. Sontchi(302) 252-2888Natalie D. Ramsey1105 Market Street, 15th FloorCounsel for The Official CommitteeOf Unsecured Creditors Leslie Controls, Inc., Case No. 10-12199 Before the Court is a discovery dispute between (i) Century Indemnity Companyand Fireman’s Fund Insurance Company (collectively, the “Insurers”); and (ii
Under the mentorship of our Youth Pastor, Marcel deRegt, 212° Ministries have continued to flourish. The GEMS organization celebrated their 50th anniversary this past year! The IGNITE Youth Group adopted part of Yale Road (from Broadway to Prest) for garbage clean-up. After 16 years of involvement and leadership, Linette Vugteveen relinquished her role. Thank you f
 Biological profi ling of new vancomycin derivatives with potent activity against superbugs
Biological profi ling of new vancomycin derivatives with potent activity against superbugs