Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Pone.0008945 1.6
Antiviral Prescriptions to U.S. Ambulatory Care Visitswith a Diagnosis of Influenza before and after High Levelof Adamantane Resistance 2005–06 Season
Yu-Hsiang Hsieh1*, Kuan-Fu Chen1,3, Charlotte A. Gaydos2, Richard E. Rothman1,2, Gabor D. Kelen1
1 Department of Emergency Medicine, Johns Hopkins University School of Medicine, Baltimore, Maryland, United States of America, 2 Department of Medicine, Johns
Hopkins University School of Medicine, Baltimore, Maryland, United States of America, 3 Department of Emergency Medicine, Chang Gung Memorial Hospital, Taipei,
Background: Rapid emergence of influenza A viruses resistance to anti-influenza drugs has been observed in the past fiveyears. Our objective was to compare antiviral prescription patterns of ambulatory care providers to patients with a diagnosisof influenza before and after the 2005–2006 influenza season, which was temporally concordant with the emergence ofadamantane resistance. We also determined providers’ adherence to Centers for Disease Control and Prevention (CDC) 2006interim treatment guidelines for influenza after the dissemination of guidelines.
Methodology/Principal Findings: We conducted a multi-year cross-sectional analysis using 2002–2006 data from thenational representative ambulatory care surveys, National Ambulatory Medical Care Survey and National HospitalAmbulatory Medical Care Survey. Our main outcome measure was prescription of any anti-influenza pharmaceuticalmedication, including amantadine, rimantadine, oseltamivir, and zanamivir. Analyses were performed using procedurestaking into account the multi-stage survey design and weighted sampling probabilities of the data source. Overall, therewere 941 visits to U.S. ambulatory care providers for which the diagnosis of influenza was made, representing 12,140,727visits nationally. Antiviral drugs were prescribed in 21.7% of visits. Even though prescription rates were not significantlydifferent by influenza season (2001–02: 26.4%; 2002–03: 11.2%; 2003–04: 16.5%; 2004–05: 18.0%; 2005–06: 35.8%; 2006–07:46.5%, p = 0.061), significantly higher prescription rates were observed in the high adamantane resistance period (18.7%versus 37.0%, p = 0.023), and after the announcement of the 2006 guidelines (18.5% versus 38.8%, p = 0.032). Use ofadamantanes decreased over time, in that they were commonly used during influenza seasons 2001–03 (60.1%), but usedmuch less frequently during seasons 2003–05 (31.9%), and used rarely after high adamantane resistance emerged (2.2%)(p,0.001). Adherence to 2006 guidelines was 97.7%. After March 2006, no prescriptions for adamantanes were given topatients with a diagnosis of influenza.
Conclusions/Significance: In this nationally representative study of U.S. ambulatory care visits, we found a completeabsence of the use of adamantanes in all ambulatory care settings after March 2006, closely corresponding to release of the2006 CDC interim guidelines. Adherence to such practice is an essential element for control and prevention of influenza,especially during the era of emergence of resistance to anti-viral drugs.
Citation: Hsieh Y-H, Chen K-F, Gaydos CA, Rothman RE, Kelen GD (2010) Antiviral Prescriptions to U.S. Ambulatory Care Visits with a Diagnosis of Influenza beforeand after High Level of Adamantane Resistance 2005–06 Season. PLoS ONE 5(1): e8945. doi:10.1371/journal.pone.0008945
Editor: Joseph S. Ross, Mount Sinai School of Medicine, United States of America
Received November 1, 2009; Accepted January 12, 2010; Published January 28, 2010
Copyright: ß 2010 Hsieh et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: Dr. Hsieh, Dr. Gaydos, Dr. Rothman and Dr. Kelen are supported in part by a grant from the United States Department of Homeland Security (GrantNumber N00014-D6-1-0991). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing Interests: The authors have declared that no competing interests exist.
influenza drugs, the adamantanes (amantadine and rimantadine)emerged in the United States, with resistance rates increasing from
Each year, Americans make more than 20 million clinic visits
14.5% during the 2004–2005 influenza season, to 92.3% during
per year for influenza. Of these, only 19% of visits receive antiviral
the 2005–2006 season [3]. In response, the US Centers for Disease
prescription from their medical providers [1]. This low rate of
Control and Prevention (CDC) recommended that adamantanes
antiviral treatment observed in practice may hamper public health
should not be used for treatment or prophylaxis of influenza on
efforts to minimize mortality, shorten the course of disease, and
January 14, 2006 in the interim treatment guidelines [4]. Since
decrease transmission in the communities for the current novel
that time, after only 3 influenza seasons, rates of oseltamivir-
influenza A (H1N1) [2] or future pandemics.
resistant to seasonal influenza A virus (H1N1) stains have risen
Rapid emergence of influenza A viruses resistance to anti-
from 12% to nearly 99% [5]. Accordingly, the CDC now
influenza drugs has been observed in the past five years. First,
recommends that when influenza A (H1N1) virus infection or
resistance of seasonal influenza A viruses to once first-line anti-
exposure is suspected, zanamivir or a combination of oseltamivir
January 2010 | Volume 5 | Issue 1 | e8945
and rimantadine are more appropriate options than oseltamivir
codes of 487, 487.0, 487.1 or 487.8. All visits with a diagnosis of
alone [6]. Only a few months later in the early summer of 2009,
influenza during the study period were included for analysis. Six
the first influenza pandemic in more than 40 years has arrived [2].
(in 2002) or eight (2003–2006) medications that were ordered or
The CDC recommends use of oseltamivir or zanamivir for the first
provided were collected and coded in the data set. Our main
line treatment and/or prevention of infections since the circulating
outcome measure was prescription of any anti-influenza pharma-
strain is resistant to the adamantanes [7]. Few cases of oseltamivir-
ceutical medication, including amantadine, rimantadine, oselta-
resistance strains of novel influenza A (H1N1) have been
mivir, and zanamivir. A visit with a prescription of anti-influenza
drug by providers was defined as medications matching for
Timely and effective dissemination of these interim treatment
NAMCS and NHAMCS drug entry codes for amantadine
guidelines for influenza from CDC to medical providers is crucial
(Symmetrel), rimantadine (Flumadine), oseltamivir (Tamiflu), and
to prescribe appropriate antivirals for patients with confirmed or
suspected influenza. In the past decade, CDC has disseminated
NAMCS and NHAMCS data from the years 2002–2006 were
treatment information (which could be a CDC Health Advisory,
merged for data analysis. A sample weight that considers selection
Health Alert, or Health Update) via CDC Health Alert Network
probability, nonresponse adjustment, and ratio adjustment for
(HAN) to state and local health officers, public information
different total sample size each year is assigned for each patient
officers, epidemiologists, state laboratory directors, weapons of
visit to generate unbiased national estimates of ambulatory
mass destruction coordinators, HAN coordinators, as well as
medical care visits. Although the sampling fraction is relatively
public health associations and clinician organizations [9]. Few, if
small, the weighted numbers calculated by the method suggested
any studies, have examined U.S. medical providers’ antiviral drug
by the CDC represent unbiased national estimates of the US
prescription usage patterns and trends for patients with a diagnosis
ambulatory medical care population. Study period was catego-
of influenza, before and after the emergence of drug resistance.
rized into 6 influenza seasons beginning October 1 to the end of
Notably, studies have been conducted evaluating provider
September of the following year. In addition, study periods were
adherence with CDC treatment guidelines for other infectious
further categorized into (1) pre-high adamantane resistance period
diseases, with rates varying significantly across syndromes, i.e. 30%
versus high adamantane resistance period, based on the time when
for pelvic inflammatory disease [10] and upper respiratory
adamantane resistance rates reached over 90% [3], i.e. October
infections [11], 50%–85% for acute epididymitis [12], and over
2005, or (2) before versus after the announcement of the 2006
interim treatment guidelines, based on the time of release of the
Utilizing the national representative ambulatory medical care
2006 CDC interim treatment guidelines [4], i.e. January 14, 2006.
surveys National Ambulatory Medical Care Survey (NAMCS) and
Adherence to the 2006 CDC interim treatment guidelines was
defined as no adamantane prescribed to patients with a diagnosis
(NHAMCS) [14] by National Center for Health Statistics, CDC,
of influenza, following the announcement of the treatment
we compared antiviral prescription patterns of ambulatory
medical care providers for patient visits with a diagnosis of
Descriptive demographic analyses of patient visits with a
influenza before and after the 2005–2006 influenza season, which
diagnosis of influenza, and patient visits with antiviral medications
was temporally concordant with the emergence of adamantane
for influenza, were performed. Comparison of proportions, e.g.
resistance. We also determined medical provider’s adherence to
prescription rate in pre-high adamantane resistance period versus
CDC 2006 interim treatment guidelines for influenza after the
that in high adamantane resistance period, was assessed by chi-
dissemination of the CDC guidelines.
square test. All p values were 2-sided, with p,0.05 consideredsignificant. Multivariate analyses and estimation of 95% CI were
not conducted if the sample size of interest was less than 30, as theestimate is considered unreliable under NAMCS and NHAMCS
We conducted a multi-year cross-sectional analysis using 2002–
analysis recommendations [17]. Analyses were performed using
2006 data from three national representative ambulatory medical
SAS 9.1 SURVEYFREQ procedure which takes into account the
care surveys. The data from these three surveys include weighted
multi-stage survey design and weighted sampling probabilities of
samples of U.S. patient visits to non-federally employed office-
the data source (SAS version 9.1, SAS Institute Inc., Cary, North
based physicians from the NAMCS, U.S. emergency department
Carolina). Results were reported as weighted frequencies,
(ED) visits from the ED component of the NHAMCS, and U.S.
percentages, and 95% confidence intervals (CI).
hospital outpatient visits, from the outpatient component ofNHAMCS. NAMCS and NHAMCS data were collected by a
standard survey form collected by physicians, office workers, orhospital staff. The multi-stage probability sampling scheme, the
Overall, during 2002–2006, there were 941 visits to U.S.
visit, and the reliability of coding and data entry for NAMCS and
ambulatory care providers for which the diagnosis of influenza was
NHAMCS have been detailed elsewhere [15]. The NAMCS and
NHAMCS data are publicly accessible and deidentified. Accord-
10,116,136–14,165,318) patient visits nationally, or 0.22% (95%
ingly, the Johns Hopkins University Medicine institutional review
CI: 0.18–0.25) of all visits over this time. Demographics, type of
board (IRB) deemed our study as nonhuman-subjects research,
ambulatory care, and influenza season in which patient visits
resulted in a diagnosis of influenza were summarized in Table 1.
In this study, we employed the data collected by the NAMCS
Office-based physician visits represented the highest volume
and NHAMCS, including demographic characteristics, diagnoses,
(9,459,918 visits, 77.9%), followed by ED visits (1,872,200 visits,
and medications of the patient visits. Up to three diagnoses were
15.4%) and outpatient visits (808,609 visits, 6.7%). Among visits
recorded as free text and coded centrally by Constella Group, Inc.
with a diagnosis of influenza, those which occurred during periods
and subject to quality control procedures [16]. A visit with a
of high adamantane resistance, and after the announcement of
diagnosis of influenza was defined as International Classification of
2006 CDC interim treatment guidelines accounted for 18.7% and
Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)
January 2010 | Volume 5 | Issue 1 | e8945
Table 1. National estimates of ambulatory medical care visits with a diagnosis of influenza and the antiviral prescription bydemographics in the United States, 2002–2006.
*Ethnicity missing for 4.7% of sample. {MSA: Metropolitan Statistical Area. {NA: Not applicable due to the sample size of interest in the surveys was less than 30, as the estimate is considered unreliable under NAMCS and NHAMCS analysis
Antiviral drugs against influenza were prescribed in 21.7%
differences in prescription rates by demographic variables
of visits (weighted 2,629,129 visits; 95% CI: 1,886,292–3,
except by the U.S. region. Even though, prescription rates
371,966). Prescription rates by each demographic character-
were not significantly different by influenza season, signifi-
istic and type of ambulatory care were summarized in Table 1.
cantly higher antiviral drug prescription rates were observed in
Although EDs had the highest prescription rate, (29.0%), there
the high adamantane resistance period, and after the
was no statistical difference observed by type of ambulatory
announcement of the 2006 CDC interim treatment guidelines
care setting (p.0.05). In addition, there were no statistical
January 2010 | Volume 5 | Issue 1 | e8945
Table 2. National estimates of ambulatory medical care visits with a diagnosis of influenza and the antiviral prescription byinfluenza season, high adamantane resistance period, and announcement of 2006 CDC guidelines in the United States, 2002–2006.
*NA: Not applicable due to the sample size of interest in the surveys was less than 30, as the estimate is considered unreliable under NAMCS and NHAMCS analysis
Numbers of antiviral prescriptions for influenza in U.S.
increased over time, becoming the predominant anti-influenza
ambulatory care visits resulting in a diagnosis of influenza were
prescription in all three ambulatory care settings during the high
summarized in Table 3. Use of adamantanes decreased over time,
adamantane resistance period, i.e. after October 2005 (97.8%;
in that they were commonly used during influenza seasons 2001–
95% CI: 93.9–100%). There were no statistical differences in anti-
02 and 2002–03 (60.1%), but were used much less frequently
influenza prescriptions by type of ambulatory care or by other
during seasons 2003–04 and 2004–05 (31.9%), and were used
demographic variables, before or during high adamantane
rarely after high adamantane resistance emerged (2.2%) (p,0.001)
resistance period (data not shown). Therefore, a multivariate
(Figure 1). In contrast, oseltamivir accounted for only 36% of total
analysis was not performed on use of adamantanes or oseltamivir
antiviral prescription during the influenza season 2001–02, but
Table 3. Numbers of antiviral prescription for influenza in U.S. ambulatory care visits with a diagnosis of influenza during 2002–2006.
*Zanamivir was prescribed, therefore, percentages of prescription in these horizontal rows were not added up to 100%. {P-value cannot be computed for all influenza seasons because at least one table cell has 0 frequency (season 2006–07). P-value was calculated based on the
comparison of influenza season 2001–02 to season 2005–06.
January 2010 | Volume 5 | Issue 1 | e8945
Figure 1. Prescription of anti-influenza agents for patient visits with a diagnosis of influenza in US ambulatory care includingemergency department visits, outpatient visits and physician office visits, by antiviral drug, influenza season 2001–2007. a The timeCDC declared interim guidelines for use of anti-influenza drugs. b The start of high adamantane resistance period. c Adamantanes include amantadineand rimantadine. doi:10.1371/journal.pone.0008945.g001
Overall, adherence with the 2006 CDC interim treatment
intensity of media reporting, and the ease of implementation.
guidelines was 97.7% (95% CI: 93.0%–100%). After March 2006,
Together these factors could contribute to the significant
no prescriptions for adamantanes were given to ambulatory-care
differences between the nearly perfect provider adherence
patients with a diagnosis of influenza (last prescription in the
observed for CDC treatment guidelines for influenza, versus that
dataset: office-based physician visit: February 2005; ED visit:
seen for PID, upper respiratory infections, and acute epididymitis
February 2006; outpatient visit: March 2006).
[10,11,12]. One infectious disease in which clinician adherencewith CDC guidelines is also high is genital chlamydial infection,
where, effective dissemination of updates, implementation ofelectronic order-entry systems, and national continuing medical
In this nationally representative study, we found that the use of
education efforts have been reported to increase rates of
adamantanes markedly decreased after the influenza 2002–2003
compliance in at least 2 large managed care organizations [13].
season, and were rapidly replaced by oseltamivir as the
Since patients with suspected influenza visit a variety of
predominantly prescribed anti-influenza drug therapy in U.S.
ambulatory care settings in the U.S., timely and concentrated
non-federally employed office-based physician, ED, and outpatient
electronic communication messages and interaction between the
visits. The major shift occurred during the early influenza 2005–
CDC and each medical society and institution, as well as effective
2006 season, paralleling the rapid emergence of adamantane
dissemination from the society or institution to its own members is
resistance of influenza A viruses seen in both Asia [18] and the
likely critical for ensuring adherence with the most up to date
U.S. [3]. We also identified a complete absence of adamantane
treatment guidelines during a pandemic. Individual institutional
prescriptions in all ambulatory medical care settings after March
utilization of modern information technology, e.g. electronic
2006, which closely corresponded to release of the CDC interim
medical record system, is also certainly important in promotion
guidelines for use of antiviral agents for 2005–06 influenza season.
of new treatment guidelines and will aid in minimizing
Both findings suggest that the antiviral prescribing practice for
inappropriate use of treatment regimen in the case that guidelines
influenza treatment or prophylaxis among U.S. ambulatory
are modified [19,20]. To what extent these interventions
medical care providers was closely in line with the most up-to-
contributed to the high rates of compliance seen here is not
date global epidemiological resistance patterns, as well as the CDC
recommendations, which provides encouraging news regarding
The NAMCS and NHMACS databases do not have a specific
medical provider’s capacity to adhere with evolving changes in
focus on adamantanes prescriptions and potential emergence of
antiviral treatment recommendations, particularly relevavant to
resistance, as this is not the primary purpose of these survey tools.
the current circulating novel H1N1 influenza virus, as well as other
Accordingly, associated factors not collected in NAMCS and
potential emerging influenza pandemics.
NHAMCS, such as virus subtype coverage (i.e., influenza A versus
Prescription patterns and compliance with existing CDC
B), medication side effects, prior antiviral prescriptions, and
treatment guidelines vary by diseases. The reasons for the
clinician’s knowledge of emerging resistance, may have contrib-
variation are beyond the scope of our study. However, potential
uted to the observed trends. In addition, other factors, e.g. ease of
contributors include severity of disease, individual provider
antiviral medication administration, need to adjust dosage
perception regarding the individual patient and public health
according to age and renal function, and prior antiviral
impact of effective treatment/post-exposure prophylaxis, the
prescriptions may have contributed to the observed temporal
January 2010 | Volume 5 | Issue 1 | e8945
decline from 2002–2005 in prescription of adamantanes in U.S.
element for control and prevention of influenza, especially during
ambulatory care settings. Finally, ICD-9-CM coding, which is not
the era of emergence of resistance to anti-viral drugs.
a gold standard for influenza case reporting, was used to definecases of influenza rather than other potentially more valid
standards – e.g. laboratory confirmed tests.
Conceived and designed the experiments: Y-HH. Analyzed the data: Y-
In conclusion, our study demonstrated extremely high adher-
HH K-FC. Wrote the paper: Y-HH. Interpretation of data: K-FC. Critical
ence to the most current national treatment recommendations for
revision of the manuscript for important intellectual content: K-FC, CAG,
influenza among non-federal-employed ambulatory medical care
providers in the U.S. Adherence to such practice is an essential
1. Linder J, Bates D, Platt R (2005) Antivirals and antibiotics for influenza in the
10. Kane B, Degutis L, Sayward H, D’Onofrio G (2004) Compliance with the
United States, 1995–2002. Pharmacoepidemiol Drug Saf 14: 531–536.
Centers for Disease Control and Prevention recommendations for the diagnosis
2. Novel Swine-Origin Influenza A (H1N1) Virus Investigation Team, Dawood F,
and treatment of sexually transmitted diseases. Acad Emerg Med 11: 371–377.
Jain S, Finelli L, Shaw M, et al. (2009) Emergence of a novel swine-origin
11. Vanderweil S, Pelletier A, Hamedani A, Gonzales R, Metlay J, et al. (2007)
influenza A (H1N1) virus in humans. N Engl J Med 360: 2605–2615.
Declining antibiotic prescriptions for upper respiratory infections, 1993–2004.
3. Bright R, Shay D, Shu B, Cox N, Klimov A (2006) Adamantane resistance
among influenza A viruses isolated early during the 2005–2006 influenza season
12. Tracy C, Costabile R (2009) The evaluation and treatment of acute epididymitis
in the United States. JAMA 295(298): 891–294.
in a large university based population: are CDC guidelines being followed?
4. Centers for Disease Control and Prevention (CDC) (2006) High levels of
adamantane resistance among influenza A (H3N2) viruses and interim guidelines
13. Magid D, Stiffman M, Anderson L, Irwin K, Lyons E (2003) Adherence to CDC
for use of antiviral agents–United States, 2005–06 influenza season. MMWR
STD guideline recommendations for the treatment of Chlamydia trachomatis
infection in two managed care organizations. Sex Transm Dis 30: 30–32.
14. Grijalva C, Nuorti J, Griffin M (2009) Antibiotic prescription rates for acute
5. Dharan N, Gubareva L, Meyer J, Okomo-Adhiambo M, McClinton R, et al.
respiratory tract infections in US ambulatory settings. JAMA 302: 758–766.
(2009) Infections with oseltamivir-resistant influenza A(H1N1) virus in the
15. National Center for Health Statistics (2007) The National Ambulatory Medical
United States. JAMA 301: 1034–1041.
Care Survey (NAMCS) Description. http://www.cdc.gov/nchs/about/major/
6. Centers for Disease Control and Prevention (CDC) (2008) Interim Recommen-
ahcd/nhamcsds.htm. Accessed September 17, 2008.
dations for the Use of Influenza Antiviral Medications in the Setting of
16. Hsieh Y-H, Rothman R, Newman-Toker D, Kelen G (2008) National
Oseltamivir Resistance among Circulating Influenza A (H1N1) Viruses,
estimation of rates of HIV serology testing in US emergency departments
2008–09 Influenza Season. http://www.cdc.gov/flu/professionals/antivirals/
1993–2005: baseline prior to the 2006 Centers for Disease Control and
recommendations.htm. Accessed February 12, 2009.
Prevention recommendations. AIDS 22: 2127–2134.
7. Centers for Disease Control and Prevention (CDC) (2009) Update: drug
17. McCaig L, Woodwell D (2006) Analyzing data from the NAMCS and the
susceptibility of swine-origin influenza A (H1N1) viruses, April 2009. MMWR
NHAMCS.: CDC/National Center for Health Statistics. http://www.cdc.gov/
nchs/ahcd/ahcd_presentations.htm. Accessed December 17, 2009.
8. World Health Organization (2009) Antiviral use and the risk of drug
18. Bright R, Medina M, Xu X, Perez-Oronoz G, Wallis T, et al. (2005) Incidence
resistance - Pandemic (H1N1) 2009 briefing note 12. http://www.who.int/
of adamantane resistance among influenza A (H3N2) viruses isolated worldwide
csr/disease/swineflu/notes/h1n1_antiviral_use_20090925/en/index.html.
from 1994 to 2005: a cause for concern. Lancet 366: 1175–1181.
19. Ozdas A, Speroff T, Waitman L, Ozbolt J, Butler J, et al. (2006) Integrating
9. Health Alert Network (2006) CDC Recommends against the Use of Amantadine
‘‘best of care’’ protocols into clinicians’ workflow via care provider order entry:
and Rimantadine for the Treatment or Prophylaxis of Influenza in the United
impact on quality-of-care indicators for acute myocardial infarction. J Am Med
States during the 2005–06 Influenza Season.: Centers for Disease Control
and Prevention. http://www2a.cdc.gov/HAN/ArchiveSys/ViewMsgV.asp?
20. Asaro P, Sheldahl A, Char D (2006) Embedded guideline information without
AlertNum = 00240. Accessed December 14, 2009.
patient specificity in a commercial emergency department computerized order-entry system. Acad Emerg Med 13: 452–458.
January 2010 | Volume 5 | Issue 1 | e8945
Introduction Sandglasses - an hour of time slipping by in music In a moment you will be viewing and listening to Sandglasses , an ‘installation concert’ created by the Lithuanian composer Juste Janulyte and the Italian video artist Luca Scarzella, performed by four cellists of the Gaida Ensemble with live electronics by Michele Tadini. In this piece several aspects of Janulyte’s mus
Brampton Civic Hospital Diagnostic Imaging Preps/Instructions Nuclear Medicine Exam Prep/Instructions Bone Density No x-ray procedure involving barium for 2 weeks prior, no nuclear medicine procedure 1 week prior, no x-ray/CT Scan with contrast dye 1 week prior. Light breakfast, no fats, no caffeine (no tea, coffee, soft drinks, decaffeinated drinks, chocolate). Hold Via
 Antiviral Prescriptions to U.S. Ambulatory Care Visitswith a Diagnosis of Influenza before and after High Levelof Adamantane Resistance 2005–06 Season
Yu-Hsiang Hsieh1*, Kuan-Fu Chen1,3, Charlotte A. Gaydos2, Richard E. Rothman1,2, Gabor D. Kelen1
1 Department of Emergency Medicine, Johns Hopkins University School of Medicine, Baltimore, Maryland, United States of America, 2 Department of Medicine, Johns
Hopkins University School of Medicine, Baltimore, Maryland, United States of America, 3 Department of Emergency Medicine, Chang Gung Memorial Hospital, Taipei,
Background: Rapid emergence of influenza A viruses resistance to anti-influenza drugs has been observed in the past fiveyears. Our objective was to compare antiviral prescription patterns of ambulatory care providers to patients with a diagnosisof influenza before and after the 2005–2006 influenza season, which was temporally concordant with the emergence ofadamantane resistance. We also determined providers’ adherence to Centers for Disease Control and Prevention (CDC) 2006interim treatment guidelines for influenza after the dissemination of guidelines.
Antiviral Prescriptions to U.S. Ambulatory Care Visitswith a Diagnosis of Influenza before and after High Levelof Adamantane Resistance 2005–06 Season
Yu-Hsiang Hsieh1*, Kuan-Fu Chen1,3, Charlotte A. Gaydos2, Richard E. Rothman1,2, Gabor D. Kelen1
1 Department of Emergency Medicine, Johns Hopkins University School of Medicine, Baltimore, Maryland, United States of America, 2 Department of Medicine, Johns
Hopkins University School of Medicine, Baltimore, Maryland, United States of America, 3 Department of Emergency Medicine, Chang Gung Memorial Hospital, Taipei,
Background: Rapid emergence of influenza A viruses resistance to anti-influenza drugs has been observed in the past fiveyears. Our objective was to compare antiviral prescription patterns of ambulatory care providers to patients with a diagnosisof influenza before and after the 2005–2006 influenza season, which was temporally concordant with the emergence ofadamantane resistance. We also determined providers’ adherence to Centers for Disease Control and Prevention (CDC) 2006interim treatment guidelines for influenza after the dissemination of guidelines. and rimantadine are more appropriate options than oseltamivir
codes of 487, 487.0, 487.1 or 487.8. All visits with a diagnosis of
alone [6]. Only a few months later in the early summer of 2009,
influenza during the study period were included for analysis. Six
the first influenza pandemic in more than 40 years has arrived [2].
and rimantadine are more appropriate options than oseltamivir
codes of 487, 487.0, 487.1 or 487.8. All visits with a diagnosis of
alone [6]. Only a few months later in the early summer of 2009,
influenza during the study period were included for analysis. Six
the first influenza pandemic in more than 40 years has arrived [2]. Table 1. National estimates of ambulatory medical care visits with a diagnosis of influenza and the antiviral prescription bydemographics in the United States, 2002–2006.
Table 1. National estimates of ambulatory medical care visits with a diagnosis of influenza and the antiviral prescription bydemographics in the United States, 2002–2006. Table 2. National estimates of ambulatory medical care visits with a diagnosis of influenza and the antiviral prescription byinfluenza season, high adamantane resistance period, and announcement of 2006 CDC guidelines in the United States, 2002–2006.
Table 2. National estimates of ambulatory medical care visits with a diagnosis of influenza and the antiviral prescription byinfluenza season, high adamantane resistance period, and announcement of 2006 CDC guidelines in the United States, 2002–2006.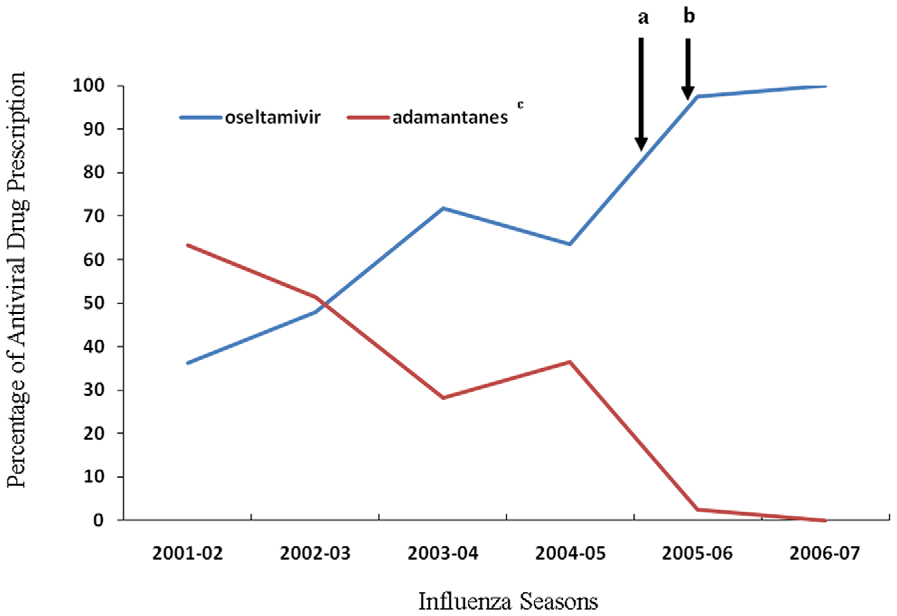
 Figure 1. Prescription of anti-influenza agents for patient visits with a diagnosis of influenza in US ambulatory care includingemergency department visits, outpatient visits and physician office visits, by antiviral drug, influenza season 2001–2007. a The timeCDC declared interim guidelines for use of anti-influenza drugs. b The start of high adamantane resistance period. c Adamantanes include amantadineand rimantadine.
Figure 1. Prescription of anti-influenza agents for patient visits with a diagnosis of influenza in US ambulatory care includingemergency department visits, outpatient visits and physician office visits, by antiviral drug, influenza season 2001–2007. a The timeCDC declared interim guidelines for use of anti-influenza drugs. b The start of high adamantane resistance period. c Adamantanes include amantadineand rimantadine. decline from 2002–2005 in prescription of adamantanes in U.S.
decline from 2002–2005 in prescription of adamantanes in U.S.