Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Microsoft word - jcphaldo11111.doc
HALDOL® Injection FOR INTRAMUSCULAR INJECTION ONLY PRODUCT INFORMATION NAME OF THE MEDICINE DESCRIPTION
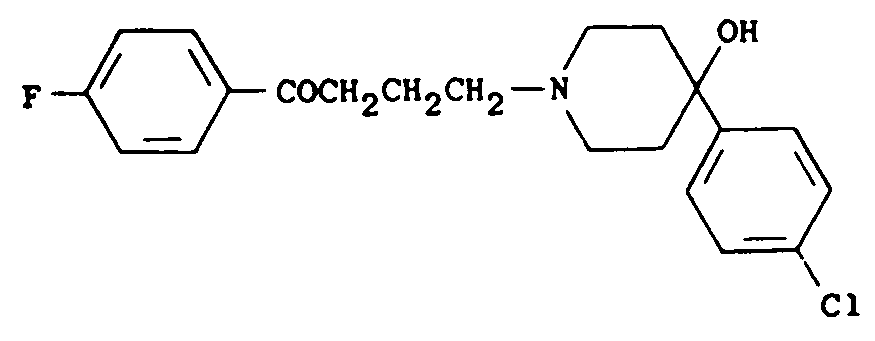
Haloperidol decanoate is the decanoate ester of haloperidol. The structural formula is:
4-(4-chlorophenyl)-1-[4-(4-fluorophenyl)-4-oxobutyl]-4-piperidinyl decanoate
Haloperidol decanoate is almost insoluble in water but is soluble in most organic solvents. Each mL contains 50 mg haloperidol (present as haloperidol decanoate 70.52 mg) in a sesame oil vehicle, with 1.5% w/v benzyl alcohol as a preservative ie: each mL contains 15 mg benzyl alcohol.
PHARMACOLOGY
Haloperidol decanoate is a long-acting form of haloperidol. The basic effects of haloperidol decanoate are the same as those of haloperidol with the exception of duration of action. When it is administered as an intramuscular depot injection in sesame oil, esterases present in the blood and tissues hydrolyse haloperidol decanoate to provide a slow release of the active neuroleptic haloperidol from the depot into the systemic circulation. Haloperidol blocks the effects of dopamine and increases its turnover rate, however the precise mechanism of action is unknown.
Pharmacokinetics
Administration of haloperidol decanoate as a depot IM injection results in a slow and sustained release of haloperidol. The plasma concentrations rise gradually, usually peaking within the first week after injection and falling thereafter with an apparent half-life of about 3 weeks. Steady state plasma levels were reached in 3-6 months in chronic psychotic patients receiving monthly injections. The relationship between dose and plasma haloperidol is roughly linear for doses below 450 mg. It should be noted however, that the pharmacokinetics of haloperidol decanoate following intramuscular injections can be quite variable between subjects. Haloperidol is metabolised in the liver and excreted in the urine and faeces. HALDOL Decanoate
is metabolised by several routes including the cytochrome P450 enzyme system (particularly CYP 3A4 or CYP 2D6) and glucuronidation.
INDICATIONS
HALDOL Decanoate is indicated for the maintenance therapy of psychoses; particularly for patients requiring prolonged parenteral neuroleptic therapy.
CONTRAINDICATIONS
HALDOL Decanoate is contraindicated in comatose states from any cause and in the presence of CNS depression due to alcohol or other depressant drugs. It is also contraindicated in patients with significant depressive states, previous spastic diseases, lesions of the basal ganglia and in Parkinson's syndrome, except in the case of dyskinesias due to levodopa treatment. It should not be used in senile patients with pre-existing Parkinson-like symptoms.
*HALDOL Decanoate is contraindicated in individuals who are hypersensitive to the drug or its excipients (cross reactivity of sesame oil in patients with a peanut allergy may occur). PRECAUTIONS Sudden Death in Elderly Patients with Dementia
Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. Analyses of seventeen placebo-controlled trials (modal duration of 10 weeks), largely in patients taking atypical antipsychotic drugs, revealed a risk of death in drug-treated patients of between 1.6 to 1.7 times the risk of death in placebo-treated patients. Over the course of a typical 10 week controlled trial, the rate of death in drug-treated patients was about 4.5%, compared to a rate of about 2.6% in the placebo group. Although the causes of death were varied, most of the deaths appeared to be either cardiovascular (e.g., heart failure, sudden death) or infectious (e.g., pneumonia) in nature. Observational studies suggest that, similar to atypical antipsychotic drugs, treatment with conventional antipsychotic drugs may increase mortality. The extent to which the findings of increased mortality in observational studies may be attributed to the antipsychotic drug as opposed to some characteristic(s) of the patients is not clear.
Cardiovascular Effects
Very rare reports of QT prolongation and/or ventricular arrhythmias, in addition to cases of sudden death have been reported in patients receiving haloperidol. They may occur more frequently with high doses and in predisposed patients.
Higher than recommended doses and intravenous administration of haloperidol appear to be associated with a higher risk of QT-prolongation and/or ventricular arrhythmias, and Torsades de Pointes (see Interactions with Other Medicines, ADVERSE REACTIONS and OVERDOSAGE). Since QT prolongation has been observed during Haldol Decanoate treatment, it is advised to be particularly cautious in patients with QT-prolonging conditions (QT-syndrome, electrolyte imbalance [especially hypokalaemia and hypomagnesaemia], drugs known to prolong QT, cardiovascular diseases, hypothyroidism, family history of QT prolongation) (see Interactions with other Medicines). HALDOL DECANOATE MUST NOT BE ADMINISTERED INTRAVENOUSLY.
Tachycardia and hypotension have also been reported in occasional patients.
Neuroleptic Malignant Syndrome
As with other neuroleptic drugs, a symptom complex sometimes referred to as neuroleptic malignant syndrome (NMS) has been reported. Cardinal features of NMS are hyperthermia, hyperpyrexia, muscle rigidity, altered mental status (including catatonic signs), and evidence of autonomic instability (irregular
pulse or blood pressure). Additional signs may include elevated CPK, myoglobinuria (rhabdomyolysis), and acute renal failure. Hyperthermia is often an early sign of this syndrome. NMS is potentially fatal, requires intensive symptomatic treatment and immediate discontinuation of neuroleptic treatment.
Dantrolene and bromocriptine have been used for the treatment of NMS.
Signs of autonomic dysfunction such as tachycardia, labile arterial pressure and sweating may precede the onset of hyperthermia thereby acting as early warning signs. Antipsychotic treatment should be withdrawn immediately and appropriate supportive therapy and careful monitoring instituted.
Hyperpyrexia and heat stroke not associated with the above symptom complex have also been reported with HALDOL Decanoate.
Extrapyramidal Symptoms
Extrapyramidal reactions such as Parkinson-like symptoms, akathisia or dystonic reactions occur frequently with neuroleptics including oral and injectable haloperidol. These have been observed with HALDOL Decanoate. In most patients, Parkinson-like symptoms, when first observed, were usually mild to moderately severe and usually reversible. They are more commonly observed during the first few days of treatment, however Parkinson rigidity, tremor and akathisia tend to appear less rapidly. They sometimes remit spontaneously as treatment continues, or can be relieved by the use of anti-Parkinson medication or a reduction in dose. Antiparkinson drugs of the anticholinergic type should only be used when required because of their potential to impair the efficacy of HALDOL Decanoate. If concomitant antiparkinson medication is required, it may have to be continued after stopping HALDOL Decanoate if its excretion is faster than that of HALDOL Decanoate in order to avoid the development or aggravation of extrapyramidal symptoms. The physician should keep in mind the possible increase in intraocular pressure when anticholinergic drugs, including antiparkinson agents, are administered.
Other types of neuromuscular reactions (motor restlessness, dystonia, akathisia, hyperreflexia, opisthotonos, oculogyric crisis) have been reported far less frequently, but were often more severe.
Akathisia is best managed by a reduction in dosage in conjunction with the temporary use of an oral antiparkinson drug. Dystonias, which can lead to laryngeal spasm or bronchospasm, may be controlled by amylobarbitone or injectable antiparkinson agents. Extrapyramidal reactions appear to be dose-related.
Tardive Dyskinesia
Tardive dyskinesia, a syndrome consisting of potentially irreversible involuntary, dyskinetic movements, is known to occur in patients treated with neuroleptics with antipsychotic properties and other drugs with substantial neuroleptic activity. The syndrome is characterised by rhythmical involuntary movements of the tongue, face, mouth or jaw (e.g., protrusion of tongue, puffing of cheeks, puckering of mouth, chewing movements). Sometimes these may be accompanied by involuntary movements of the extremities. Tardive dyskinesia may appear in some patients on long-term therapy or may appear after drug therapy has been discontinued. The symptoms are persistent and although the dyskinetic syndrome may remit partially or completely if the medication is withdrawn, it is irreversible in some patients.
The prevalence of the syndrome appears to be highest among the elderly, especially elderly women. At the present time there is uncertainty as to whether neuroleptic drugs differ in their potential to cause tardive dyskinesia. There is no known effective treatment for tardive dyskinesia; antiparkinsonian agents usually do not alleviate the symptoms of this syndrome. Since there is a significant prevalence of this syndrome associated with the use of neuroleptic drugs, and there is no known effective treatment, chronic use of these drugs should generally be restricted to patients for whom there is no alternative therapy available with better risk acceptability. If manifestations of tardive dyskinesia are detected during the use of a neuroleptic, the drug should be discontinued. It is suggested that the dosage of all antipsychotic agents be progressively reduced with a view to discontinuation if possible. Should it be necessary to reinstitute treatment or increase the dosage of the agent, or switch to a different antipsychotic agent, the syndrome may be masked. It has been reported that fine vermicular movements of the tongue may be an early sign of the syndrome, and, if the medication is stopped at that time, the full syndrome may not develop.
The risk of a patient developing tardive dyskinesia and of the syndrome becoming irreversible appear to increase with the duration of treatment and the total amount of drugs administered, although, in some instances, tardive dyskinesia may develop after relatively short periods of treatment at low doses. The risk of developing tardive dyskinesia may, therefore, be minimised by reducing the dose of the neuroleptic drug
used and its duration of administration, consistent with the effective management of the patient's condition. Continued use of neuroleptics should be periodically reassessed.
Tardive Dystonia
Tardive dystonia, which might be observed in the absence of other symptoms of the above syndrome, has also been reported. Tardive dystonia is characterized by delayed onset of choreic or dystonic movements, is often persistent, and has the potential of becoming irreversible.
Seizures/ Convulsions Seizures can be triggered by haloperidol. If indicated, adequate anticonvulsant therapy should be concomitantly maintained. Caution is advised in patients suffering from epilepsy and in conditions predisposing to convulsions (e.g. alcohol withdrawal and brain damage). Hepatobiliary concerns Since haloperidol is metabolised in the liver, careful observation of patients with liver disease is recommended. Impaired liver function and/or jaundice or hepatitis, most often cholestatic, has been reported. Endocrine System Concerns
Patients with thyrotoxicosis. Antipsychotic medication, including HALDOL Decanoate, may result in severe neurotoxicity (rigidity, inability to walk or talk). Antipsychotic treatment in these patients should always be accompanied by appropriate monitoring and therapy.
*Venous thromboembolism Cases of venous thromboembolism (VTE) have been reported with antipsychotic drugs. Since patients treated with antipsychotics often present with acquired risk factors for VTE, all possible risk factors for VTE should be identified before and during treatment with HALDOL Decanoate and preventive measures undertaken.
Weight Gain
Clinically significant weight gain has been reported in patients taking HALDOL DECANOATE. Patients taking antipsychotic medications, including HALDOL Decanoate should undergo regular monitoring of weight and the testing of other parameters (e.g., blood glucose, haemoglobin A1C) that would be appropriate in the setting of significant weight gain. Clinicians should individualize treatment decisions based on such monitoring.
Additional Considerations
It is recommended that patients to be treated with HALDOL Decanoate be treated initially with oral haloperidol to exclude the possibility of severe unexpected sensitivity to haloperidol.
HALDOL Decanoate should be administered with caution to:
• Patients with severe cardiovascular disorders, because of the possibility of transient hypotension
and/or precipitation of anginal pain. When antihypertensives and haloperidol are used concomitantly the use of vasopressors such as noradrenaline may be indicated if the resulting hypotension is prolonged and severe. Adrenaline should not be used since haloperidol may reverse its action and cause profound hypotension.
• Patients receiving anticonvulsant medications with a history of seizures, or with EEG abnormalities,
because haloperidol may lower the convulsive threshold (see PRECAUTIONS – Seizures/ Convulsions).
• Patients who are elderly or debilitated. These patients should be observed for evidence of
over-sedation, which, unless alleviated, could result in complications such as terminal stasis pneumonia.
• Patients with thyrotoxicosis (see PRECAUTIONS – Endocrine System Concerns). • Patients with known allergies or with a history of allergic reactions to drugs. • Patients receiving anticoagulants (see Interactions With Other Drugs).
When HALDOL Decanoate is used to control mania in bipolar disorders, there may be a rapid mood swing to depression.
Antiemetic action may obscure the diagnosis of an underlying condition characterised by nausea and vomiting.
It is advisable to carefully observe the patients who receive haloperidol decanoate for a long period in order to identify any changes in the skin or eyes. Oculocutaneous changes have been observed following use of butyrophenones structurally related to haloperidol.
If concomitant antiparkinson medication is required, it may have to be continued after HALDOL Decanoate is discontinued because of the prolonged action of haloperidol decanoate. If both drugs are discontinued simultaneously, extrapyramidal symptoms may occur.
Effects on Fertility
There are no human data on the effects of haloperidol on male and female fertility. In female rats, administration of haloperidol induced oestrus cycle disruptions, and in female mice, subcutaneous administration of haloperidol prior to ovulation induced delays in implantation, cleavages and blastocoele formation. In male rats, oral administration of haloperidol prior to mating reduced fertility, increased preimplantation loss and induced histopathological changes in the reproductive organs. Following intraperitoneal administration of haloperidol to female rats from early pregnancy to weaning, the frequency of ejaculation in offspring was reduced. These studies used various dose levels and in some cases a no-effect level was not established. The significance of these findings for human exposure to therapeutic doses of haloperidol decanoate is unknown.
Carcinogenicity
There was no evidence of carcinogenicity in Wistar rats following oral administration of haloperidol for 24 months at doses up to 5mg/kg/day. In female mice, there was an increase in mammary gland neoplasia and total tumour incidence following oral administration of haloperidol at doses of 1.25 and 5mg/kg/day and an increase in pituitary gland neoplasia at 5mg/kg/day. There were no carcinogenic effects in male mice. Haloperidol increases prolactin levels, which may affect human breast cancers, one-third of which are prolactin dependent in vitro. Although clinical studies have not shown an association between chronic treatment with antipsychotic drugs (including haloperidol) and an increase in breast cancer incidence, it may be a factor of importance when prescribing haloperidol for patients with a history of breast cancer.
In four alternative short-term carcinogenicity models using neonatal or transgenic mice, there was no evidence of carcinogenicity at systemic exposures (plasma AUC) from one to eleven times the clinical exposure, at the maximal recommended human intramuscular dose of haloperidol decanoate.
Genotoxicity
Haloperidol and haloperidol decanoate were negative in bacterial gene mutation assays, and haloperidol was also negative in a mammalian forward mutation assay and in assays for chromosomal damage in human lymphocytes in vitro and in vivo and in rat bone marrow in vivo.Use in Pregnancy (Category C)
There have been isolated case reports of birth defects following foetal exposure to haloperidol in combination with other drugs.
*Non-teratogenic class effect: Neonates exposed to antipsychotic drugs (including HALDOL) during the third trimester of pregnancy are at risk of experiencing extrapyramidal neurological disturbances and/or withdrawal symptoms following delivery. There have been post-market reports of agitation, hypertonia, hypotonia, tremor, somnolence, respiratory distress, and feeling disorder in these neonates. These complications have varied in severity; while in some cases symptoms have been self-limited; in other cases neonates have required additional medical treatment or monitoring. HALDOL should be used during pregnancy only if the anticipated benefit outweighs the risk and the administered dose and duration of treatment should be as low and as short as possible.
Withdrawal-emergent syndromes in neonates, following long-term, in utero exposure to haloperidol, have been reported.
In pregnant rodents, administration of haloperidol during the period of organogenesis has produced adverse effects including embryolethality, gross malformations (cleft palate, neural tube defects), and reduced brain and body weight and behavioural effects in offspring. The significance of these findings for human exposure to therapeutic doses of haloperidol decanoate is unknown.
Use In Lactation
Since haloperidol is excreted in human breast milk, infants should not be nursed during treatment with HALDOL Decanoate. Extrapyramidal symptoms have been observed in breast-fed infants of women treated with HALDOL Decanoate.
Use In Children
Safety and efficacy in children have not been established; therefore HALDOL Decanoate is not recommended for use in the paediatric age group.
Effects on Ability to Drive or Operate Machinery
HALDOL Decanoate may impair the mental and/or physical abilities required for the performance of hazardous tasks such as operating machinery or driving a motor vehicle. The ambulatory patient should be warned accordingly.
Interactions With Other Medicines
As with other antipsychotics, caution is advised when prescribing with medications known to prolong the QT interval.
Haloperidol is metabolised by several routes, including glucuronidation and the cytochrome P450 enzyme system (particularly CYP 3A4 or CYP 2D6). Inhibition of these routes of metabolism by another drug or a decrease in CYP 2D6 enzyme activity may result in increased haloperidol concentrations and an increased risk of of adverse events, including QT-prolongation. In pharmacokinetic studies, mild to moderately increased haloperidol concentrations have been reported when haloperidol was given concomitantly with drugs characterised as substrates or inhibitors of CYP 3A4 or CYP 2D6 isozymes, such as itraconazole, nefazodone, buspirone, venlafaxine, alprazolam, fluvoxamine, quinidine, fluoxetine, sertraline, chlorpromazine and promethazine. A decrease in CYP2D6 enzyme activity may result in increased haloperidol concentrations. Increases in QTc have been observed when haloperidol was given with a combination of the metabolic inhibitors ketoconazole (400mg/day) and paroxetine (20mg/day). It may be necessary to reduce the haloperidol dosage.
Caution is advised when used in combination with drugs known to cause electrolyte imbalance.
Effect of Other Medicines on HALDOL Decanoate
When prolonged treatment with enzyme inducing drugs such as carbamazepine, phenobarbitaI and rifampicin is added to HALDOL Decanoate therapy, a significant fall in haloperidol plasma levels occurs. Therefore, during therapy with this combination, the HALDOL Decanoate dosage may need to be increased. Conversely, after stopping therapy with such drugs it may be necessary to reduce the dosage of HALDOL Decanoate.
Sodium valproate, a drug known to inhibit glucuronidation, does not affect haloperidol plasma concentrations.
Effects of HALDOL Decanoate on Other Medicines
Although HALDOL Decanoate does not provoke a respiratory depression, it can have a potentiating effect on CNS depressants such as anaesthetics, opiates, hypnotics (barbiturates) and alcohol.
An enhanced CNS effect (disorientation, memory loss, mental retardation, aggression, irritability) when combined with methyldopa has been reported.
HALDOL Decanoate may antagonise the action of adrenaline and other sympathomimetic agents and reverse the blood pressure lowering effects of adrenergic blocking agents such as guanethidine.
HALDOL Decanoate may impair the antiparkinsonian effects of levodopa.
Haloperidol is an inhibitor of CYP 2D6. HALDOL Decanoate inhibits the metabolism of tricyclic antidepressants, increasing blood levels of these drugs. This may result in increased tricyclic antidepressant toxicity.
Other Forms of Interaction
An encephalopathic syndrome characterised by weakness, lethargy, fever, tremulousness and confusion, extrapyramidal symptoms, leukocytosis, elevated serum enzymes and BUN and followed by irreversible brain damage has occurred in a few patients treated with lithium plus haloperidol; a causal relationship has not been established. However patients receiving such combined therapy should be monitored closely for early evidence of neurological toxicity and treatment discontinued should such signs appear.
Haloperidol has been reported to interfere with the activity of phenindione and coumarin anticoagulants.
The use of alcohol with this drug should be avoided due to possible additive effects and hypotension.
ADVERSE EFFECTS Clinical Trial Data Comparator and Open-Label Trial Data – Adverse Drug Reactions Reported at ≥1% Incidence
The safety of HALDOL Decanoate (15-500 mg/month) was evaluated in 410 subjects who participated in
13 clinical trials in the treatment of schizophrenia or a schizoaffective disorder.
Adverse Drug Reactions (ADRs) reported by ≥1% of HALDOL DECANOATE-treated subjects in these
trials are shown in Table 1. Table 1. Adverse Drug Reactions Reported by ≥1% of HALDOL DECANOATE-
treated Subjects in Comparator and Open-Label Clinical Trials of HALDOL
System/Organ Class Haloperidol decanoate Nervous System Disorders
Tremor 8.0 Parkinsonism 7.3 Somnolence 4.9 Masked facies
Gastrointestinal Disorders
Constipation 2.0 Salivary hypersecretion
Musculoskeletal and Connective Tissue Disorders Reproductive System and Breast Disorders General Disorders and Administration Site Conditions Investigations Comparator and Open-Label Trial Data – Adverse Drug Reactions Reported at <1% Incidence
Additional ADRs that occurred in <1% of HALDOL DECANOATE-treated subjects either of the above
trial data are listed below in Table 2. Table 2. Adverse Drug Reactions Reported by <1 % of HALDOL DECANOATE-
treated Subjects in Comparator and Open-Label Clinical Trials of HALDOL
Nervous System Disorders
Akinesia Dyskinesia Hypertonia Dystonia Cogwheel rigidity
Eye disorders
Vision blurred Visual disturbance Oculogyric Crisis
Cardiac Disorders
The following is a list of additional ADRs that have been identified in clinical trials with other formulations
Endocrine Disorders Psychiatric Disorders
Libido decreased Loss of libido Restlessness
Nervous System Disorders
Bradykinesia Dizziness Hyperkinesia Hypokinesia Motor dysfunction Muscle contractions involuntary Neuroleptic malignant syndrome Nystagmus Tardive dyskinesia
Vascular Disorders Musculoskeletal and Connective Tissue Disorder
Muscle spasms Musculoskeletal stiffness Muscle twitching Trismus Torticollis
Reproductive System and Breast Disorder
Amenorrhoea Breast discomfort Breast pain Dysmenorrhoea Erectile dysfunction Galactorrhoea Menstrual disorder Menorrhagia
General Disorders and Administration Site Postmarketing Data
Adverse events first identified as ADRs during postmarketing experience with haloperidol, presented by
frequency category based on spontaneous reporting rates, are included in Table 3. The postmarketing
review was based on review of all cases including haloperidol and haloperidol decanoate products. In
each table, the frequencies are provided according to the following convention:
Very common ≥1/10 Common ≥1/100 to <1/10 Uncommon ≥1/1,000 to <1/100 Rare ≥1/10,000 to <1/1,000 Very rare <1/10,000, including isolated reports
Table 3: Adverse Drug Reactions Identified During Postmarketing Experience with Haloperidol (oral, solution, or decanoate) by Frequency Category Estimated From Spontaneous Reporting Rates Blood and Lymphatic System Disorders Very rare
Agranulocytosis, Pancytopenia, Thrombocytopenia, Leukopenia, Neutropenia
Immune System Disorders Very rare Endocrine Disorders Very rare
Inappropriate antidiuretic hormone secretion (presenting with hyponatraemia)
Metabolic and Nutritional Disorders Very rare Psychiatric Disorders Very rare
Psychotic disorder, Agitation, Confusional state, Depression, Insomnia
Nervous System Disorders Very rare
Cardiac Disorders Very rare
Torsade de pointes, Ventricular fibrillation, Ventricular tachycardia, Extrasystoles
Respiratory, Thoracic and Mediastinal Disorders Very rare
Bronchospasm, Laryngospasm, Laryngeal oedema, Dyspnoea
Gastrointestinal Disorders Very rare Hepatobiliary Disorders Very rare
Acute hepatic failure, Hepatitis, Cholestasis, Jaundice, Liver function test abnormal
Skin and Subcutaneous Tissue Disorders Very rare
Leukocytoclastic vasculitis, Dermatitis exfoliative, Urticaria, Photosensitivity reaction, Rash, Pruritis, Hyperhidrosis
Renal and Urinary Disorders Very rare
Pregnancy, Puerperium and Perinatal Conditions Very rare
Reproductive System and Breast Disorders Very rare
General Disorders and Administration Site Conditions Very rare
Sudden death, Face oedema, Oedema, Hypothermia, Hyperthermia, Injection site abscess
Investigations Very rare
Electrocardiogram QT prolonged, Weight decreased
DOSAGE AND ADMINISTRATION
HALDOL Decanoate should be administered by deep intramuscular injection into the gluteal region. A 2-inch long, 21-gauge needle is recommended. The maximum volume per injection site should not exceed 3 mL. The recommended interval between doses is 4 weeks.
DO NOT ADMINISTER INTRAVENOUSLY
HALDOL Decanoate is intended for use in chronic psychotic patients who require prolonged parenteral antipsychotic therapy. These patients should be previously stabilised on antipsychotic medication before considering a conversion to HALDOL Decanoate. Furthermore, it is recommended that patients being considered for HALDOL Decanoate therapy be initially converted to oral haloperidol to exclude the possibility of an unexpected adverse sensitivity to haloperidol.
The starting dose of HALDOL Decanoate should be based on the patient's clinical history, physical condition and response to previous antipsychotic therapy. It is recommended that the initial dose of HALDOL Decanoate be 10-15 times the previous daily dose in oral haloperidol equivalents, but no more than a maximum initial dose of 100 mg (2 mL). The preferred approach to determining the minimum effective dose is to begin with lower initial doses and to adjust the dose upward as needed. Close clinical supervision is required during the initial period of dose adjustment in order to minimise the risk of over-dosage or reappearance of psychotic symptoms before the next injection. During dose adjustment or episodes of exacerbation of psychotic symptoms, HALDOL Decanoate therapy can be supplemented with short-acting forms of haloperidol.
Haloperidol decanoate has been effectively administered at monthly intervals - however variation in patient response may dictate a need for adjustment of the dosing interval as well as the dose.
Lower initial doses and more gradual adjustments are recommended for elderly or debilitated patients.
Clinical experience with HALDOL Decanoate at doses greater than 300 mg (6 mL) per month has been limited.
OVERDOSAGE
While over dosage is less likely to occur with parenteral than with oral medication, information pertaining to oral haloperidol is presented, modified only to reflect the extended duration of action of haloperidol decanoate.
Manifestations
In general, the symptoms of over dosage would be an exaggeration of known pharmacological effects and adverse reactions, the most prominent of which would be severe extrapyramidal reactions, hypotension or sedation.
The patient would appear comatose with respiratory depression and hypotension that could be severe enough to produce a shock-like state. The extrapyramidal reaction would be manifest by muscular weakness or rigidity and generalised or localised tremor, as demonstrated by akinetic or agitans types respectively. With accidental over dosage, hypertension rather than hypotension occurred in a two-year-old child.
There is a possibility of ventricular arrhythmias, sometimes associated with QT prolongation.
Treatment
Since there is no specific antidote, treatment is primarily supportive. A patent airway must be established by use of an oropharyngeal airway or endotracheal tube or, in prolonged cases of coma, by tracheostomy. Respiratory depression may be counteracted by artificial respiration and mechanical respirators.
Hypotension and circulatory collapse may be counteracted by use of intravenous fluids, plasma, or concentrated albumin, and vasopressor agents such as noradrenaline. Adrenaline should not be used. In case of severe extrapyramidal reactions antiparkinson medication should be administered, continued for several weeks then withdrawn very cautiously as extrapyramidal symptoms may emerge.
ECG and vital signs should be monitored until the ECG is normal. Severe arrhythmias should be treated with appropriate anti-arrhythmic measures.
PRESENTATION AND STORAGE CONDITIONS Presentation
HALDOL Decanoate Injection haloperidol decanoate 70.52 mg/mL (equivalent to 50 mg haloperidol) oily injection for IM use only, 1 mL or 3 mL in packs of 5 ampoules.
Store below 25 C. Protect from light. Do not freeze or refrigerate.
NAME AND ADDRESS OF THE SPONSOR
JANSSEN-CILAG Pty Ltd 1-5 Khartoum Road Macquarie Park NSW 2113 Australia NZ Office: Auckland New Zealand
POISON SCHEDULE OF THE MEDICINE
S4 – Prescription Medicine Date of first inclusion on the ARTG: 28th August 1991 Date of most recent amendment: 24th November 2011
* Please note changes (presented as *italicised text) in Product Information.
Prof. Dr. med. Maximilian Spraul Chefarzt der Medizinischen Klinik III Interdisziplinäres Diabetes-Fuß-Zentrum, Mathias-Spital und Jakobi-Krankenhaus, Rheine Mathias Spital Frankenburgstraße 31 48431 Rheine [email protected] Tel.: +49 (59 71) 46411 Fax: +49 (59 71) 4 23 16 95 Beruflicher Werdegang 1977 - Studium der Betriebswirtschaftslehre an der Universität Mannhei
Notizie salutari (a cura di Rosa Maria Chicco) ottobre 2003 - Il Sidney Morning Herald" (uno dei piu' importanti quotidiani australiani) del 23.10.2003, in un articolo dal titolo “Una tecnica di controllo dell'asma in alternativa al Ventolin", riferisce su una nuova sperimentazione avviata in Australia dal Co-operative Research Centre for Asthma, per accertare se sia possibile ottenere r

 HALDOL®
HALDOL®