Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Doi:10.1016/j.fertnstert.2003.11.057
FERTILITY AND STERILITY
Copyright 2004 American Society for Reproductive Medicine
Printed on acid-free paper in U.S.A. Platelet-activating factor significantly enhances intrauterine insemination pregnancy rates in non-male factor infertility William E. Roudebush, Ph.D., Andrew A. Toledo, M.D., Hilton I. Kort, M.D.,Dorothy Mitchell-Leef, M.D., Carlene W. Elsner, M.D., and Joe B. Massey, M.D.Reproductive Biology Associates, Atlanta, GeorgiaObjective: To determine the efficacy of treating semen specimens with platelet-activating factor (PAF) before IUI. Design: Prospective randomized double-blinded study of PAF treatment of sperm for patients with a history of infertility undergoing IUI. Setting: Private infertility center. Intervention(s): Patients had ovulation induction therapy with clomiphene citrate (CC) or gonadotropin, two IUIs per month with PAF treatment. Main Outcome Measure(s): Clinical pregnancy rates. Result(s): There was a significant difference in IUI pregnancy rates per cycle between control (10/56; 17.9%) and PAF (14/47; 29.8%) treatment groups in the normal male study arm. There was a significant difference in cumulative IUI pregnancy rates between control (10/35; 28.6%) and PAF (14/26; 53.9%) patient groups in the normal male study arm. There was no significant difference in IUI pregnancy rates per cycle between control (12/124; 9.7%) and PAF (14/119; 11.8%) treatment groups in the male factor study arm. There was no significant difference in cumulative IUI pregnancy rates between control (12/46; 26.1%) and PAF (14/38; 36.8%) patient groups in the male factor study arm. There was a significant difference in overall cumulative IUI pregnancy rates between control (21/81; 25.9%) and PAF (27/64; 42.2%) patient groups. Conclusion(s): The inclusion of PAF into the IUI sperm wash procedure significantly improves pregnancy rates. However, the significant improvement can only be shown to affect men presenting with normal semen parameters. (Fertil Steril 2004;82:52– 6. 2004 by American Society for Reproductive Medicine.) Key Words: Platelet-activating factor, intrauterine insemination, sperm, pregnancy
IUI cycles followed by gonadotropin/IUI for up
induction followed by intrauterine insemina-
to three cycles. Failed IUI therapy subsequently
tion (IUI) has become standard therapy for
results in consideration of IVF therapy. Silver-
Presented in part (O-222)at the 58th Annual Meeting
nontubal factor-related infertility. The initial
berg et al. have shown that two IUI proce-
treatment for infertile couples is IUI and is
dures per cycle have improved pregnancy rates,
Reproductive Medicine,Seattle, WA, October 12–
although this continues to be controversial
dependent on the ovulation induction regimen
Male fertility requires production of an ad-
lative pregnancy rates for three cycles have
sperm with sufficient motility and the ability to
approached those of a single IVF treatment
undergo capacitation and the acrosome reac-
when gonadotropins are combined with IUI
tion to penetrate the oocyte’s cumulus oopho-
Atlanta, Georgia 30342(FAX: 404-256-8376;
Commonly, because of lower patient costs,
rus and zona pellucida for fertilization. Defects
complexity and risks of high order multiple
in any of these necessary events may lead to
pregnancy (i.e., triplets or more), clomiphene
subfertility or infertility. Recently, for exam-
citrate (CC) is initially used. In our center the
ple, chromatin integrity of sperm was found to
doi:10.1016/j.fertnstert.2003. 11.057
typical treatment regimen involves three CC/
A number of endogenous biochemical factors have been
completed. Cycle stimulation was controlled by CC or go-
attributed to regulate the fertility potential of spermatozoa,
nadotropins. In CC-controlled cycles, 50 –150 mg of CC was
for example, platelet-activating factor (PAF). Platelet-acti-
given for 5 cycle days. Timing of IUI was based on LH surge
vating factor is a unique and novel signaling phospholipid
or ultrasound-timed hCG administration. In cycles managed
that has pleiotropic biologic properties in addition to platelet
by gonadotropins, stimulations were started on cycle day 3
activation. Since its discovery in the early 1970s this novel
with 75–225 IU daily (with dosages individually titrated
compound has been implicated in a variety of reproductive
based on patient age and previous response). Ultrasound
functions including fertilization, implantation, and parturi-
(one to four ultrasound follicular studies per IUI cycle)
tion The exact mechanism is uncertain, yet its impor-
monitoring with E (Access2, Beckman Coulter, Inc., Brea,
tance in normal fertility is significant.
CA) observation was performed until the lead follicle was at
Platelet-activating factor is present in human spermatozoa
least 18 mm in all but exceptional cases. Preovulatory LH
and its endogenous content has a significant and positive
surge timing was monitored by urine LH levels. The IUI was
relationship with motility and pregnancy rate Exogenous
performed 12–18 hours and again in 36 –38 hours after hCG
PAF has been used to stimulate human sperm motility
injection. Patients taking CC who experienced a spontaneous
and IVF and embryo development rates in rabbits A
LH surge had only one IUI performed 24 hours later.
preliminary study demonstrated the improvement of IUI
Semen Analysis
pregnancy rates after a short-term exposure of sperm to PAF.
Semen specimens were permitted to liquefy for 30 – 60 min-
In the present study, our objective was to determine the
utes at 37°C. Sperm concentration and motility, before and after
effect of exogenous PAF on IUI pregnancy rates in couples
treatment, were evaluated by computer-assisted semen analysis
presenting with normal and abnormal semen analyses. The
(IVOS v10.9i, Hamilton-Thorne Research, Beverly, MA) opera-
study was a prospective randomized double-blinded study of
ting at a sampling frequency of 60 Hz. All analyses were per-
PAF treatment of sperm for patients with a history of infer-
formed using MicroCell-20 Micron (Conception Technologies,
tility undergoing IUI. Patients were randomized (blind num-
San Diego, CA) counting chambers. A total of five random
ber draw from computer-generated random number table)
areas were selected and evaluated by the IVOS system at 37°C.
into either receiving PAF treatment or serving as controls for
Semen Processing and PAF Exposure for IUI
up to three IUI cycles. Furthermore, couples were catego-rized into either normal or male factor groups. Control Group MATERIALS AND METHODS
Semen specimens were processed (400 g; 12 minutes)
through a 90% density silane-coated silica suspension (1:1;
Study Population and Management
Promotor; CERES Fertility, San Diego, CA), washed with 4
Healthy, infertile patients with nontubal factor infertility
mL of sperm wash medium (InVitroCare, San Diego, CA),
were made aware of the study and informed of the study
centrifuged (300 g; 8 minutes) and resuspended with 0.5 mL
design with the possibility of improved results based on a
of PureSperm-Wash (Nidacon International AB, Goteborg,
small clinical trial The PAF treatment option was not
made available outside the current study. Possible risks were
PAF Treatment Group
discussed and informed consent was obtained under guide-lines approved by the Western Institutional Review Board
Semen specimens were processed (400 g; 12 minutes)
(Seattle, WA). Inclusion criteria were as follows: basal FSH
through a 90% density silane-coated silica suspension (1:1;
level Ͻ15 mIU/mL, evidence of a normal uterine cavity, and
Promotor), resuspended in 10Ϫ7M PAF in sperm wash medium
no contraindication to pregnancy. Infertility diagnoses in-
(InVitroCare) and incubated for 15 minutes at 37°C. After
cluded anovulatory, endometriosis, idiopathic, tubal (single
incubation, sperm were washed (300 g; 8 minutes) free of PAF
or fibroids), cervical factor, and male factor. Male factor
and resuspended in 0.5 mL of PureSperm-Wash (Nidacon).
infertility patients were classified as such if they failed to
IUI and Pregnancy Outcomes
meet one or more reference standards Couples were
Washed sperm preparations were inseminated with an IUI
permitted to enter the study at any point in a series of IUI
Catheter (Lifetek Medical, Inc., Portage, WI). Pregnancy
treatments. Couples (normal male and male factor study
outcomes were determined first by -hCG serum levels
groups) were randomized into one of two study groups
(Access2, Beckman Coulter, Inc.) and confirmed by ultra-
(group 1, control; group 2, PAF) from January 2001 to
sonography (fetal heartbeat ϭ a positive outcome).
December 2002. Once patients were assigned to the respec-tive treatment group, only the RBA Andrology Laboratory
Sample Size and Statistical Analysis
staff was aware of assignment. Patients were subsequently
Power estimates based on published IUI pregnancy rates
treated in each consecutive cycle with the same regimen (i.e.,
(5%–16%) and preliminary data reveal that a minimal sam-
control or PAF augmented). No clinical staff (physician or
ple size of 83 IUI cycles per male factor and 40 IUI cycles
nurse) was informed of assignment until the study was
per normal male treatment group is required for alpha to equal
FERTILITY & STERILITY
Platelet activating factor-intrauterine insemination patient
Cumulative Platelet activating factor-intrauterine
Control, 36.4 (Ϯ3.01); PAF, 35.5 (Ϯ4.02)
Control, 38.5 (Ϯ6.01); PAF, 36.0 (Ϯ5.94)
Control, 36.2 (Ϯ4.16); PAF, 35.9 (Ϯ4.93)
Control, 35.8 (Ϯ4.54); PAF, 34.1 (Ϯ4.40)
a,b,cSimilar superscripts are significantly different, PϽ.05. Roudebush. Platelet-activating factor and IUI pregnancy. Fertil Steril 2004.
enrolled in the study, of these 3 (1.8%) converted to IVF and
17 (10.3%) never followed through with IUI therapy.
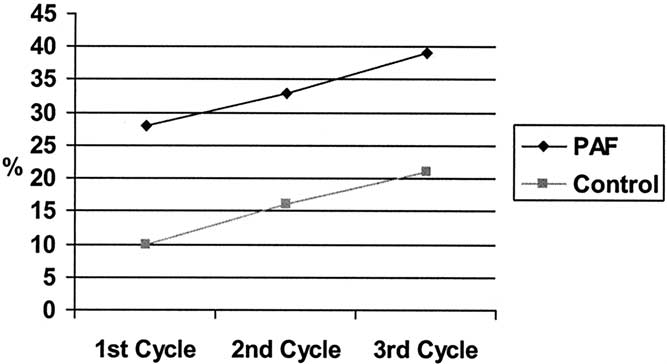
Patient pregnancy rates are presented in (per
Roudebush. Platelet-activating factor and IUI pregnancy. Fertil Steril 2004.
cycle) and (cumulative). Cumulative IUI pregnancyrate by number of attempts according to treatment group for
0.05 and to show a difference with 80% power (beta ϭ 0.80).
all patients (normal and male factor) are presented in Figure
A 50% increase in pregnancy rate after treatment to the IUI
1. In couples presenting with normal semen characteristics
protocol was used. Data were analyzed by 2. Statistical calcu-
the cycle-specific pregnancy rate was 29.8% (14/47) when
lations were performed with SigmaStat for Windows, ver-
PAF was used. This was significantly higher (PϽ.05) when
sion 2.03 (Jandel Scientific Corporation, San Rafael, CA).
compared with the control (10/56; 17.9%). Cumulative preg-nancy rates were significantly higher (PϽ.05) in the PAF
treatment group (14/26; 53.90%) than the control group(10/35; 28.6%). There was no significant difference in IUI
A prospective comparison of pregnancy rates was performed
pregnancy rates per cycle between control (12/124; 9.7%)
after sperm treatment with or without PAF, at the time of semen
and PAF (14/119; 11.8%) treatment groups in the male
washing just before IUI. Patient demographics are presented in
factor study arm. There was no significant difference in
There were no significant differences in patient
cumulative IUI pregnancy rates between control (12/46;
demographics between the pregnant and nonpregnant groups
26.1%) and PAF (14/38; 36.8%) patient groups in the male
or control and PAF treatment groups. A total of 165 patients
factor study arm. There was a significant difference (PϽ.05)in overall cumulative IUI pregnancy rates between control(22/81; 27.2%) and PAF (28/64; 43.8%) patient groups.
Platelet activating factor-intrauterine inseminationpregnancy rate per cycle.
Platelet activating factor-intrauterine inseminationmultiple pregnancy rate.
Significantly different, PϽ.05. Roudebush. Platelet-activating factor and IUI pregnancy. Fertil Steril 2004.Roudebush. Platelet-activating factor and IUI pregnancy. Fertil Steril 2004.Roudebush et al.
Platelet-activating factor and IUI pregnancy
Cumulative intrauterine insemination (IUI) pregnancy rate by
Ongoing platelet activating factor-intrauterine
number of attempts according to treatment group for all
patients (normal and male factor). PAF ϭ platelet-activating
Roudebush. Platelet-activating factor and IUI pregnancy. Fertil Steril 2004.
cells’ surface, initiating intracellular calcium release, en-hancing sperm capacitation and cell motility, thus enhancingfertilization rates. Sperm with defective or low numbers ofPAF receptor may not respond to PAF (endogenous orexogenous), thus having poor motility Additional stud-ies will elucidate the reproductive significance of PAF ac-
Roudebush. Platelet-activating factor and IUI pregnancy. Fertil Steril 2004.
tivity and PAF’s mechanism of action in spermatozoa. Otherpossible factors may attribute to the high pregnancy ratesobserved in this study. For example, in most cases we
There was no significant difference in multiple pregnancy rates
performed two IUI’s per cycle, which has been demonstrated
between the control and PAF treatment groups
Additional clinical studies are warranted to further estab-
DISCUSSION
lish the use of PAF therapy for patient’s undergoing IUI
The inclusion of PAF to IUI sperm wash procedure im-
therapy for infertility treatment. In particular, larger numbers
proves pregnancy rates. However, this significant improve-
of male factor infertility patients will determine the signifi-
ment could only be demonstrated in cases where the semen
cance of PAF–IUI therapy for these individuals. To summa-
analysis was normal. This confirms our original results dem-
rize, exposure of sperm to PAF can significantly increase IUI
onstrating the effectiveness of exogenous PAF supplemen-
Treatment of sperm in male factor patients with PAF
APPENDUM
showed an increase in pregnancy rates, albeit not statistically
On February 10, 2003, we initiated the routine washing of
significant. It is possible that sperm in these individuals are
semen with PAF before IUI. Our overall ongoing pregnancy
incapable of responding to the exogenous PAF due to poor
rate since then is 41.6% and is presented in
PAF receptor levels and, or faulty PAF receptors in thesperm The PAF antagonists will inhibit the motility,acrosome reaction and hamster oocyte penetration in ex-posed sperm, thus suggesting the presence of receptors forPAF We have recently reported on the presence anddistribution of the PAF receptor in human sperm and
Acknowledgments: The authors express their sincere gratitude and thanks to
our preliminary data demonstrate that distribution of the
the staff and physicians (Daniel Shapiro, M.D., David Keenan, M.D., and
receptor is significantly altered in abnormal sperm We
Scott Slayden, M.D.) at Reproductive Biology Associates for patient re-
have also discovered that PAF receptor mRNA expression
cruitment and laboratory work without whose assistance would have madethis study impossible.
differs significantly between motile (high content) and non-motile (low content) sperm In addition we have foundthat sperm with abnormal motility have different PAF recep-
References
tor mRNA sequences The PAF plays a significant role
1. Garceau L, Henderson J, Davis LJ, Petrou S, Henderson LR, McVeigh
E, et al. Economic implications of assisted reproductive techniques: a
in sperm function and has recently been reviewed It
systematic review. Hum Reprod 2002;12:3090 –109.
may affect sperm motility and fertilization through a recep-
2. Ecochard R, Mathieu C, Royere D, Blache G, Rabilloud M, Czyba JC.
A randomized prospective study comparing pregnancy rates after clo-
tor-mediated control of intracellular calcium. The PAF has
miphene citrate and human menopausal gonadotropin before intrauter-
been shown to augment sperm capacitation
ine insemination. Fertil Steril 2000;73:90 –3.
3. Pasqualotto EB, Daitch JA, Hendin BN, Falcone T, Thomas AJ, Nelson
We believe that the beneficial effect of PAF on IUI
DR, et al. Relationship to total motile sperm count and percentagemotile sperm to successful pregnancy rates following intrauterine in-
pregnancy rates is due to PAF binding to its receptor on the
semination. J Assisted Reprod Genetics 1999;16:476 –82. FERTILITY & STERILITY
4. Matorras R, Diaz T, Corcostegui B, Ramon O, Pijoan JI, Rodriguez-
Programme for Research Development and Research Training in Hu-
Escudero FJ. Ovarian stimulation in intrauterine insemination with
man Reproduction: Cambridge University Press, Cambridge, UK 1999.
donor sperm: a randomized study comparing clomiphene citrate in fixed
15. Purnell ET, Roudebush WE. Platelet-activating factor activity (ligand
protocol versus highly purified urinary FSH. Hum Reprod 2002;8:
and receptor transcript) content in sperm: motile versus nonmotile. In:
Robaire E, Chemes H, Morales CR, eds. Andrology in the 21st century,
5. Silverberg KM, Johnson JV, Olive DL, Burns WN, Schenken RS. A
Proceedings of the VIIth International Congress of Andrology. Engle-
prospective, randomized trial comparing two different intrauterine in-
wood, NJ: Medimond Publishing Company, Inc., 2001:71–6.
semination regimens in controlled ovarian hyperstimulation cycles.
16. Sengoku K, Tamate K, Takaoka Y, Ishikawa M. Effects of platelet-
activating factor on human sperm function in vitro. Hum Reprod
6. Cantineau AE, Heineman MJ, Cohlen BJ. Single versus double intra-
uterine insemination in stimulated cycles for subfertile couples: a
17. Minhas BS. Platelet-activating factor treatment of human spermatozoa
systematic review based on a Cochrane review. Hum Reprod 2003;18:
7. Duran EH, Morshedi M, Taylor S, Oehninger S. Sperm DNA quality
18. Reinhardt JC, Cui X, Roudebush WE. Immunofluorescent evidence for
predicts intrauterine insemination outcome: a prospective cohort study.
the presence of the platelet-activating factor receptor in human sper-
matozoa. Fertil Steril 1999;71:941–2.
8. Harper MJK. Platelet-activating factor: a paracrine factor in preimplan-
19. Roudebush WE, Wild MD, Maguire EH. Platelet-activating factor
tation stages of development? Biol Reprod 1989;40:907–13.
receptor expression in human spermatozoa: differences in mRNA con-
9. Minhas BS, Kumar R, Ricker DD, Robertson JL, Dodson MG. The
presence of platelet activating factor-like activity in human spermato-
tent and protein distribution between normal and abnormal spermato-
zoa. Fertil Steril 2000;73:967–71.
10. Roudebush WE, Purnell ET. Platelet-activating factor content in human
20. Roudebush WE, Mayorov V, Adkison LR, Slayden SM, Shapiro DB,
spermatozoa: predicting pregnancy outcome. Fertil Steril 2000;74:257–
Elsner CW, et al. Abnormal sequence of the platelet-activating factor-
receptor in nonmotile spermatozoa. Fertil Steril 2002;76:P-460.
11. Ricker DD, Minhas BS, Kumar R, Robertson JL, Dodson MG. The
21. Levine AS, Kort HI, Toledo AA, Roudebush WE. A review of the
effects of platelet activating factor on the motility of human spermato-
effect of platelet-activating factor on male reproduction and sperm
12. Roudebush WE, Fukuda AI, Minhas BS. Enhanced embryo develop-
22. Wu C, Stojanov T, Chami O, Ishii S, Shimizu T, Li A, et al. Evidence
ment of rabbit oocytes fertilized in vitro with platelet-activating factor
for the autocrine induction of capacitation of mammalian spermatozoa.
treated spermatozoa. J Assisted Reprod Genet 1993;10:91–4.
13. Wild MD, Roudebush WE. Platelet-activating factor improves intra-
23. Toledo AA, Mitchell-Leef D, Elsner CW, Slayden SM, Roudebush
uterine insemination outcome. Am J Obstet Gynecol 2001;184:1064 –5.
WE. Fertilization potential of human sperm is correlated with endog-
14. WHO Laboratory Manual. The examination of human semen and
enous platelet-activating factor content. J Assist Reprod Genet 2003;
sperm– cervical mucus interaction. 4th ed. Prepared by WHO Special
Roudebush et al.
Platelet-activating factor and IUI pregnancy
Ein innovativer Ansatz zur Bestimmung der Kosten-Effektivität und der Budgetauswirkung neuer Wirkstoffe am Beispiel von Rimonabant Aidelsburger P1, Fuchs S1, Moock J2, Hessel F3, Mangiapane S4, Gothe H4, Kohlmann T2, Wasem J3 1CAREM GmbH, Deutschland 2Institut für Community Medicine, Ernst-Moritz-Arndt Universität Greifswald, Deutschland 3Lehrstuhl für Medizinmanagement, Universität
132 (2013), p. 139 -149. ALGEBRAIC AND TOPOLOGICAL STRUCTURES ON THE SET OF MEAN FUNCTIONS AND GENERALIZATION OF THE AGM MEAN Abstract. In this paper, we present new structures and results on theset MD of mean functions on a given symmetric domain D in R2. First,we construct on MD a structure of abelian group in which the neutralelement is the arithmetic mean; then we study som



 Platelet activating factor-intrauterine insemination patient
Cumulative Platelet activating factor-intrauterine
Control, 36.4 (Ϯ3.01); PAF, 35.5 (Ϯ4.02)
Control, 38.5 (Ϯ6.01); PAF, 36.0 (Ϯ5.94)
Control, 36.2 (Ϯ4.16); PAF, 35.9 (Ϯ4.93)
Control, 35.8 (Ϯ4.54); PAF, 34.1 (Ϯ4.40)
a,b,cSimilar superscripts are significantly different, PϽ.05.
Platelet activating factor-intrauterine insemination patient
Cumulative Platelet activating factor-intrauterine
Control, 36.4 (Ϯ3.01); PAF, 35.5 (Ϯ4.02)
Control, 38.5 (Ϯ6.01); PAF, 36.0 (Ϯ5.94)
Control, 36.2 (Ϯ4.16); PAF, 35.9 (Ϯ4.93)
Control, 35.8 (Ϯ4.54); PAF, 34.1 (Ϯ4.40)
a,b,cSimilar superscripts are significantly different, PϽ.05.
 Cumulative intrauterine insemination (IUI) pregnancy rate by
Ongoing platelet activating factor-intrauterine
number of attempts according to treatment group for all
patients (normal and male factor). PAF ϭ platelet-activating
Roudebush. Platelet-activating factor and IUI pregnancy. Fertil Steril 2004.
cells’ surface, initiating intracellular calcium release, en-hancing sperm capacitation and cell motility, thus enhancingfertilization rates. Sperm with defective or low numbers ofPAF receptor may not respond to PAF (endogenous orexogenous), thus having poor motility Additional stud-ies will elucidate the reproductive significance of PAF ac-
Roudebush. Platelet-activating factor and IUI pregnancy. Fertil Steril 2004.
tivity and PAF’s mechanism of action in spermatozoa. Otherpossible factors may attribute to the high pregnancy ratesobserved in this study. For example, in most cases we
There was no significant difference in multiple pregnancy rates
performed two IUI’s per cycle, which has been demonstrated
between the control and PAF treatment groups
Additional clinical studies are warranted to further estab-
DISCUSSION
Cumulative intrauterine insemination (IUI) pregnancy rate by
Ongoing platelet activating factor-intrauterine
number of attempts according to treatment group for all
patients (normal and male factor). PAF ϭ platelet-activating
Roudebush. Platelet-activating factor and IUI pregnancy. Fertil Steril 2004.
cells’ surface, initiating intracellular calcium release, en-hancing sperm capacitation and cell motility, thus enhancingfertilization rates. Sperm with defective or low numbers ofPAF receptor may not respond to PAF (endogenous orexogenous), thus having poor motility Additional stud-ies will elucidate the reproductive significance of PAF ac-
Roudebush. Platelet-activating factor and IUI pregnancy. Fertil Steril 2004.
tivity and PAF’s mechanism of action in spermatozoa. Otherpossible factors may attribute to the high pregnancy ratesobserved in this study. For example, in most cases we
There was no significant difference in multiple pregnancy rates
performed two IUI’s per cycle, which has been demonstrated
between the control and PAF treatment groups
Additional clinical studies are warranted to further estab-
DISCUSSION