Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Elisedusseldorp.nl
British Journal of Cancer (2004) 90, 1176 – 1183
All rights reserved 0007 – 0920/04 $25.00
Survival of patients with nonseminomatous germ cell cancer: areview of the IGCC classification by Cox regression and recursivepartitioning
MR van Dijk*,1, EW Steyerberg1, SP Stenning2, E Dusseldorp3 and JDF Habbema1
Department of Public Health, Erasmus MC – University Medical Center Rotterdam, PO Box 1738, 3000 DR Rotterdam, The Netherlands; 2Medical
Research Council, Clinical Trials Unit, 222 Euston Road, London, NW1 2DA, UK; 3Data Theory Group, Department of Education, Leiden University, PO
Box 9555, 2300 RB Leiden, The Netherlands
The International Germ Cell Consensus (IGCC) classification identifies good, intermediate and poor prognosis groups among patients
with metastatic nonseminomatous germ cell tumours (NSGCT). It uses the risk factors primary site, presence of nonpulmonary
visceral metastases and tumour markers alpha-fetoprotein (AFP), human chorionic gonadotrophin (HCG) and lactic dehydrogenase
(LDH). The IGCC classification is easy to use and remember, but lacks flexibility. We aimed to examine the extent of any loss in
discrimination within the IGCC classification in comparison with alternative modelling by formal weighing of the risk factors. We
analysed survival of 3048 NSGCT patients with Cox regression and recursive partitioning for alternative classifications. Good,
intermediate and poor prognosis groups were based on predicted 5-year survival. Classifications were further refined by subgrouping
within the poor prognosis group. Performance was measured primarily by a bootstrap corrected c-statistic to indicate discriminative
ability for future patients. The weights of the risk factors in the alternative classifications differed slightly from the implicit weights in the
IGCC classification. Discriminative ability, however, did not increase clearly (IGCC classification, c ¼ 0.732; Cox classification,
c ¼ 0.730; Recursive partitioning classification, c ¼ 0.709). Three subgroups could be identified within the poor prognosis groups,
resulting in classifications with five prognostic groups and slightly better discriminative ability (c ¼ 0.740). In conclusion, the IGCC
classification in three prognostic groups is largely supported by Cox regression and recursive partitioning. Cox regression was the
most promising tool to define a more refined classification.
British Journal of Cancer (2004) 90, 1176 – 1183. doi:10.1038/sj.bjc.6601665
Keywords: Cox regression; recursive partitioning; germ cell cancer; prognostic classifications
Testicular germ cell tumours (seminomatous and nonseminoma-
combining the main prognostic factors for progression-free
tous) are the most common cancers among young adult men. Since
survival (PFS) and overall survival (Bajorin et al, 1988, 1991;
the 1970s, long-term cure rates of patients with germ cell tumours
Mead et al, 1992). The coexistence of classifications differing in
have increased to over 80%, because of the ability of cisplatin-
type, complexity and ability to separate good from poor prognosis
based chemotherapy to cure advanced disease (Bosl and Motzer,
complicated international collaboration in randomised trials and
1997; Hartmann et al, 1999; Steele et al, 1999; Sonneveld et al,
made comparison of nonrandomised studies impossible. Interna-
2001). Owing to the high overall cure rate, interest has shifted from
tional collaboration by the International Germ Cell Cancer
increasing the overall cure rate to reducing treatment-related
Collaborative Group resulted in the development of the Interna-
toxicity for patients with a good prognosis (de Wit et al, 2001). On
tional Germ Cell Consensus Classification (IGCC classification),
the other hand, high-risk patients, eligible for more intensive
which is widely applied and easy to use and remember (IGCCCG,
treatment, for example, stem-cell support or high-dose chemother-
apy, should be identified (Bokemeyer et al, 1999, 2002).
For the IGCC classification, readily available risk factors were
Several classifications have been proposed in the past to
selected from a wider set following Cox regression analyses,
distinguish patients according to prognosis, by identifying and
namely primary site, presence of nonpulmonary visceral metas-tases (NPVM) and elevation of the tumour markers alpha-fetoprotein (AFP), human chorionic gonadotrophin (HCG) and
*Correspondence: MR van Dijk; E-mail: [email protected]
lactic dehydrogenase (LDH). All variables were categorical, since
Presented in part at Third Joint meeting of the International Society for
no major differences in performance were found compared to
Clinical Biostatistics and the Society for Clinical Trials, London, UK, 20 –
using continuous variables (McCaffrey et al, 1998). In Table 1, how
the risk factors were combined into three prognostic groups for
Received 6 November 2003; revised 17 December 2003; accepted 17
patients with nonseminomatous germ cell tumours (NSGCT) with
December 2003; published online 24 February 2004
either good, intermediate or poor prognosis are shown. The good
A review of the development of the IGCC classificationMR van Dijk et al
International Germ Cell Consensus Classification for nonsemi-
Centres participating in the International Germ Cell Collaborative
Group provided retrospective data of 5202 adult male patients with
NSGCT. All patients were treated between 1975 and 1990 with
cisplatin-based chemotherapy. Data were collected on age, primary
AFP good ¼ 0 and HCG good ¼ 0 and LDH good ¼ 0
site, date of diagnosis, levels of serum AFP, HCG and LDH, nodal
disease in the abdomen, mediastinum, and neck, lung metastases,spread to other visceral sites like liver, bone and brain and on
treatment details like previous therapy. For the development of the
IGCC classification, patients without missing data on the risk
factors primary site, NPVM, tumour markers AFP, HCG and LDH
and the outcome survival were selected (n ¼ 3048) (IGCCCG,
AFP intermediate ¼ 1 or HCG intermediate ¼ 1 or LDH intermediate ¼ 1
The outcome measures were PFS and overall survival from the
start of the chemotherapy. The risk factors in the IGCC
classification were primary site (testis/retroperitoneal vs medias-
AFP poor ¼ 2 or HCG poor ¼ 2 or LDH poor ¼ 2
tinum), presence of NPVM (yes/no) and tumour markers AFP,
HCG and LDH. Each tumour marker had three categories; good,
Tumour markers AFP/HCG/LDH: Good – AFP o1000 ng mlÀ1, HCG o5000 iu lÀ1,
intermediate and poor with specific cutoff points on the
LDH o1.5 Â upper limit of normal; Intermediate – AFP 1000 – 10000 ng mlÀ1, HCG
continuous tumour markers (see Table 1) (IGCCCG, 1997). The
5000 – 50000 ng mlÀ1, LDH 1.5 – 10 Â N; Poor – AFP 410000 ng mlÀ1, HCG
same risk factors and categories were used to construct the
alternative classifications based on Cox regression and recursivepartitioning.
prognosis group is characterised by the absence of adverse riskfactors. The intermediate prognosis group is defined by the
The IGCC classification makes no clear distinction between the
presence of any intermediate tumour marker, that is, one or more
intermediate tumour markers and between the poor risk factors
intermediate tumour markers are present. The poor prognosis
and is represented by a max score. One way to assess this
group is characterised by the presence of any of the poor risk
assumption is by evaluating whether the weights in the IGCC
factors mediastinal primary site, NPVM, AFP poor, HCG poor or
classification were optimally allocated to the risk factors. We
LDH poor, that is, one or more poor risk factors are present. The
hereto varied the IGCC weights (1/2) over the levels of the risk
classification can be seen as a max function where the good,
factors and compared all possible combinations with respect to
intermediate and poor prognosis groups have a maximum score of
performance. Performance was quantified by the difference in
minus twice the log likelihood (model w2) (Clayton and Hills,
In the IGCC classification, all intermediate tumour markers and
all poor risk factors were required only to be sufficiently bad to be
We used the Cox regression to study the univariable and
classified as intermediate and poor prognosis, respectively, that is,
multivariable effects of the IGCC risk factors on the overall
differences in importance between intermediate tumour markers
survival, expressed as Hazard ratios and regression coefficients.
and differences in importance between poor risk factors are not
The Cox regression model formed the basis of classification ‘5R’.
taken into account. Furthermore, no distinction is made between
We multiplied the multivariate regression coefficients by 10 and
the number of intermediate tumour markers in the intermediate
rounded them to obtain weights. A sum score was calculated by
prognosis group and the number of poor risk factors in the poor
multiplying the weights with individual patient characteristics and
prognosis group. Better discrimination might be achieved by
adding the resulting individual scores (Assmann et al, 2002). We
incorporating differences in predictive strength and testing
calculated the estimated 5-year survival rate for each score.
The IGCC classification can be viewed as implying that the risk
Furthermore, it is difficult to adjust the current classification for
factors are strongly dependent, that is, that there are interactions
changes in treatment strategy. A more flexible scoring system
between risk factors. There is, for example, no distinction made
could more easily identify subgroups for the identification of very
between patients with one poor risk factor or three poor risk
high risk patients eligible for novel chemotherapy approaches such
factors. To test whether and which interactions were present, we
as high-dose chemotherapy or the use of novel cytotoxic agents
added all two-way interactions between the IGCC risk factors in a
(Bokemeyer et al, 1999; Kollmannsberger et al, 2000). We however
Cox regression model. Important interactions were selected
note that an important consideration in developing the IGCC
through stepwise backward selection (Po0.05). Since interactions
classification was that all the prognostic groups should be large
based on small number of patients give unreliable regression
enough to make randomised trials of new treatments for each
coefficients, the interaction terms were defined as linear. The
prognostic group feasible (IGCCCG, 1997).
resulting model forms the basis of classification ‘5Ri’. A sum score
The aim of this study was to reconsider steps taken in the
based on a regression model with interactions is, however, more
development of the IGCC classification, and to investigate
difficult to calculate and interpret. Therefore, a table was
alternative classifications based on Cox regression and recursive
constructed with 5-year survival estimates for all possible
partitioning (Breiman et al, 1984) that may discriminate better and
combinations of the IGCC risk factors based on the Cox regression
be more suitable to identify more subgroups.
model with linear interactions. The number of patients on which
British Journal of Cancer (2004) 90(6), 1176 – 1183
A review of the development of the IGCC classification
each survival estimate was based is given to indicate the reliability
validated by taking random bootstrap samples (100) (Efron and
Tibshirani, 1993; Harrell et al, 1996).
An alternative and visually more attractive way of exploring and
presenting interactions between risk factors is by growing a treethrough recursive partitioning (Breiman et al, 1984; Segal and
Bloch, 1989; Ahn and Loh, 1994) that we used to constructclassification ‘5T’. A binary tree is built by the following process:
The median follow-up time of surviving patients was 50 months.
first the risk factor that best splits the data into two groups, leading
Disease progression occurred in 680 patients, and 533 patients
to the largest decrease in prediction error, is determined (recursive
died. The 5-year PFS was 78% (95% CI 76 – 79%) and the 5-year
partitioning or splitting method). Splitting continues until the
overall survival 82% (95% CI 81 – 84%). Most patients had as
subgroups reach a minimum size or until no improvement can be
primary site testis or retroperitoneum (97%), no NPVM (92%),
made (stopping rule). The full tree, which is often too complex and
and good AFP, HCG and LDH levels (84, 87 and 67%, respectively)
overfit, is pruned using crossvalidation. All trees within one
(Table 2). All risk factors were predictors of survival as indicated
standard error of the lowest crossvalidated prediction error are
by the Hazard ratios ranging from 2.1 to 6.2, where the tumour
considered as equivalent. From these equivalent trees, the simplest
marker AFP was the weakest risk factor in the univariable analysis.
is chosen as final tree (Breiman et al, 1984).
As a splitting method, the exponential scaling method was used
(Therneau et al, 1990; LeBlanc and Crowley, 1992). The splittingprocess stopped when a minimum of five patients per groups was
The regression-based weights of the risk factors in classification
reached or when there was no further decrease in prediction error.
5R, and the cutoff points on the resulting sum score are presented
We used 10-fold crossvalidation to determine the optimal tree size.
in Table 3, with the weights and cutoff points of the IGCC
Modelling was performed with S-plus version 2000 using the
RPART library that contains a recursive partitioning method for
The weights suggest that differences between risk factors were
present. Tumour marker AFP had a much lower weight in the
The RPART library (rpart2.zip) and manual (rpart2doc.zip) can
multivariate analysis than tumour markers HCG and LDH. As a
be found at http://www.stats.ox.ac.uk/pub/SWin.
result, a poor AFP level (score 3) is not sufficient to be classified aspoor prognosis in classification 5R. Also, the combination of twoor three intermediate tumour markers, which would lead to an
intermediate prognosis in the IGCC classification, results in a scoreof over 10 and thus in classification in the poor prognosis group in
In all classifications, three prognostic groups were identified using
classification 5R. The presence of risk factor NPVM (score 7) alone
the estimated 5-year survival by sum score (classification 5R),
was not sufficient to be classified as poor prognosis, in contrast
combination of risk factors (5Ri) or binary tree (5T). Subgroups
with the IGCC classification. Patients would only be classified as
with a 5-year survival higher than 90% were considered as good
poor prognosis when other risk factors besides NPVM or AFP are
prognosis, between 65 and 89% as intermediate prognosis, and
We identified four significant interactions in the Cox regression
Furthermore for each classification, we explored the possibility
model; between AFP and primary site (Po0.001), AFP and NPVM
of identifying more subgroups. For the IGCC classification, this
(Po0.01), HCG and NPVM (Po0.003) and HCG and LDH
was carried out by allowing weights to vary from zero to four(instead of zero to two), and comparing all possible combinationson performance. For classifications 5R, 5Ri and 5T, we changed the
Characteristics of 3048 NSGCT patients on the IGCC risk
cutoff points on estimated 5-year survival. A 5-year survival rate
higher than 90% was considered as good prognosis, 75 – 89% asintermediate prognosis, 60 – 74% as good-poor prognosis, 40 – 59%
as intermediate-poor prognosis, and lower than 40% as poor-poorprognosis (Kollmannsberger et al, 2000). Survival of the five
groups of the IGCC classification and classifications 5R, 5Ri and 5T
was presented by Kaplan – Meier curves.
The classifications were evaluated by their ability to distinguishbetween patients differing in survival. An indication of the
discriminative ability is the difference in 5-year survival rates
between the good, intermediate and poor prognosis groups. A c-
statistic was also calculated for both the three and five group
classifications. For binary outcomes, the c-statistic is similar to the
area under the ROC curve (Harrell et al, 1984). The c-statistic for
survival data indicates the probability that for a randomly chosen
pair of patients, the one having the higher predicted survival is the
one who survives longer (Harrell et al, 1984). Overall performanceof the three and five group classifications was measured by model
w2. When a model is developed and evaluated on the same data, the
performance of the model is usually too optimistic. The optimism
can be quantified with statistical methods, known as internal
validation techniques (Steyerberg et al, 2001). To estimate and
correct for the optimism in discriminative ability, the steps takenin the Cox regression and recursive partitioning were internally
NPVM ¼ nonpulmonary visceral metastases.
British Journal of Cancer (2004) 90(6), 1176 – 1183
A review of the development of the IGCC classificationMR van Dijk et al
Weights, coding of variables, and cutoff on the max function of
the IGCC classification and the sum score of the regression-based
The final tree fitted by recursive partitioning, using the
exponential scaling method. The 5-year survival rates, events and total
number of observations per subgroup are given. The resulting subgroups
are displayed in rectangulars and determine classification 5T.
Classifications 5Ri did show a statistically significant increase in
overall performance over the IGCC classification (model w2 422,
2 d.f.). Classification 5T had a worse overall performance with a
NPVM ¼ nonpulmonary visceral metastases.
(Po0.01). The regression coefficients all had negative signs,
indicating that the effect of the risk factors together was smaller
Within the max score, different weights did not lead to an
than the sum of their separate effects. For all 108 combinations of
improvement in overall performance over the weights of the IGCC
the IGCC risk factors, we present 5-year survival estimates from
classification (model w2 402, 2 d.f.). The following weights were
the Cox regression model with interactions (Appendix). Patients
allocated to derive a max function with five prognostic groups in
with testis as primary site and good or intermediate tumour
the IGCC classification with the score varying between 0 and 4;
markers had the highest estimated survival (55 – 92%). Patients
primary site mediastinum (4), NPVM (3), AFP good/intermediate/
with mediastinum as primary site and NPVM had the worst
poor (0/1/2), HCG good/intermediate/poor (0/2/3) and LDH good/
estimated survival (0 – 64%). Since the number of patients with
intermediate/poor (0/1/3). The 5-year survival varied from 37 to
more than one poor risk factor was limited, the survival estimates
92% for the five groups of the IGCC classification, from 34 to 92%
for these patients were less reliable. Recursive partitioning resulted
for classification 5R, from 36 to 92% for classification 5Ri and from
in a tree with seven subgroups with 5-year survival ranging from
35 to 91% for classification 5T (Table 5). The cutoff points on the
35 to 91% (Figure 1), forming the basis of classification 5T.
sum score for the five groups of classification 5R are also given in
Tumour marker LDH was the principal determinant of 5-year
Table 5. The difference in survival between the prognostic groups
survival, making a split between good LDH (N ¼ 2036) and
for each classification is illustrated in Figure 2. The c-statistic for
intermediate/poor LDH (N ¼ 1012). The majority of the ‘good
the five groups of the IGCC classification and classifications 5R
LDH’ subgroup consists of patients with no risk factors (N ¼ 1865)
and 5Ri was slightly higher than for the three group classifications
with an observed 5-year survival of 91% (95% CI 90 – 93%).
(0.739, 0.741 and 0.744, respectively) and with a small amount of
Furthermore, a subgroup of 29 patients with primary site
optimism (0.002) for the Cox regression models. The increase of
mediastinum had a 5-year survival of 55% (95% CI 34 – 72%)
the c-statistic for the five groups of classification 5T was very
and patients with intermediate or poor HCG (N ¼ 142) had a 5-
limited (0.722) with an optimism of 0.011. The increase in model w2
year survival of 70% (95% CI 61 – 77%). Within the subgroup
was more substantial; 422 for the extended IGCC classification, 446
intermediate/poor LDH, four further subgroups were identified
for classification 5R, 450 for classification 5Ri. The increase in
with the risk factors NPVM, primary site and HCG, with 5-year
model w2 for classification 5T (383) was less substantial.
The 5-year survival rates for the good, intermediate and poor
The discriminative ability of classifications derived through Cox
prognosis groups were comparable for the IGCC classification and
regression and recursive partitioning was in concordance with the
classifications 5R, 5Ri and 5T (Table 4). The c-statistic of the IGCC
IGCC classification and therefore supports the validity of the IGCC
classification was 0.732. The apparent c-statistics of classifications
classification. We did, however, find that not all intermediate
5R, 5Ri and 5T were 0.732, 0.735 and 0.718, respectively. Validation
tumour markers and poor risk factors were equally important, and
showed minor optimism in the c-statistic in the Cox regression
that taking these differences into account does affect the
models (0.002). More optimism was present in the classification
classification of patients. In Cox regression-based classifications,
5T, with the c-statistic decreasing from 0.718 to 0.709. Classifica-
especially risk factors NPVM and AFP had less impact compared
tion 5R did not show an improvement in model w2 compared to the
to the other risk factors. That AFP is of less importance than the
IGCC classification (model w2 402 and 401, respectively, 2 d.f.).
other risk factors is confirmed by recursive partitioning where AFP
British Journal of Cancer (2004) 90(6), 1176 – 1183
A review of the development of the IGCC classification
Survival of the IGCC classification, the regression-based classifications 5R and 5Ri and classification 5T based on recursive partitioning
Survival of subgroups within the IGCC classification, the regression-based classifications 5R and 5Ri and classification 5T based on recursive
Surv ¼ 5-year survival. Cutoff points on sum score classification 5R: Good 0, Intermediate 2 – 9, Good – poor 10 – 16, Intermediate – poor 17 – 22, Poor – poor 422.
Survival curves for the five groups of the IGCC classification (A) and classifications 5R (B), 5Ri, (C) and 5T (D).
was not selected in the final tree. Furthermore, not all risk factors
allow for more flexible classifications with more subgroups,
had statistical interactions. In classifications 5Ri and 5T, only a
leading to a small improvement in discriminative ability and 5-
limited number of interactions were included. Combining several
year survival of 34% for the poorest risk patients.
risk factors led to differences in 5-year survival, that is, patients
It appears that the maximum discriminative ability might have
with one poor risk factor had a better chance of survival than
been reached with the current IGCC risk factors and coding,
patients with three risk factors. These deviations from the weights
making further improvement in discriminative ability difficult.
used by the IGCC classification did, however, not lead to
The risk factors selected for the IGCC classification are in
improvements in discriminative ability, in contrast with what we
agreement with risk factors used in other studies on identifying
expected. The use of Cox regression and recursive partitioning did
good and poor prognosis patients with NSGCT (Bajorin et al, 1991;
British Journal of Cancer (2004) 90(6), 1176 – 1183
A review of the development of the IGCC classificationMR van Dijk et al
Mead et al, 1992). Some other potentially useful risk factors
The IGCC dataset suffers from a number of limitations. First,
include age, lung metastases and abdominal mass size. However,
not all data were used for the multivariable regression
adding these three risk factors to the Cox model had no substantial
models because of missing data. When patients with missing
effect on discriminative ability (c increased from 0.73 to 0.74). One
data differ from the other patients on prognosis, this causes a bias
could also consider using continuous codings of tumour markers,
in the regression coefficients and the estimated 5-year survival
but this would lead to an undesirable increase in complexity and
rates (Little, 1992; van Buuren et al, 1999; Clark and Altman,
2003). Secondly, we could not internally validate the IGCC
The division into more prognostic groups is similar to another
classification, because the exact steps taken in the modelling
division by recursive partitioning of poor prognosis patients
process (selection and categorisation of risk factors) were not
(Kollmannsberger et al, 2000). Kollmannsberger et al identified
defined. The IGCC classification was applied to a 30% validation
three prognosis groups: a good-poor, intermediate-poor and poor-
set (IGCCCG, 1997), and although the proportion of patients in
poor risk group with 2-year survival rates of 84, 64 and 49%,
each prognostic group was similar, the 5-year survival for
respectively. These survival rates are higher than the survival rates
poor prognosis patients was higher (57%). We did internally
of the good-poor, intermediate-poor and poor-poor risk groups
validate the modelling steps of the Cox regression models and
identified in the IGCC dataset. This may be due to the difference in
found minor optimism in discriminative ability. Classification 5T,
survival for the poor prognosis patients (72 vs 50%), and remains
based on recursive partitioning, however, showed optimism in
when the difference in follow-up time is taken into account (2 vs 5
discriminative ability, as might be expected from a more data-
years). The data in Kollmannsberger et al (2000) are more recent
driven method. This, in combination with the poorer performance,
and improvements in treatment may have led to the difference in
suggests that recursive partitioning is less suitable for the
construction of prognostic classifications. It can be useful,
The lack of improvement in discriminative ability in both the
however, for exploratory analyses in finding interactions between
classifications with three and five groups might also be explained
by the dominance of the good prognosis group, which has a similar
The survival estimates of the IGCC classification were also
survival for all classifications and contains more than half of all
externally validated with more recent data from an MRC/EORTC
patients. We therefore examined whether discriminative ability
trial (N ¼ 300). The 2-year PFS outcome largely corresponded with
increased within the poor prognosis group of each classification.
the IGCC estimates (IGCCCG, 1997). To gain further insight in the
Discriminative ability increased from 0.50 to 0.60, 0.63, 0.64 and
generalisability of the Cox regression models as well as the IGCC
0.65 for the three poor prognosis groups of classifications 5T,
classification, further external validation is necessary, in larger
IGCC, 5R and 5Ri, respectively. Hence, some improvement was
recent datasets with longer follow-up.
noted within the IGCC poor prognosis group. Furthermore, even
In conclusion, the IGCC classification appears to be a valid way
though the c-statistic is often used and easy to interpret, it is not
to classify patients with NSGCT in three prognostic groups.
suitable for detecting small differences in discriminative ability
Recursive partitioning is less suitable for the construction of
(Harrell et al, 1996; Steyerberg et al, 2000).
prognostic classifications, because of its poorer performance.
Although the use of Cox regression and recursive partitioning
Although Cox regression did not lead to a clear improvement in
did not have a major effect on discriminative ability, they can still
performance, it gave a more flexible and transparent scoring
be useful tools in the construction of future prognostic classifica-
system without much loss in simplicity. We therefore recommend
tions when other criteria are taken into account. One of the
the use of regression-based weights in the development of future
advantages of classifications such as the IGCC classification is its
simplicity. Classification 5T is reasonably simple with only a fewsubgroups and the survival probability readily available. Classifi-cation 5R is slightly more complicated because of the sum scorethat has to be calculated. Finally, classification 5Ri is not so much
complicated as visually unattractive. Furthermore, survival esti-mates for infrequent combinations of risk factors are not reliable
This work was supported by the Netherlands Organisation for
and therefore provide little information on the prognosis of
Scientific Research and by the Royal Netherlands Academy of Arts
and Sciences. We thank the members of the IGCCCG (Medical
A disadvantage of the IGCC classification is its inflexibility.
Research Council (MRC): GM Mead (Royal South Hants Hospital,
More groups could be defined, but not in a straightforward
Southampton, Hampshire, UK), P Cook (MRC Clinical Trials Unit,
manner. Classification 5R and classification 5Ri are very
London), SD Fossa (Norwegian Radium Hospital, Montebello,
flexible with many possible cutoff points. Classification 5T is
Oslo, Norway), A Horwich, SB Kaye (Royal Marsden Hospital,
less flexible due to the limited number of subgroups, but
Surrey, England), RTD Oliver (St Bartholomew’s Hospital, London,
flexibility could be increased by putting fewer restrictions on the
England). European Organisation for the Research and Treatment
recursive partitioning allowing for more subgroups to be
of Cancer (EORTC): PHM de Mulder (Academic Hospital
Nijmegen, The Netherlands), R de Wit and G Stoter (Rotterdam
The IGCC classification considered not just discrimination but
Cancer Institute, The Netherlands), RJ Sylvester (EORTC Data
also simplicity and the size of the resulting prognostic groups and
Center, Brussels Belgium). USA: DF Bajorin, GJ Bosl, M Mazumdar
was chosen by consensus from a shortlist of possible models,
(Memorial Sloan-Kettering Cancer Center, New York). CR Nichols
which balanced these considerations. Consequently, in the IGCC
(Indiana University Hospital, Indianapolis). R Amato (University
classification there is a lack of transparency; it is unclear how the
of Texas MD Anderson Cancer Center, Houston, Texas). Italy: G
classification was constructed statistically because statistical
Pizzocaro (Istituto Nazionale per lo studio e la Cura dei Tumori,
considerations were not the only criteria used to derive the
Milan). France: JP Droz (Centre Leon Benard, Lyon), A Kramar
classification. Classification 5T shows very clearly how the
(CRLC Val d’Aurelle, Montpellier). Denmark: G Daugaard
subgroups were derived from the successive splits in the risk
(Rigshospitalet, Copenhagen). Spain: H Cortes-Funes and L Paz-
factors. Classification 5R shows the difference in importance
Ares (Hospital Doce de Octubre, Madrid). Australia: JA Levi
between the risk factors and how the risk factors are combined in a
(Royal North Shore Hospital, Sydney). New Zealand: BM Colls
sum score. Classification 5Ri could be presented in a similar way as
(Christchurch Hospital, Christchurch), VJ Harvey (Auckland
classification 5R, but interpretation of the main and interaction
Hospital, Auckland). Canada: C Coppin (Fraser Valley Cancer
Centre, Vancouver, British Columbia) and their colleagues (see
British Journal of Cancer (2004) 90(6), 1176 – 1183
A review of the development of the IGCC classification
below) for kindly providing their data for the analyses in this
Netherlands). USA: R Motzer (Memorial Sloan-Kettering Cancer
Center, New York), L Finn (University of Texas MD Anderson
MRC: N Aass (Norwegian Radium Hospital, Oslo, Montebello,
Cancer Center). Italy: R Salvioni and L Mariani (Istituto Nazionale
Norway), PI Clark (Clatterbridge Hospital, Liverpool, England),
Tumori, Milan). Spain: P Lianes Barragan (Hospital doce de
MH Cullen (Queen Elizabeth Hospital, Birmingham, England), D
Octubre, Madrid). Denmark: S Werner Hansen (Rigshospitalet,
Dearnaley (Royal Marsden Hospital, Surrey, England), SJ Harland
(Middlesex Hospital, London, England), WG Jones (Yorkshire
Montpellier), J Bouzy (Institut Gustave Roussy, Villejuif).
Centre for Cancer Treatment, Leeds, England (retired)), ES
Australia: D Thompson (Princess Alexandra Hospital, Brisbane),
Newlands (Charing Cross Hospital, London, England), JT Roberts
T Sandeman (Peter MacCallum Institute, Melbourne), PG Gill
(Northern Centre for Cancer Treatment, Newcastle, England), GJS
Rustin (Mt Vernon Hospital, Middlesex, England), P Wilkinson
Prince Alfred Hospital, Sydney), M Byrne, (Sir Charles Gairnder
and G Read (Christie Hospital, Manchester, England), MV
Hospital, Perth). New Zealand: JD Perez (Dunedin Hospital,
Williams (Addenbrookes Hospital, Cambridge, England). EORTC:
Dunedin), P Thompson & M Bennet, (Auckland Hospital,
D Sleijfer (Academic Hospital Groningen, The Netherlands), D
Auckland). Canada: N Murray (Vancouver Cancer Centre,
WW ten Bokkel Huinink, Netherlands Cancer Institute, The
Ahn H, Loh WY (1994) Tree-structured proportional hazards regression
Hartmann JT, Kanz L, Bokemeyer C (1999) Diagnosis and treatment of
patients with testicular germ cell cancer. Drugs 58: 257 – 281
Assmann G, Cullen P, Schulte H (2002) Simple scoring scheme for
IGCCCG (1997) International Germ Cell Consensus Classification: a
calculating the risk of acute coronary events based on the 10-year follow-
prognostic factor-based staging system for metastatic germ cell cancers.
up of the prospective cardiovascular Munster (PROCAM) study.
International Germ Cell Cancer Collaborative Group. J Clin Oncol 15:
Bajorin D, Katz A, Chan E, Geller N, Vogelzang N, Bosl GJ (1988)
Kollmannsberger C, Nichols C, Meisner C, Mayer F, Kanz L, Bokemeyer C
Comparison of criteria for assigning germ cell tumor patients to ‘good
(2000) Identification of prognostic subgroups among patients with
risk’ and ‘poor risk’ studies. J Clin Oncol 6: 786 – 792
metastatic ‘IGCCCG poor-prognosis’ germ-cell cancer: an explorative
Bajorin DF, Geller NL, Bosl GJ (1991) Assessment of risk in metastatic testis
analysis using cart modeling. Ann Oncol 11: 1115 – 1120
carcinoma: impact on treatment. Urol Int 46: 298 – 303
LeBlanc M, Crowley J (1992) Relative risk trees for censored survival data.
Bokemeyer C, Kollmannsberger C, Meisner C, Harstrick A, Beyer J, Metzner
B, Hartmann JT, Schmoll HJ, Einhorn L, Kanz L, Nichols C (1999) First-
Little R (1992) Regression with missing X’s: a review. J Am Statist Assoc 87:
line high-dose chemotherapy compared with standard-dose PEB/VIP
chemotherapy in patients with advanced germ cell tumors: a multivariate
McCaffrey JA, Bajorin DF, Motzer RJ (1998) Risk assessment for metastatic
and matched-pair analysis. J Clin Oncol 17: 3450 – 3456
testis cancer. Urol Clin North Am 25: 389 – 395
Bokemeyer C, Oechsle K, Hartmann JT, Schoffski P, Schleucher N, Metzner
Mead GM, Stenning SP, Parkinson MC, Horwich A, Fossa SD, Wilkinson
B, Schleicher J, Kanz L (2002) Treatment-induced anaemia and its
PM, Kaye SB, Newlands ES, Cook PA (1992) The Second Medical
potential clinical impact in patients receiving sequential high dose
Research Council study of prognostic factors in nonseminomatous germ
chemotherapy for metastatic testicular cancer. Br J Cancer 87: 1066 – 1071
cell tumors. Medical Research Council Testicular Tumour Working
Bosl GJ, Motzer RJ (1997) Testicular germ-cell cancer. N Engl J Med 337:
Segal MR, Bloch DA (1989) A comparison of estimated proportional
Breiman L, Friedman JH, Olshen RA, Stone CJ (1984) Classification and
hazards models and regression trees. Stat Med 8: 539 – 550
Regression Trees. Belmont, California: Wadsworth
Sonneveld DJ, Hoekstra HJ, van der Graaf WT, Sluiter WJ, Mulder NH,
Clark TG, Altman DG (2003) Developing a prognostic model in the
Willemse PH, Koops HS, Sleijfer DT (2001) Improved long term survival
presence of missing data: an ovarian cancer case study. J Clin Epidemiol
of patients with metastatic nonseminomatous testicular germ cell
carcinoma in relation to prognostic classification systems during the
Clayton D, Hills M (1993) In Statistical Models in Epidemiology, pp 242 –
Steele GS, Richie JP, Stewart AK, Menck HR (1999) The National Cancer
de Wit R, Roberts JT, Wilkinson PM, de Mulder PH, Mead GM, Fossa SD,
Data Base report on patterns of care for testicular carcinoma, 1985 – 1996.
Cook P, de Prijck L, Stenning S, Collette L (2001) Equivalence of three or
four cycles of bleomycin, etoposide, and cisplatin chemotherapy and of a
Steyerberg EW, Eijkemans MJ, Harrell Jr FE, Habbema JD (2000)
3- or 5-day schedule in good-prognosis germ cell cancer: a randomized
Prognostic modelling with logistic regression analysis: a comparison of
study of the European Organization for Research and Treatment of
selection and estimation methods in small data sets. Stat Med 19:
Cancer Genitourinary Tract Cancer Cooperative Group and the Medical
Research Council. J Clin Oncol 19: 1629 – 1640
Steyerberg EW, Harrell Jr FE, Borsboom GJ, Eijkemans MJ, Vergouwe Y,
Efron B, Tibshirani RJ (1993) An Introduction to the Bootstrap. London:
Habbema JD (2001) Internal validation of predictive models: efficiency of
some procedures for logistic regression analysis. J Clin Epidemiol 54:
Harrell Jr FE, Lee KL, Califf RM, Pryor DB, Rosati RA (1984) Regression
modelling strategies for improved prognostic prediction. Stat Med 3:
Therneau T, Grambsch P, Fleming T (1990) Martingale based residuals for
survival models. Biometrika 77: 147 – 160
Harrell Jr FE, Lee KL, Mark DB (1996) Multivariable prognostic models:
van Buuren S, Boshuizen HC, Knook DL (1999) Multiple imputation of
issues in developing models, evaluating assumptions and adequacy, and
missing blood pressure covariates in survival analysis. Stat Med 18:
measuring and reducing errors. Stat Med 15: 361 – 387
British Journal of Cancer (2004) 90(6), 1176 – 1183
A review of the development of the IGCC classificationMR van Dijk et al
5-year survival estimates and number of patients are given for all 108 combinations of the IGCC risk factors based on a Cox regression model of
the IGCC risk factors and interactions AFP and primary site, AFP and NPVM, HCG and NPVM, and HCG and LDH
Surv ¼ 5-year survival; N ¼ number of patients. Classification into three groups; good prognosis 5-year survival 490%, intermediate prognosis 5-year survival 65 – 89%, poorprognosis 5-year survival o65%. Classification into five groups; good prognosis 5-year survival 490%, intermediate prognosis 5-year survival 75 – 89%, good-poor prognosis 5-year survival 60 – 74%, intermediate-poor prognosis 5-year survival 40 – 59%, Poor-poor prognosis 5-year survival o40%.
British Journal of Cancer (2004) 90(6), 1176 – 1183
Mcneil Consumer Healthcare Recalls Four Product Lots of Benadryl® Allergy Ultratab™ Tablets, 100 Count, and One Product Lot of Extra Strength Tylenol® Rapid Release Gels, 50 Count Contact: Bonnie Jacobs 215-273-8994 Marc Boston 215-273-7649 FOR IMMEDIATE RELEASE - Fort Washington, PA - June 15, 2010 - McNeil Consumer Healthcare, Division of McNEIL-PPC, Inc., is recalling
Statistics Concentration)M. S. (Applied Statistics)University of the Philippines at Diliman, 1985Department of BiostatisticsUniversity of Alabama at Birmingham, Oct 2008 – presentCenter for Cardiovascular BiologyUniversity of Alabama at Birmingham, November 2010 – presentCenter for AIDS ResearchUniversity of Alabama at Birmingham, May 2008 – presentDepartment of BiostatisticsUniversity
 British Journal of Cancer (2004) 90, 1176 – 1183
All rights reserved 0007 – 0920/04 $25.00
Survival of patients with nonseminomatous germ cell cancer: areview of the IGCC classification by Cox regression and recursivepartitioning
MR van Dijk*,1, EW Steyerberg1, SP Stenning2, E Dusseldorp3 and JDF Habbema1
Department of Public Health, Erasmus MC – University Medical Center Rotterdam, PO Box 1738, 3000 DR Rotterdam, The Netherlands; 2Medical
Research Council, Clinical Trials Unit, 222 Euston Road, London, NW1 2DA, UK; 3Data Theory Group, Department of Education, Leiden University, PO
Box 9555, 2300 RB Leiden, The Netherlands
The International Germ Cell Consensus (IGCC) classification identifies good, intermediate and poor prognosis groups among patients
with metastatic nonseminomatous germ cell tumours (NSGCT). It uses the risk factors primary site, presence of nonpulmonary
visceral metastases and tumour markers alpha-fetoprotein (AFP), human chorionic gonadotrophin (HCG) and lactic dehydrogenase
(LDH). The IGCC classification is easy to use and remember, but lacks flexibility. We aimed to examine the extent of any loss in
discrimination within the IGCC classification in comparison with alternative modelling by formal weighing of the risk factors. We
analysed survival of 3048 NSGCT patients with Cox regression and recursive partitioning for alternative classifications. Good,
intermediate and poor prognosis groups were based on predicted 5-year survival. Classifications were further refined by subgrouping
within the poor prognosis group. Performance was measured primarily by a bootstrap corrected c-statistic to indicate discriminative
ability for future patients. The weights of the risk factors in the alternative classifications differed slightly from the implicit weights in the
IGCC classification. Discriminative ability, however, did not increase clearly (IGCC classification, c ¼ 0.732; Cox classification,
c ¼ 0.730; Recursive partitioning classification, c ¼ 0.709). Three subgroups could be identified within the poor prognosis groups,
resulting in classifications with five prognostic groups and slightly better discriminative ability (c ¼ 0.740). In conclusion, the IGCC
classification in three prognostic groups is largely supported by Cox regression and recursive partitioning. Cox regression was the
most promising tool to define a more refined classification.
British Journal of Cancer (2004) 90, 1176 – 1183
All rights reserved 0007 – 0920/04 $25.00
Survival of patients with nonseminomatous germ cell cancer: areview of the IGCC classification by Cox regression and recursivepartitioning
MR van Dijk*,1, EW Steyerberg1, SP Stenning2, E Dusseldorp3 and JDF Habbema1
Department of Public Health, Erasmus MC – University Medical Center Rotterdam, PO Box 1738, 3000 DR Rotterdam, The Netherlands; 2Medical
Research Council, Clinical Trials Unit, 222 Euston Road, London, NW1 2DA, UK; 3Data Theory Group, Department of Education, Leiden University, PO
Box 9555, 2300 RB Leiden, The Netherlands
The International Germ Cell Consensus (IGCC) classification identifies good, intermediate and poor prognosis groups among patients
with metastatic nonseminomatous germ cell tumours (NSGCT). It uses the risk factors primary site, presence of nonpulmonary
visceral metastases and tumour markers alpha-fetoprotein (AFP), human chorionic gonadotrophin (HCG) and lactic dehydrogenase
(LDH). The IGCC classification is easy to use and remember, but lacks flexibility. We aimed to examine the extent of any loss in
discrimination within the IGCC classification in comparison with alternative modelling by formal weighing of the risk factors. We
analysed survival of 3048 NSGCT patients with Cox regression and recursive partitioning for alternative classifications. Good,
intermediate and poor prognosis groups were based on predicted 5-year survival. Classifications were further refined by subgrouping
within the poor prognosis group. Performance was measured primarily by a bootstrap corrected c-statistic to indicate discriminative
ability for future patients. The weights of the risk factors in the alternative classifications differed slightly from the implicit weights in the
IGCC classification. Discriminative ability, however, did not increase clearly (IGCC classification, c ¼ 0.732; Cox classification,
c ¼ 0.730; Recursive partitioning classification, c ¼ 0.709). Three subgroups could be identified within the poor prognosis groups,
resulting in classifications with five prognostic groups and slightly better discriminative ability (c ¼ 0.740). In conclusion, the IGCC
classification in three prognostic groups is largely supported by Cox regression and recursive partitioning. Cox regression was the
most promising tool to define a more refined classification. A review of the development of the IGCC classificationMR van Dijk et al
International Germ Cell Consensus Classification for nonsemi-
Centres participating in the International Germ Cell Collaborative
Group provided retrospective data of 5202 adult male patients with
NSGCT. All patients were treated between 1975 and 1990 with
cisplatin-based chemotherapy. Data were collected on age, primary
AFP good ¼ 0 and HCG good ¼ 0 and LDH good ¼ 0
site, date of diagnosis, levels of serum AFP, HCG and LDH, nodal
disease in the abdomen, mediastinum, and neck, lung metastases,spread to other visceral sites like liver, bone and brain and on
treatment details like previous therapy. For the development of the
IGCC classification, patients without missing data on the risk
factors primary site, NPVM, tumour markers AFP, HCG and LDH
and the outcome survival were selected (n ¼ 3048) (IGCCCG,
AFP intermediate ¼ 1 or HCG intermediate ¼ 1 or LDH intermediate ¼ 1
The outcome measures were PFS and overall survival from the
start of the chemotherapy. The risk factors in the IGCC
classification were primary site (testis/retroperitoneal vs medias-
AFP poor ¼ 2 or HCG poor ¼ 2 or LDH poor ¼ 2
tinum), presence of NPVM (yes/no) and tumour markers AFP,
HCG and LDH. Each tumour marker had three categories; good,
Tumour markers AFP/HCG/LDH: Good – AFP o1000 ng mlÀ1, HCG o5000 iu lÀ1,
intermediate and poor with specific cutoff points on the
LDH o1.5 Â upper limit of normal; Intermediate – AFP 1000 – 10000 ng mlÀ1, HCG
continuous tumour markers (see Table 1) (IGCCCG, 1997). The
5000 – 50000 ng mlÀ1, LDH 1.5 – 10 Â N; Poor – AFP 410000 ng mlÀ1, HCG
same risk factors and categories were used to construct the
alternative classifications based on Cox regression and recursivepartitioning.
A review of the development of the IGCC classificationMR van Dijk et al
International Germ Cell Consensus Classification for nonsemi-
Centres participating in the International Germ Cell Collaborative
Group provided retrospective data of 5202 adult male patients with
NSGCT. All patients were treated between 1975 and 1990 with
cisplatin-based chemotherapy. Data were collected on age, primary
AFP good ¼ 0 and HCG good ¼ 0 and LDH good ¼ 0
site, date of diagnosis, levels of serum AFP, HCG and LDH, nodal
disease in the abdomen, mediastinum, and neck, lung metastases,spread to other visceral sites like liver, bone and brain and on
treatment details like previous therapy. For the development of the
IGCC classification, patients without missing data on the risk
factors primary site, NPVM, tumour markers AFP, HCG and LDH
and the outcome survival were selected (n ¼ 3048) (IGCCCG,
AFP intermediate ¼ 1 or HCG intermediate ¼ 1 or LDH intermediate ¼ 1
The outcome measures were PFS and overall survival from the
start of the chemotherapy. The risk factors in the IGCC
classification were primary site (testis/retroperitoneal vs medias-
AFP poor ¼ 2 or HCG poor ¼ 2 or LDH poor ¼ 2
tinum), presence of NPVM (yes/no) and tumour markers AFP,
HCG and LDH. Each tumour marker had three categories; good,
Tumour markers AFP/HCG/LDH: Good – AFP o1000 ng mlÀ1, HCG o5000 iu lÀ1,
intermediate and poor with specific cutoff points on the
LDH o1.5 Â upper limit of normal; Intermediate – AFP 1000 – 10000 ng mlÀ1, HCG
continuous tumour markers (see Table 1) (IGCCCG, 1997). The
5000 – 50000 ng mlÀ1, LDH 1.5 – 10 Â N; Poor – AFP 410000 ng mlÀ1, HCG
same risk factors and categories were used to construct the
alternative classifications based on Cox regression and recursivepartitioning. A review of the development of the IGCC classification
each survival estimate was based is given to indicate the reliability
validated by taking random bootstrap samples (100) (Efron and
Tibshirani, 1993; Harrell et al, 1996).
A review of the development of the IGCC classification
each survival estimate was based is given to indicate the reliability
validated by taking random bootstrap samples (100) (Efron and
Tibshirani, 1993; Harrell et al, 1996). A review of the development of the IGCC classificationMR van Dijk et al
Weights, coding of variables, and cutoff on the max function of
the IGCC classification and the sum score of the regression-based
The final tree fitted by recursive partitioning, using the
exponential scaling method. The 5-year survival rates, events and total
number of observations per subgroup are given. The resulting subgroups
are displayed in rectangulars and determine classification 5T.
A review of the development of the IGCC classificationMR van Dijk et al
Weights, coding of variables, and cutoff on the max function of
the IGCC classification and the sum score of the regression-based
The final tree fitted by recursive partitioning, using the
exponential scaling method. The 5-year survival rates, events and total
number of observations per subgroup are given. The resulting subgroups
are displayed in rectangulars and determine classification 5T.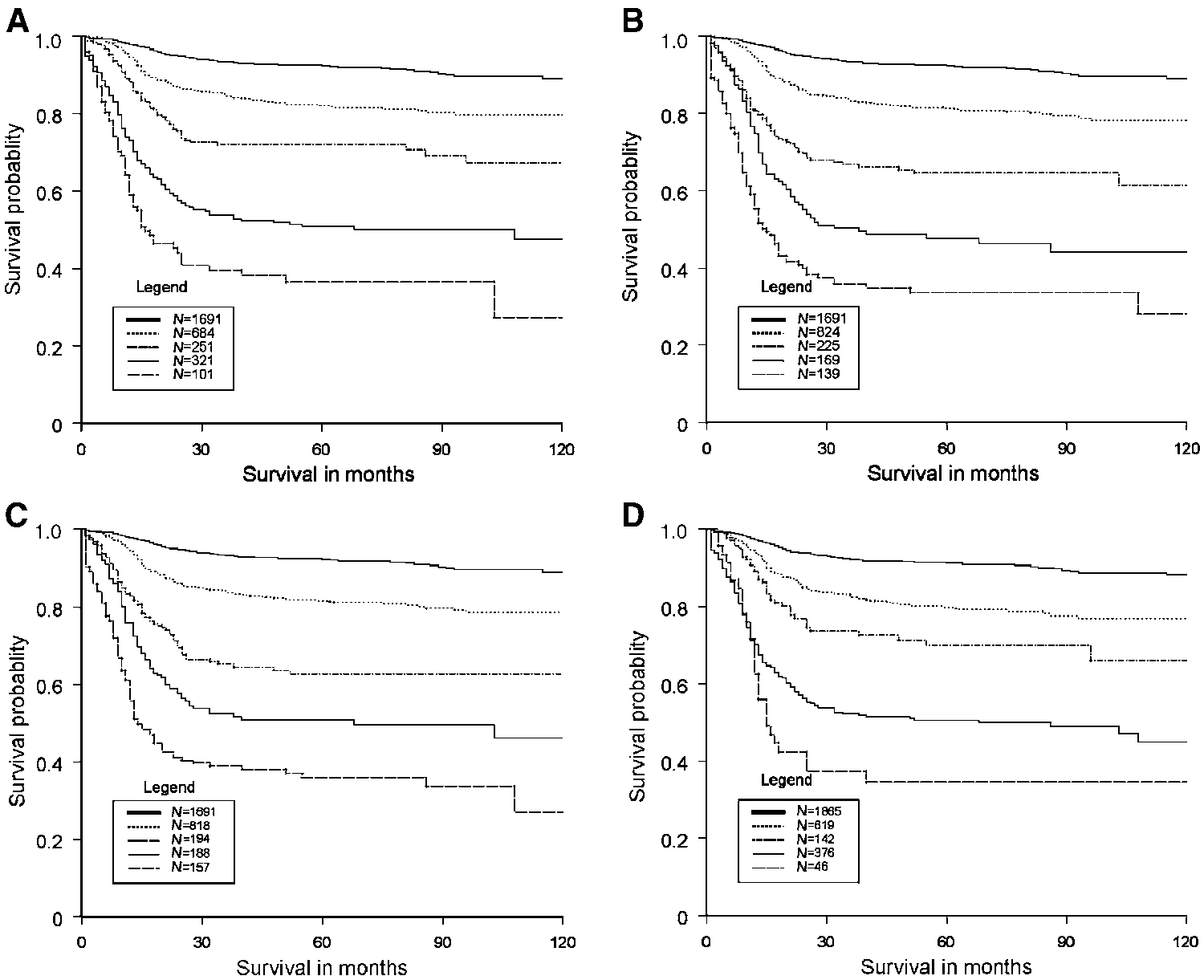
 A review of the development of the IGCC classification
Survival of the IGCC classification, the regression-based classifications 5R and 5Ri and classification 5T based on recursive partitioning
Survival of subgroups within the IGCC classification, the regression-based classifications 5R and 5Ri and classification 5T based on recursive
Surv ¼ 5-year survival. Cutoff points on sum score classification 5R: Good 0, Intermediate 2 – 9, Good – poor 10 – 16, Intermediate – poor 17 – 22, Poor – poor 422.
A review of the development of the IGCC classification
Survival of the IGCC classification, the regression-based classifications 5R and 5Ri and classification 5T based on recursive partitioning
Survival of subgroups within the IGCC classification, the regression-based classifications 5R and 5Ri and classification 5T based on recursive
Surv ¼ 5-year survival. Cutoff points on sum score classification 5R: Good 0, Intermediate 2 – 9, Good – poor 10 – 16, Intermediate – poor 17 – 22, Poor – poor 422. A review of the development of the IGCC classificationMR van Dijk et al
Mead et al, 1992). Some other potentially useful risk factors
The IGCC dataset suffers from a number of limitations. First,
include age, lung metastases and abdominal mass size. However,
not all data were used for the multivariable regression
adding these three risk factors to the Cox model had no substantial
models because of missing data. When patients with missing
effect on discriminative ability (c increased from 0.73 to 0.74). One
data differ from the other patients on prognosis, this causes a bias
could also consider using continuous codings of tumour markers,
in the regression coefficients and the estimated 5-year survival
but this would lead to an undesirable increase in complexity and
rates (Little, 1992; van Buuren et al, 1999; Clark and Altman,
2003). Secondly, we could not internally validate the IGCC
The division into more prognostic groups is similar to another
classification, because the exact steps taken in the modelling
division by recursive partitioning of poor prognosis patients
process (selection and categorisation of risk factors) were not
(Kollmannsberger et al, 2000). Kollmannsberger et al identified
defined. The IGCC classification was applied to a 30% validation
three prognosis groups: a good-poor, intermediate-poor and poor-
set (IGCCCG, 1997), and although the proportion of patients in
poor risk group with 2-year survival rates of 84, 64 and 49%,
each prognostic group was similar, the 5-year survival for
respectively. These survival rates are higher than the survival rates
poor prognosis patients was higher (57%). We did internally
of the good-poor, intermediate-poor and poor-poor risk groups
validate the modelling steps of the Cox regression models and
identified in the IGCC dataset. This may be due to the difference in
found minor optimism in discriminative ability. Classification 5T,
survival for the poor prognosis patients (72 vs 50%), and remains
based on recursive partitioning, however, showed optimism in
when the difference in follow-up time is taken into account (2 vs 5
discriminative ability, as might be expected from a more data-
years). The data in Kollmannsberger et al (2000) are more recent
driven method. This, in combination with the poorer performance,
and improvements in treatment may have led to the difference in
suggests that recursive partitioning is less suitable for the
construction of prognostic classifications. It can be useful,
The lack of improvement in discriminative ability in both the
however, for exploratory analyses in finding interactions between
classifications with three and five groups might also be explained
by the dominance of the good prognosis group, which has a similar
The survival estimates of the IGCC classification were also
survival for all classifications and contains more than half of all
externally validated with more recent data from an MRC/EORTC
patients. We therefore examined whether discriminative ability
trial (N ¼ 300). The 2-year PFS outcome largely corresponded with
increased within the poor prognosis group of each classification.
A review of the development of the IGCC classificationMR van Dijk et al
Mead et al, 1992). Some other potentially useful risk factors
The IGCC dataset suffers from a number of limitations. First,
include age, lung metastases and abdominal mass size. However,
not all data were used for the multivariable regression
adding these three risk factors to the Cox model had no substantial
models because of missing data. When patients with missing
effect on discriminative ability (c increased from 0.73 to 0.74). One
data differ from the other patients on prognosis, this causes a bias
could also consider using continuous codings of tumour markers,
in the regression coefficients and the estimated 5-year survival
but this would lead to an undesirable increase in complexity and
rates (Little, 1992; van Buuren et al, 1999; Clark and Altman,
2003). Secondly, we could not internally validate the IGCC
The division into more prognostic groups is similar to another
classification, because the exact steps taken in the modelling
division by recursive partitioning of poor prognosis patients
process (selection and categorisation of risk factors) were not
(Kollmannsberger et al, 2000). Kollmannsberger et al identified
defined. The IGCC classification was applied to a 30% validation
three prognosis groups: a good-poor, intermediate-poor and poor-
set (IGCCCG, 1997), and although the proportion of patients in
poor risk group with 2-year survival rates of 84, 64 and 49%,
each prognostic group was similar, the 5-year survival for
respectively. These survival rates are higher than the survival rates
poor prognosis patients was higher (57%). We did internally
of the good-poor, intermediate-poor and poor-poor risk groups
validate the modelling steps of the Cox regression models and
identified in the IGCC dataset. This may be due to the difference in
found minor optimism in discriminative ability. Classification 5T,
survival for the poor prognosis patients (72 vs 50%), and remains
based on recursive partitioning, however, showed optimism in
when the difference in follow-up time is taken into account (2 vs 5
discriminative ability, as might be expected from a more data-
years). The data in Kollmannsberger et al (2000) are more recent
driven method. This, in combination with the poorer performance,
and improvements in treatment may have led to the difference in
suggests that recursive partitioning is less suitable for the
construction of prognostic classifications. It can be useful,
The lack of improvement in discriminative ability in both the
however, for exploratory analyses in finding interactions between
classifications with three and five groups might also be explained
by the dominance of the good prognosis group, which has a similar
The survival estimates of the IGCC classification were also
survival for all classifications and contains more than half of all
externally validated with more recent data from an MRC/EORTC
patients. We therefore examined whether discriminative ability
trial (N ¼ 300). The 2-year PFS outcome largely corresponded with
increased within the poor prognosis group of each classification. A review of the development of the IGCC classification
below) for kindly providing their data for the analyses in this
Netherlands). USA: R Motzer (Memorial Sloan-Kettering Cancer
Center, New York), L Finn (University of Texas MD Anderson
MRC: N Aass (Norwegian Radium Hospital, Oslo, Montebello,
Cancer Center). Italy: R Salvioni and L Mariani (Istituto Nazionale
Norway), PI Clark (Clatterbridge Hospital, Liverpool, England),
Tumori, Milan). Spain: P Lianes Barragan (Hospital doce de
MH Cullen (Queen Elizabeth Hospital, Birmingham, England), D
Octubre, Madrid). Denmark: S Werner Hansen (Rigshospitalet,
Dearnaley (Royal Marsden Hospital, Surrey, England), SJ Harland
(Middlesex Hospital, London, England), WG Jones (Yorkshire
Montpellier), J Bouzy (Institut Gustave Roussy, Villejuif).
A review of the development of the IGCC classification
below) for kindly providing their data for the analyses in this
Netherlands). USA: R Motzer (Memorial Sloan-Kettering Cancer
Center, New York), L Finn (University of Texas MD Anderson
MRC: N Aass (Norwegian Radium Hospital, Oslo, Montebello,
Cancer Center). Italy: R Salvioni and L Mariani (Istituto Nazionale
Norway), PI Clark (Clatterbridge Hospital, Liverpool, England),
Tumori, Milan). Spain: P Lianes Barragan (Hospital doce de
MH Cullen (Queen Elizabeth Hospital, Birmingham, England), D
Octubre, Madrid). Denmark: S Werner Hansen (Rigshospitalet,
Dearnaley (Royal Marsden Hospital, Surrey, England), SJ Harland
(Middlesex Hospital, London, England), WG Jones (Yorkshire
Montpellier), J Bouzy (Institut Gustave Roussy, Villejuif). A review of the development of the IGCC classificationMR van Dijk et al
5-year survival estimates and number of patients are given for all 108 combinations of the IGCC risk factors based on a Cox regression model of
the IGCC risk factors and interactions AFP and primary site, AFP and NPVM, HCG and NPVM, and HCG and LDH
Surv ¼ 5-year survival; N ¼ number of patients. Classification into three groups; good prognosis 5-year survival 490%, intermediate prognosis 5-year survival 65 – 89%, poorprognosis 5-year survival o65%. Classification into five groups; good prognosis 5-year survival 490%, intermediate prognosis 5-year survival 75 – 89%, good-poor prognosis 5-year survival 60 – 74%, intermediate-poor prognosis 5-year survival 40 – 59%, Poor-poor prognosis 5-year survival o40%.
A review of the development of the IGCC classificationMR van Dijk et al
5-year survival estimates and number of patients are given for all 108 combinations of the IGCC risk factors based on a Cox regression model of
the IGCC risk factors and interactions AFP and primary site, AFP and NPVM, HCG and NPVM, and HCG and LDH
Surv ¼ 5-year survival; N ¼ number of patients. Classification into three groups; good prognosis 5-year survival 490%, intermediate prognosis 5-year survival 65 – 89%, poorprognosis 5-year survival o65%. Classification into five groups; good prognosis 5-year survival 490%, intermediate prognosis 5-year survival 75 – 89%, good-poor prognosis 5-year survival 60 – 74%, intermediate-poor prognosis 5-year survival 40 – 59%, Poor-poor prognosis 5-year survival o40%.