Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Chroniccure.ie
0363-5465/103/3131-0268$02.00/0THE AMERICAN JOURNAL OF SPORTS MEDICINE, Vol. 31, No. 2 2003 American Orthopaedic Society for Sports Medicine
Shock Wave Application for Chronic Plantar Fasciitis in Running Athletes A Prospective, Randomized, Placebo-Controlled Trial
Jan D. Rompe,* MD, Jens Decking, MD, Carsten Schoellner, MD, and Bernhard Nafe, MD
From the Department of Orthopaedics, Johannes Gutenberg University School of Medicine,Background: Recent articles have reported success with repeated low-energy shock wave application for treatment of chronic plantar fasciitis in runners. Hypothesis: Shock wave treatment for chronic plantar fasciitis is safe and effective. Study Design: Prospective, randomized, placebo-controlled trial. Methods: Forty-five running athletes with intractable plantar heel pain for more than 12 months were enrolled; half were assigned to a treatment group that received three applications of 2100 impulses of low-energy shock waves, and half received sham treatment. Follow-up examinations were performed at 6 months and at 1 year by a blinded observer. Results: After 6 months, self-assessment of pain on first walking in the morning was significantly reduced from an average of 6.9 to 2.1 points on a visual analog scale in the treatment group and from an average of 7.0 to 4.7 points in the sham group. The mean difference between groups was 2.6 points. After 12 months, there was a further reduction of pain in both groups, to an average 1.5 points in the treatment group, and to 4.4 points in the sham group. Conclusion: Three treatments with 2100 impulses of low-energy shock waves were a safe and effective method for treatment of chronic plantar fasciitis in long-distance runners. 2003 American Orthopaedic Society for Sports Medicine
Chronic plantar fasciitis due to cumulative overload stress
protocol is regarded as the mainstay of recommended treat-
is one of the most common painful foot conditions observed
ment.32 The use of shoes with shock-absorbing soles or shoes
in runners, both competitive athletes and those who run
fitted with a standard orthopaedic device such as a rubber
for basic conditioning.12,22,45 The specific pathologic fea-
heel pad or taping of the foot into a specific position is also
tures of this clinical entity are not well understood; inflam-
recommended. The recommendation of heel elevation to
mation of the plantar fascia, thickening of the proximal
achieve reduction of loading of the plantar fascia is contro-
fascia, decreased vascularity, peritendinous inflammation,
versial.19 Steroid injections into the painful area also have
loss of normal elasticity, and alteration of nociceptor physi-
been used27 but are associated with a significant risk of
ology all may play roles in the onset and persistence of heel
subsequent rupture of the plantar fascia.23
pain.22,30 The pain is usually present when the patient first
Usually, plantar fasciitis can be treated successfully by
stands on his or her feet after awakening, and it persists or
tailoring treatment to a patient’s risk factors and prefer-
becomes worse with activities of daily living. The use of
ences. When nonoperative treatment options are unsuc-
nonoperative methods such as rest, application of ice to the
cessful, physicians often resort to open or endoscopic re-
sore area, nonsteroidal antiinflammatory medication, or top-ical application of steroids will alleviate the condition in most
lease of a portion of the plantar fascial insertion onto the
patients,14,33,37,39,42 and the performance of a stretching
calcaneus. If there is suspicion of entrapment of the cal-caneal branches of the tibial nerve, the nerves can bedecompressed. As with any surgery, fascial release is notwithout substantial risk and may be associated with pro-
* Address correspondence and reprint requests to Jan D. Rompe, MD,
longed healing time and postoperative rehabilitation; an
Department of Orthopaedics, Johannes Gutenberg University School of Med-
alteration of foot biomechanical integrity may also
icine, Langenbeckstrasse 1, D-55131 Mainz, Germany.
One author has received financial benefit from research in this study. Shock Wave Application for Plantar Fasciitis
Because of the recognized risks and delayed healing
week before symptoms occurred. Over a period of more
associated with surgery, alternative nonoperative thera-
than 6 months, at least three attempts of nonoperative
peutic methods have been assessed. Since 1996, there
treatment had failed to provide pain relief for all patients:
have been reports of promising results from the use of
this included at least two prior courses of intervention
extracorporeal shock wave application for plantar fasci-
with physical therapy, the use of orthotic devices, and at
itis, particularly in Europe.7,9,20,26,30,31,34 Randomized,
least one prior course of pharmacologic treatment.
controlled studies on shock wave application and prospec-
Exclusion Criteria. Exclusion criteria included dysfunc-
tive observational trials on shock wave application have
tion in the knee or ankle, local arthritis, generalized poly-
reported comparable treatment effects in 50% to 60% of
arthritis, rheumatoid arthritis, ankylosing spondylitis,
patients.2,10 The scientific value of some of the studies
Reiter’s syndrome, neurologic abnormalities, nerve en-
that examined the use of shock wave application for treat-
trapment syndrome, a history of previous plantar fascial
ment of plantar fasciitis was seriously questioned recent-
surgery, age of less than 18 years, pregnancy, infections or
ly.6 Therefore, the current clinical study was planned as a
tumors, a history of spontaneous or steroid-induced rup-
prospective, randomized, single-blinded evaluation of the
ture of the plantar fascia, bilateral heel pain, participation
potential for low-energy electromagnetic application of ex-
in a workers’ compensation program, or use of systemic
tracorporeal shock waves to bring about pain relief for
therapeutic anticoagulants or nonsteroidal antiinflamma-
chronic plantar fasciitis in runners. Our hypothesis was
tory drugs for any chronic condition. No other treatment
that three applications of 2100 impulses were superior to
was permitted until 6 weeks after shock wave application,
three placebo applications at 6 months after treatment.
with the exception of use of already-worn shoe insertsduring the period of treatment. Patients were instructedto use the foot but to avoid painful stress.
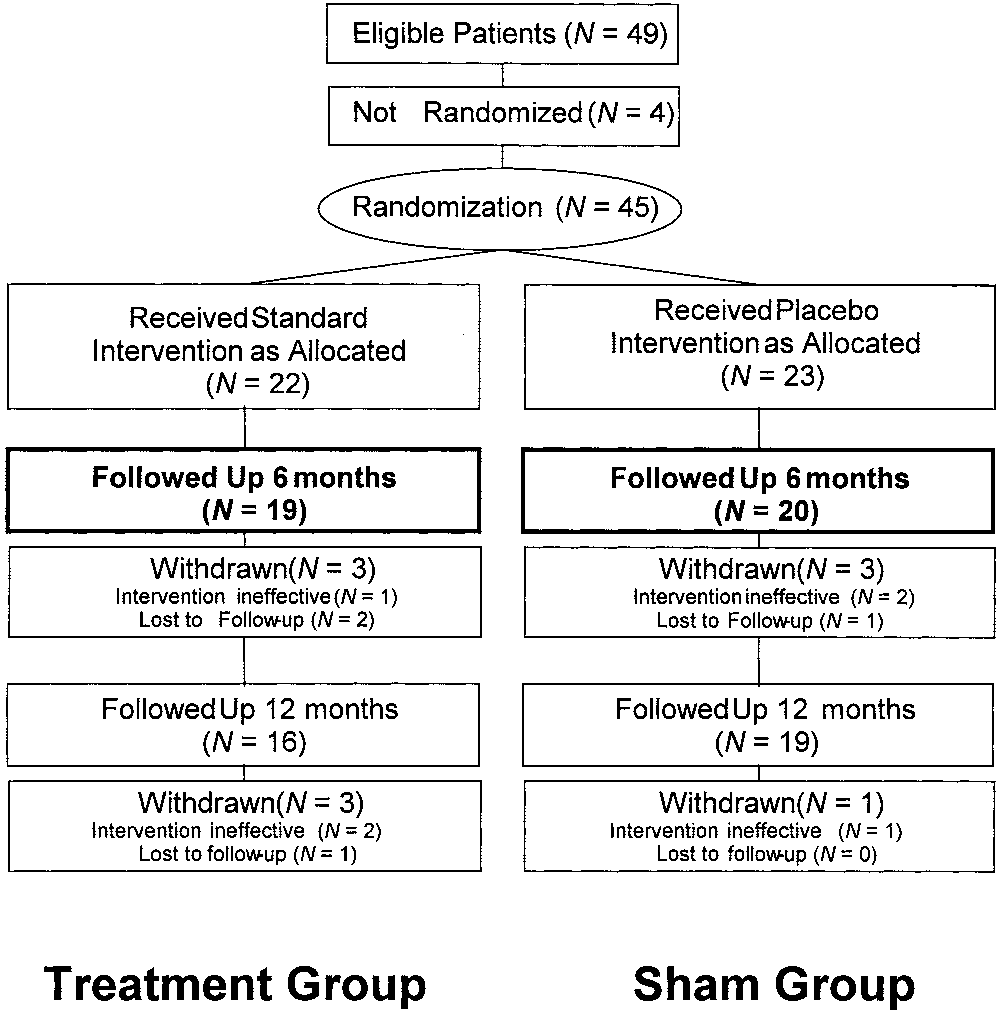
Forty-nine patients qualified for the study, of whom 4
The study was designed as a randomized, single-center,
declined to be randomized, leaving 45 patients enrolled in
single-blinded parallel treatment study with an indepen-
the study (Fig. 1). Extracorporeal shock wave treatment
dent observer to determine the effectiveness of three ap-
was free of cost to all participants. No crossover between
plications of 2100 impulses of low-energy shock waves to
the two groups was offered. In case of failure of treatment,
the heels of long-distance runners with intractable plan-
the patients were invited to undergo surgery of the heel.
tar fasciitis. A sham treatment group was used for
All patients had been treated unsuccessfully by their gen-
eral practitioner, and 38 patients had also been treated byan orthopaedic practitioner. All patients had been givenmedication, mostly nonsteroidal antiinflammatory drugs,
and had received shock-absorbing shoe inserts. All had
On the basis of the results of a pilot study,36 a difference
performed some kind of stretching exercises on a regular
of 3 points on the average pain rating on a visual analog
basis; only 18 patients had used night splints. Eleven
scale ranging from 0 to 10 points was assumed to be asignificant difference between the groups, with a commonstandard deviation of 3 points. A sample size of 17 pa-tients per treatment group would have more than 80% ofthe power to detect the treatment difference with a two-sided significance level of 0.05. Accordingly, a sample sizeof 22 patients per treatment group, including an assumed20% rate of patients lost to follow-up, was calculated togive sufficient statistical power. The sample size was alsosufficient for the evaluation of the treatment differencesin terms of the Ankle-Hindfoot Scale,18 and in terms of thesubjective four-step rating scale.
Over a period of 3 years, recreational athletes who ranmore than 30 miles per week and were suffering fromchronic plantar fasciitis for more than 12 months werescreened and randomized to one of two treatment groups:active treatment or sham treatment. Inclusion Criteria. For the current study, chronic heel
pain was defined as symptoms of moderate-to-severe heelpain in the involved foot at the origin of the proximalplantar fascia on the medial calcaneal tuberosity. Thepain must have persisted for at least 12 months before thestudy enrollment, in patients who ran at least 30 miles per
Figure 1. Profile of the randomized controlled trial. American Journal of Sports Medicine
patients had been immobilized in a cast for at least 2
another. Each study subject assigned to active treatment
weeks, and an average of 2.8 corticosteroid injections had
underwent shock wave application for a total of 6300
been given (range, 1 to 5). An average of three different
shocks in three treatment sessions, with a 1-week interval
physical therapy treatment regimens had been used, such
in between, at an energy flux density of 0.16 mJ/mm2 and
as icing, ultrasound, magnetic field, iontophoresis or pho-
at a frequency of 4 Hz, without local anesthesia. Ultra-
nophoresis, contrast baths, or radiation therapy (range,
sound coupling gel was used between the treatment head
one to five different treatment regimens).
and the heel. The shock tube head was applied underin-line ultrasound control (Fig. 2); fine adjustment to the
most tender region was performed by palpation and inter-action with the patient. Treatment was started at the
After 4 weeks of no treatment at all and after giving
lowest energy level, 1, for 50 impulses and was then in-
informed consent, the patients were reevaluated regard-
creased to energy level 2 for another 50 impulses. Then
ing exclusion criteria and were then randomized into the
2000 impulses of energy level 3 (energy flux density of 0.16
two treatment groups by use of identical sealed envelopes.
Patients in the two groups did not differ regarding weekly
For those patients assigned to sham treatment, a sound-
running distance, age, sex, duration of pain, weight, or
reflecting pad was interposed between the coupling mem-
body mass index. The first shock wave application started
brane of the treatment head and the heel to absorb the
immediately after the identification of treatment group.
shock waves through the presence of multiple air cavities. Shock Wave Treatment Group. The treatment group
No coupling gel was used. A total of 6300 shocks was
consisted of 10 women and 12 men, with a mean age of 43
delivered in three treatment sessions, with a 1-week in-
years (range, 32 to 59) and a mean duration of pain of 20
terval in between, effectively duplicating the duration and
Sham Treatment Group. The group receiving sham
treatment consisted of 13 women and 10 men, with amean age of 40 years (range, 30 to 61) and a mean dura-
tion of pain of 18 months (range, 12 to 72).
All patients were assessed before and after treatment. Theactual study procedure was conducted by a physician who
was aware of the treatment. However, this physicianplayed no role in assessing the patients after treatment.
The extracorporeal shock wave therapy was applied by a
Another physician, an independent treatment-blinded ob-
mobile therapy unit especially designed for orthopaedic
server, examined the patients at 6 and at 12 months after
use (Sonocur Plus, Siemens AG, Erlangen, Germany),
the last application of the extracorporeal shock wave
with the shock wave head suspended by an articulating
arm for flexible movement of the head in three planes. Theshock wave head was equipped with an electromagneticshock wave emitter. Shock wave focus guidance was es-
tablished by in-line integration of an ultrasound probe (a7.5-MHz sector scanner) in the shock head. The physical
The primary outcome measure was prospectively defined
output parameters of the device, measured with a laser
as reduction of the subject’s self-assessment of pain on
first walking in the morning. On the visual analog scale,
Both groups were treated under the same conditions,
10 points indicated unbearable pain and 0 points, no pain
and patients were treated singly to avoid influencing one
at all. The 6-month interval was selected because it was
Output Parameters of the Shock Wave Device
Shock Wave Application for Plantar Fasciitis
to walk free from pain for more than 1 hour. Three pointswas considered acceptable, with symptoms somewhat im-proved, pain at a more tolerable level than before treat-ment, and the patient slightly satisfied with the treatmentoutcome. Four points indicated a poor outcome, withsymptoms identical or worse and the patient dissatisfiedwith the treatment outcome.
The methods used for statistical analysis in this studywere determined by the local Institute for Medical Statis-tics and Documentation before the study was begun andwere performed by them when the study was completed. Wilcoxon’s rank sum test was applied for comparison ofthe difference between the two groups for pseudocontinu-ous, not normally distributed variables, such as pain whenfirst walking in the morning and scores on the Ankle-Hindfoot Scale.24 The four-step scale, a categorical vari-able, was compared by means of Fisher’s exact test and itsextension to 2 ϫ N contingency tables. The level of signif-icance was set at 95%. Tested comparisons with P valuesof less than 0.05 were considered to be significantly dif-ferent. Multiple adjustments were not performed for sec-ondary outcome measures, which were measured in anexploratory way. The primary outcome measure wastested in a confirmatory way.28
Twenty-two and 23 patients were randomized consecu-
Figure 2. Ultrasound-guided adaptation of the shock wave
tively to each group. Two patients in the treatment group
head to the medioplantar aspect of the left heel.
and one patient in the sham group were lost to follow-up. Thus, after 6 months, 19 patients in the treatment groupand 20 in the sham group were evaluated (Fig. 1). One
expected that the healing process would likely be evident
patient in the treatment group and two patients in the
(although not necessarily complete) at this point in time.
sham group refused further contact because of lack ofsuccess of the therapy.
At 12 months, the intervention had been ineffective for
two patients, who refused to cooperate further, and one
Prospectively defined secondary outcome measures for
patient could not be contacted. Thus, 16 patients in the
clinical evaluation 6 and 12 months after treatment in-
treatment group were available for examination. Nineteen
cluded at least a 50% reduction of a subject’s self-assess-
patients in the sham group were evaluated at 12 months,
ment of pain on first walking in the morning, a visual
and one additional patient refused to cooperate further
analog scale rating of less than 4 of 10 points, and im-
because shock wave therapy had not improved his
provement from the baseline in the American Orthopaedic
Foot and Ankle Society’s Ankle-Hindfoot Scale.18 Thisstrictly clinical score has 100 possible points (pain, 40
points; function, 50 points; alignment, 10 points). In addi-tion, patients had to show improvement from baseline on
The primary outcome measure was prospectively defined
a subjective four-point rating scale and achievement of a
as reduction of pain on first walking in the morning after
rating less than or equal to two points at 6 months and at
6 months of a subject’s self-assessment. Results are pre-
12 months after shock wave application. On the scale, 1
sented in Table 2. The mean difference between groups
point was defined as excellent, with the patient having no
was 2.6 points (P ϭ 0.0004; 95% confidence interval, 1.3 to
pain, satisfied with the treatment outcome, and able to
perform unlimited walking free from pain. Two points was
After 6 months, 12 of 20 patients (60%) in the treatment
defined as good, with symptoms significantly improved
group and 6 of 22 patients (27%) in the sham group re-
and the patient satisfied with treatment outcome and able
ported more than a 50% improvement in pain on first
American Journal of Sports Medicine
during the various and unsuccessful treatment regimens
Mean Reduction in Self-Assessment of Pain on First Walking in
before the current study. No patient discontinued the
shock wave procedure because of severe pain. No side
effects were seen at either follow-up examination. Therewere no hematomas, infections, or abnormal neurologic
walking in the morning, with values of less than 4 points
Numbers of concurrent interventions did not differ signif-
on the visual analog scale (P ϭ 0.0600). These results
icantly between groups at follow-up. At 6 months, 3 of 19
included those of one patient in the treatment group and
patients (16%) in the treatment group and 6 of 20 patients
two patients in the sham group who reported via tele-
(30%) in the sham group received further nonoperative
phone an ineffectiveness of the intervention and refused
therapy. At 12 months, 3 of 16 patients (19%) in the
further clinical evaluation; they were rated as treatment
treatment group and 5 of 19 patients (26%) in the sham
failures. After 12 months, 13 of 18 patients (72%) in the
group received further nonoperative therapy. One patient
treatment group and 7 of 20 patients (35%) in the sham
in each group had undergone surgery (6% and 5%,
group reported more than a 50% improvement in pain on
first walking in the morning (P ϭ 0.0051). These resultsalso included those of two patients in the treatment groupand one patient in the sham group who reported by tele-
phone an ineffectiveness of the intervention and refused
The clinical diagnosis of plantar fasciitis is relatively easy
further clinical evaluation; they were also rated as treat-
to make.21 Radiographically, a heel spur on the inferior
surface of the calcaneus frequently is evident but is not
After 6 months, an increase in the Ankle-Hindfoot Scale
considered pathognomonic of the disorder.37 Magnetic res-
was observed in both groups, by 37.2 Ϯ 15.2 points in the
onance imaging regularly shows edematous involvement
treatment group and by 19.4 Ϯ 17.8 points in the sham
of the calcaneal insertion of the plantar aponeurosis, with
group (P ϭ 0.0025). The three patients who refused to
a marked thickening of the proximal segment of the cen-
participate further in the study because of ineffectiveness
tral cord of the plantar fascia.4,13,29,40 Although proximal
of treatment were not included in the computation of the
plantar fasciitis is the most frequent cause of inferomedial
score. Results are given in Table 3.
heel pain, other pathologic conditions, such as seronega-
Before the extracorporeal shock wave therapy started,
tive arthropathies or nerve entrapment, may be causal in
all patients rated their condition as “4” in the subjective
about 10% of cases. Two patient cohorts seem to have a
four-step scale. There was no difference between the
particularly high incidence of plantar fasciitis: obese mid-
groups at this point in time. After 6 months, an improve-
dle-aged women and young male runners.26,30,37
ment was seen in both groups on the four-step scale, by
Most authors agree that subjects with insertional plan-
1.9 Ϯ 0.9 points in the treatment group and by 1.0 Ϯ 1.0
tar fasciitis have a self-limiting disease and that most will
point in the sham group (P ϭ 0.0112). Results are given in
attain good results without significant intervention.
Therefore, the initial treatment should be nonoperative,with use of modalities such as physical therapy, especially
fascial stretching, orthoses, night splints, shoe wear mod-ifications, and nonsteroidal antiinflammatory drugs.30
Low-energy extracorporeal shock wave therapy was con-
However, Martin et al.27 reviewed numerous studies of
sidered unpleasant by all patients, although not as un-
nonsurgical treatment for plantar fasciitis and showed a
pleasant as the local infiltration all patients had had
wide variation of acceptable outcomes, ranging from 44%to 82% of patients obtaining complete relief of heel pain.
In their metaanalysis, Crawford et al.12 looked for ran-
Mean Scores on the American Orthopaedic Foot and Ankle
domized controlled trials on plantar fasciitis and found 11
studies on nonoperative treatment since 1966. However,
these trials had low methodologic assessment scores; not a
single one evaluated the effectiveness of surgical therapy.
The metaanalysis showed there was limited evidence for
the short-term effectiveness of topical corticosteroid ad-ministered by iontophoresis and for the effectiveness of
use of dorsiflexion night splints. A preliminary study from
our institution also showed limited evidence of the effective-
ness of low-energy extracorporeal shock wave therapy.34
This preliminary positive outcome has been confirmed in
prospective clinical studies from various university hospi-
tals.20,31,38 The scientific value of these studies was seri-
Shock Wave Application for Plantar Fasciitis
ously questioned recently,6 and the therapeutic mechanism
months, pressure pain had dropped for patients in group 1
involved remains a topic of speculation.15,25 Ogden et al.30
from 77 points to 19 points on a visual analog scale. In
postulated that shock waves are directed at controlled mi-
group 2, the ratings did not decrease significantly, from 79
crodisruption of internal fascial tissue, which initiates a
points to 77 points. In group 1, walking became completely
more appropriate healing response within the fascia and a
free from pain for 25 of 50 patients, compared with none of
better long-term capacity to adapt to biologic and biome-
48 patients in group 2. By 5 years, when the rates of good
chanical demands. No evidence was presented.
or excellent outcomes in the four-step score were com-
There is no consensus so far concerning the (repeated)
pared, the difference of only 11% in favor of group 1 was no
use of low-energy shock waves, requiring no local anesthe-
longer significant; pressure pain was down to 9 points in
sia,34,36 versus the (single) use of high-energy shock
group 1 and to 29 points in group 2. Meanwhile, 5 of 38
waves, requiring local or regional anesthesia.7,30 Indeed,
patients (13%) in group 1 had undergone surgery of the
there is no consensus so far as to how to differentiate
heel, compared with 23 of 40 patients (58%) in group 2.
low-energy from high-energy shock waves, because multi-
Buchbinder et al.8 included 166 patients in a double-
ple physical parameters are involved (see Table 1). Al-
blind, randomized, placebo-controlled trial. Patients were
though the clinical effect of both protocols appears to be
randomly assigned to receive either ultrasound-guided
comparable, as discussed later, there is clear evidence of
extracorporeal shock wave treatment given weekly for 3
increasing side effects with the application of increasing
weeks to a total dose of at least 1 J/mm2 or an identical
energy levels.35 With the treatment regimen described in
placebo to a total dose of 0.006 J/mm2. After significant
this article, deleterious side effects are extremely unlikely
improvements in both groups (26.3 points in the treat-
as compared with treatment regimens involving applica-
ment group, 25.7 points in the sham group), there was no
tion of higher-energy flux densities. No local anesthesia
evidence for superiority of extracorporeal shock wave
was required, so related side effects are lacking. The only
treatment over placebo. The study by Buchbinder et al. is
“disadvantage” is that, according to our experience, a re-
of excellent quality, but there are some points to be dis-
cussed. First, patients in the treatment group did not
Maier et al.26 recently reported good or excellent results
receive identical treatment (either 2000 or 2500 shock
on a subjective four-step score in 75% of 48 heels 29
waves per treatment of energy levels varying between
months after low-energy shock waves were applied three
0.02 mJ/mm2 and 0.33 mJ/mm2), in contrast with the
times at weekly intervals without local anesthesia. The
current study. Second, the mean dose in the treatment
clinical outcome was not influenced by the length of fol-
group was 1407 mJ/mm2, 500 mJ/mm2 more than in the
low-up. No negative side effects were reported. Wang et
current study. In the experience of the authors of the
al.43 reported 33 of 41 patients to be either free of pain or
current study, patients will not tolerate such a high dose
significantly better at 12 weeks after shock wave therapy.
unless the treatment area of maximal pain is missed.
Ogden et al.30 published results of a randomized placebo-
Accordingly, and third, Buchbinder et al. did not focus on
controlled study with 119 patients in the treatment group
the area of maximal pain as in the current study, but on
and 116 patients in the placebo group. Twelve weeks after
the area of maximal thickness of the plantar fascia.
a single application of 1500 high-energy shock waves at
Fourth, a potent analgesic drug was allowed for the dura-
18 kV under regional anesthesia, success was observed in
tion of the study. Fifth, patients were enrolled with a pain
47% of patients (56). After sham treatment, the success
history as short as 6 weeks, in contrast with the 12
rate was only 30% (35 patients). The results of this study
months in the current study. Sixth, there was no real
led to approval of shock wave therapy for painful heel by
placebo group; sham therapy consisted of application of
the United States Food and Drug Administration in 2000.
Buch et al.7 reported the results of another randomized
In the current study, better results were observed 6
placebo-controlled study for the Food and Drug Adminis-
months after low-energy shock wave application of 2100
tration involving 150 patients. Therapy was applied once,
impulses compared with sham treatment, with a signifi-
with 3800 high-energy impulses under regional anesthe-
cant reduction of the subjects’ self-assessment of pain on
sia. After 3 months, 61% of the patients (45 patients) in
first walking in the morning by an average of 5 points in
the treatment group and only 40% (29 patients) of the
the treatment group (from 7 to 2 points) and by 2 points
placebo group met the success criterion. Chen et al.9 stud-
(from 7 to 5 points) in the sham group. Sixty percent of
ied 80 patients treated with 1000 shock wave impulses at
patients in the treatment group, versus 27% of the pa-
14 kV. Fifty-four patients were evaluated at 6 months.
tients in the sham group, reported at least a 50% reduc-
There were no complaints from 32 patients (59.3%), and
tion and a visual analog scale rating of less than 4 of 10
15 patients (27.7%) were significantly improved.
points. After 12 months, 72% of the patients of the treat-
More recently, we reported a randomized controlled
ment group, versus 35% of the patients of the sham group,
trial of shock wave therapy in 112 patients.36 Group 1
rated accordingly. Cointerventions remained on a compa-
received 3 applications of 1000 impulses of a low-energy
flux density, and group 2 received 3 applications of 10
Because of the well-described natural history of proxi-
impulses within 2 weeks. When the rates of good and
mal plantar fasciitis,30 it was expected that symptoms of
excellent outcome on a four-step score were compared
chronic heel pain could resolve with time, even in this
between the two groups, there was a significant difference
selected treatment patient population in whom several
of 47% in favor of group 1 treatment at 6 months. At 6
previous nonoperative treatments had failed. Therefore,
American Journal of Sports Medicine
the improvement in both groups between 6 months and 1
9. Chen HS, Chen LM, Huang TW: Treatment of painful heel syndrome with
shock waves. Clin Orthop 387: 41– 46, 2001
year after treatment probably reflects the self-limiting
10. Concato J, Shah N, Horwitz RI: Randomized, controlled trials, observa-
course of the disease. However, more patients in the treat-
tional studies, and the hierarchy of research designs. N Engl J Med 342:
ment group improved during this period of follow-up than
11. Conti RJ, Shinder M: Soft tissue calcifications induced by local corticoste-
in the sham group. No side effects have been reported so
roid injection. J Foot Surg 30: 34 –37, 1991
far from low-energy extracorporeal shock wave applica-
12. Crawford F, Atkins D, Edward J: Interventions for treating plantar heel pain
tion, compared with calcification after steroid injections or
(Cochrane Review), in Cochrane Library, Issue 3. Oxford, Update Soft-ware, 2000
postoperative development of wound infections, hypertro-
13. Grasel RP, Schweitzer ME, Kovalovich AM, et al: MR imaging of plantar
phic sensitive scars, or calcaneal fractures.5,11,37 In the
fasciitis: Edema, tears, and occult marrow abnormalities correlated with
current study, no negative side effects were recorded. This
outcome. AJR Am J Roentgenol 173: 699 –701, 1999
14. Gudeman SD, Eisele SA, Heidt RS Jr, et al: Treatment of plantar fasciitis
clinical experience is in accordance with those of histologic
by iontophoresis of 0.4% dexamethasone. A randomized, double-blind,
and MRI-based studies.26,35 High-energy shock waves,
placebo-controlled study. Am J Sports Med 25: 312–316, 1997
also in use for the treatment of heel pain,30,31,38 on the
15. Heller KD, Niethard FU: Using extracorporeal shockwave therapy in or-
thopedics: A meta-analysis [in German]. Z Orthop Ihre Grenzgeb 136:
other hand, may produce side effects such as periosteal
detachments and small fractures of the inner surface of
16. Henricson AS, Westlin NE: Chronic calcaneal pain in athletes: Entrapment
of the calcaneal nerve? Am J Sports Med 12: 152–154, 1984
17. Ikeda K, Tomita K, Takayama K: Application of extracorporeal shock wave
on bone: Preliminary report. J Trauma 47: 946 –950, 1999
18. Kitaoka HB, Alexander IJ, Adelaar RS, et al: Clinical rating systems for the
ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int 15: 349 –
19. Kogler GF, Veer FB, Verhulst SJ, et al: The effect of heel elevation on
The results of the current study revealed beneficial effects
strain within the plantar aponeurosis: In vitro study. Foot Ankle Int 22:433– 439, 2001
of low-energy extracorporeal shock wave therapy in long-
20. Krischek O, Rompe JD, Herbsthofer B, et al: Symptomatic low-energy
distance runners with chronic plantar fasciitis. In accor-
shockwave therapy in heel pain and radiologically detected plantar heel
dance with the results of other prospective randomized
spur. Z Orthop Ihre Grenzgeb 136: 169 –174, 1998
21. Lapidus PW, Guidotti FP: Painful heel: Report of 323 patients with 364
controlled trials,7,30,36 shock wave therapy appeared to be
painful heels. Clin Orthop 39: 178 –186, 1965
a useful, noninvasive treatment method with negligible
22. Leach RE, DiIorio E, Harney RA: Pathologic hindfoot conditions in the
side effects. The level of evidence for success with this
athlete. Clin Orthop 177: 116 –121, 1983
23. Leach RE, Jones R, Silva T: Rupture of the plantar fascia in athletes.
treatment concept is still limited,6,12 but this is true also
J Bone Joint Surg 60A: 537–539, 1978
for other nonoperative procedures and especially true for
24. Lehmann EL: Nonparametrics: Statistical Methods Based on Ranks. San
surgical treatment, which bears a higher risk of compli-
25. Loew M, Daecke W, Kusnierczak D, et al: Shock-wave therapy is effective
cations. Therefore, we recommend shock wave therapy to
for chronic calcifying tendinitis of the shoulder. J Bone Joint Surg 81B:
any patient who has had unsuccessful conventional non-
26. Maier M, Steinborn M, Schmitz C, et al: Extracorporeal shock wave
operative treatment over a period of at least 6 months,
application for chronic plantar fasciitis associated with heel spurs: Predic-
before considering an operative intervention. Further pro-
tion of outcome by magnetic resonance imaging. J Rheumatol 27: 2455–
spective work is necessary to compare the effectiveness of
27. Martin RL, Irrgang JJ, Conti SF: Outcome study of subjects with inser-
repeated low-energy shock wave application without local
tional plantar fasciitis. Foot Ankle Int 19: 803– 811, 1998
anesthesia with the efficacy of single high-energy shock
28. Maurer W, Hothorn LA, Lehmacher W: Multiple comparison in drug
wave application with local or regional anesthesia.
clinical trials and preclinic assays: A priori ordered hypotheses, inVollmer J (ed): Biometrie in der pharmazeutischen Industrie. Volume 6. Testing Principles in Clinical and Preclinical Trials. Stuttgart, Fischer,1995, pp 3–18
29. Narvaez JA, Narvaez J, Ortega R, et al: Painful heel: MR imaging findings. REFERENCES
30. Ogden JA, Alvarez R, Levitt R, et al: Shock wave therapy for chronic
1. Barrett SL, Day SV: Endoscopic plantar fasciotomy for chronic plantar
proximal plantar fasciitis. Clin Orthop 387: 47–59, 2001
fasciitis/heel spur syndrome: Surgical technique— early clinical results. J
31. Perlick L, Boxberg W, Giebel G: High-energy shock wave treatment of the
painful heel spur [in German]. Unfallchirurg 101: 914 –918, 1998
2. Benson K, Hartz AJ: A comparison of observational studies and random-
32. Pfeffer G, Bacchetti P, Deland J, et al: Comparison of custom and pre-
ized, controlled trials. N Engl J Med 342: 1878 –1886, 2000
fabricated orthoses in the initial treatment of proximal plantar fasciitis. Foot
3. Benton-Weil W, Borelli AH, Weil LS Jr, et al: Percutaneous plantar fas-
ciotomy: A minimally invasive procedure for recalcitrant plantar fasciitis. J
33. Probe RA, Baca M, Adams R, et al: Night splint treatment for plantar
Foot Ankle Surg 37: 269 –272, 1998
fasciitis. A prospective randomized study. Clin Orthop 368: 190 –195,
4. Berkowitz JF, Kier R, Rudicel S: Plantar fasciitis: MR imaging. Radiology
34. Rompe JD, Hopf C, Nafe B, et al: Low-energy extracorporeal shock wave
5. Blanco CE, Leon HO, Guthrie TB: Endoscopic treatment of calcaneal spur
therapy for painful heel. A prospective controlled single-blind study. Arch
syndrome: A comprehensive technique. Arthroscopy 17: 517–522, 2001
Orthop Trauma Surg 115: 75–79, 1996
6. Bo¨ddeker R, Scha¨fer H, Haake M: Extracorporeal shockwave therapy
35. Rompe JD, Kirkpatrick CJ, Kullmer K, et al: Dose-related effects of shock
(ESWT) in the treatment of plantar fasciitis—A biometrical review. Clin
waves on rabbit tendo Achillis. A sonographic and histological study. J Bone Joint Surg 80B: 546 –552, 1998
7. Buch M, Knorr U, Fleming L, et al: Extracorporeal shockwave therapy in
36. Rompe JD, Schoellner C, Nafe B: Evaluation of low-energy extracorporeal
plantar fasciitis—-3 months results of a multicentre prospective random-
shock-wave application and treatment of chronic plantar fasciitis. J Bone
ised double blind placebo controlled trial. Orthopa¨de 31: 637– 644, 2002
8. Buchbinder R, Ptasznik R, Gordon J, et al: Ultrasound-guided extracor-
37. Schepsis AA, Leach RE, Gorzyca J: Plantar fasciitis. Etiology, treatment,
poral shock wave therapy for plantar fasciitis: A randomized controlled
surgical results, and review of the literature. Clin Orthop 266: 185–196,
trial. JAMA 288: 1364 –1372, 2002
Shock Wave Application for Plantar Fasciitis
38. Sistermann R, Katthagen BD: Five-year lithotripsy of plantar heel spur:
42. Tomczak RL, Haverstock BD: A retrospective comparison of endoscopic
Experiences and results. A follow-up study after 36.9 months [in German].
plantar fasciotomy to open plantar fasciotomy with heel spur resection for chronic
Z Orthop Ihre Grenzgeb 136: 402– 406, 1998
plantar fasciitis/heel spur syndrome. J Foot Ankle Surg 34: 305–311, 1995
39. Sobel E, Levitz SJ, Caselli MA: Orthoses in the treatment of rearfoot
43. Wang CJ, Chen HS, Chen SW, et al: Treatment of painful heels using
problems. J Am Podiatr Med Assoc 89: 220 –233, 1999
extracorporeal shock wave. J Formos Med Assoc 99: 580 –583, 2000
40. Steinborn M, Heuck A, Maier M, et al: MRI of plantar fasciitis [in
44. Wapner KL, Sharkey PF: The use of night splints for treatment of recal-
German]. RoFo Fortschr Geb Rontgenstr Neuen Bildgeb Verfahr 170:
citrant plantar fasciitis. Foot Ankle 12: 135–137, 1991
45. Ward WG, Clippinger FW: Proximal medial longitudinal arch incision for
41. Theodorou DJ, Theodorou SJ, Kakitsubata Y, et al: Plantar fasciitis and
plantar fascia release. Foot Ankle 8: 152–155, 1987
fascial rupture: MR imaging findings in 26 patients supplemented with
46. Young CC, Rutherford DS, Niedfeldt MW: Treatment of plantar fasciitis.
anatomic data in cadavers. Radiographics 20: S181–S197, 2000
Am Fam Physician 63: 467– 478, 2001
Abuse of Dominance: The Third Wave of Brazil’s Antitrust Enforcement? Ana Paula Martinez* T he first Brazilian competition law dates from 1962, but it was only in the mid-1990s when the modern era of antitrust began as the country shifted to a market-based economy. Among other reforms, in 1994 Congress enacted Law No 8,884, which governed Brazil’s administrative antitrust law
Skin Disease/Sign Medications 2000, Derm Facts Adverse Drug Reaction Probability Scale Question 1. Are there previous conclusive reports of this reaction? 2. Did the adverse event appear after the suspected drug was administered? 3. Did the adverse reaction improve when the drug was discontinued or a specific antagonist was administered? 4. Did the adverse reaction reappear w
 Shock Wave Application for Plantar Fasciitis
Because of the recognized risks and delayed healing
week before symptoms occurred. Over a period of more
associated with surgery, alternative nonoperative thera-
than 6 months, at least three attempts of nonoperative
peutic methods have been assessed. Since 1996, there
treatment had failed to provide pain relief for all patients:
have been reports of promising results from the use of
this included at least two prior courses of intervention
extracorporeal shock wave application for plantar fasci-
with physical therapy, the use of orthotic devices, and at
itis, particularly in Europe.7,9,20,26,30,31,34 Randomized,
least one prior course of pharmacologic treatment.
Shock Wave Application for Plantar Fasciitis
Because of the recognized risks and delayed healing
week before symptoms occurred. Over a period of more
associated with surgery, alternative nonoperative thera-
than 6 months, at least three attempts of nonoperative
peutic methods have been assessed. Since 1996, there
treatment had failed to provide pain relief for all patients:
have been reports of promising results from the use of
this included at least two prior courses of intervention
extracorporeal shock wave application for plantar fasci-
with physical therapy, the use of orthotic devices, and at
itis, particularly in Europe.7,9,20,26,30,31,34 Randomized,
least one prior course of pharmacologic treatment. Shock Wave Application for Plantar Fasciitis
to walk free from pain for more than 1 hour. Three pointswas considered acceptable, with symptoms somewhat im-proved, pain at a more tolerable level than before treat-ment, and the patient slightly satisfied with the treatmentoutcome. Four points indicated a poor outcome, withsymptoms identical or worse and the patient dissatisfiedwith the treatment outcome.
Shock Wave Application for Plantar Fasciitis
to walk free from pain for more than 1 hour. Three pointswas considered acceptable, with symptoms somewhat im-proved, pain at a more tolerable level than before treat-ment, and the patient slightly satisfied with the treatmentoutcome. Four points indicated a poor outcome, withsymptoms identical or worse and the patient dissatisfiedwith the treatment outcome.