Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 1 of 13
Phys Ther. 2009 April; 89(4): 384–393.
Copyright 2009, American Physical Therapy Association
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor Agility Exercise Program
LA King, PT, PhD, is Post-doctoral Fellow, Oregon Health and Sciences University, Portland, Oregon. FB Horak, PT, PhD, is Research Professor of Neurology and Adjunct Professor of Physiology and Biomedical Engineering, Department of Neurology, Oregon Health and Sciences University, West Campus, Building 1, 505 NW 185th Ave, Beaverton, OR 97006-3499 (USA). Address all correspondence to Dr Horak at: [email protected]
Received July 11, 2008; Accepted January 12, 2009.
This article has been cited by other articles in PMC. Abstract
This article introduces a new framework for therapists to develop an exercise program to delay mobility
disability in people with Parkinson disease (PD). Mobility, or the ability to efficiently navigate and
function in a variety of environments, requires balance, agility, and flexibility, all of which are affected by
PD. This article summarizes recent research identifying how constraints on mobility specific to PD,
such as rigidity, bradykinesia, freezing, poor sensory integration, inflexible program selection, and
impaired cognitive processing, limit mobility in people with PD. Based on these constraints, a
conceptual framework for exercises to maintain and improve mobility is presented. An example of a
constraint-focused agility exercise program, incorporating movement principles from tai chi, kayaking,
boxing, lunges, agility training, and Pilates exercises, is presented. This new constraint-focused agility
exercise program is based on a strong scientific framework and includes progressive levels of
sensorimotor, resistance, and coordination challenges that can be customized for each patient while
maintaining fidelity. Principles for improving mobility presented here can be incorporated into an
ongoing or long-term exercise program for people with PD.
Most people who are diagnosed with Parkinson disease (PD) do not consult with a physical therapist
until they already have obvious mobility problems. However, it is possible that a rigorous exercise
program that focuses on anticipated problems, which are inevitable with progression of the disease,
may help patients who do not yet exhibit mobility problems. Although there are excellent guidelines for
physical therapists to treat patients with PD who exhibit mobility problems in order to improve or
maintain their mobility,1,2 there is little research on whether exercise may delay or reduce the eventual
mobility disability in patients diagnosed with PD.
The major cause of disability in people with PD is impaired mobility.3 Mobility, the ability of a person to
move safely in a variety of environments in order to accomplish functional tasks,4 requires dynamic
neural control to quickly and effectively adapt locomotion, balance, and postural transitions to changing
environmental and task conditions. Such dynamic control requires sensorimotor agility, which involves
coordination of complex sequences of movements, ongoing evaluation of environmental cues and
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664996/?tool=pubmed
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 2 of 13
contexts, the ability to quickly switch motor programs when environmental conditions change, and the
ability to maintain safe mobility during multiple motor and cognitive tasks.5,6 The types of mobility
deficits inevitable with the progression of PD suggest that the basal ganglia are critical for sensorimotor
agility.2 Critical aspects of mobility disability in people with PD, such as postural instability, are
unresponsive to pharmacological and surgical therapies,7 making preventative exercise an attractive
option. As yet, there is no known ongoing exercise program for people diagnosed with PD that focuses
on maintaining or improving their agility to slow or reduce their decline in mobility.
This article uses the known sensorimotor impairments of PD that affect balance, gait, and postural
transitions to develop a conceptual framework to design exercises that aim to delay disability and
maintain or improve mobility in people with PD. This framework is based on the current knowledge of
the neurophysiology of PD and the inevitable constraints on mobility resulting from basal ganglia
degeneration. The scientifically based principles presented here, which are focused on mobility
disorders in people with PD, can be incorporated into an existing therapy program for people with PD.
Based on this framework, this article also presents an example of a novel sensorimotor agility program
that we are currently testing in a clinical trial. This program is unique in that it encourages a partnership
among physical therapists, exercise trainers, and patients to set up, progress, and re-evaluate an
exercise program that ultimately can be carried out independently in the community. It is likely that a
mobility program, such as the one presented here, would need to be sustained and modified
throughout the course of the disease to maintain maximal benefit. Why Exercise May Prevent or Delay Mobility Disability in People With PD
Exciting new findings in neuroscience regarding the effects of exercise on neural plasticity and
neuroprotection of the brain against neural degeneration suggest that an intense exercise program can
improve brain function in patients with neurological disorders. Specifically, animal studies have
demonstrated neurogenesis,8 an increase in dopamine synthesis and release,9 and increased
dopamine in the striatum following acute bouts of exercise.10 Such changes in the brain may affect
behavioral recovery as a result of neuroplasticity (the ability of the brain to make new synaptic
connections), neuroprotection, and slowing of neural degeneration.11,12 Studies with parkinsonian rats
have suggested that chronic exercise may help reverse motor deficits in animals by changing brain
function. Specifically, rats that ran on a treadmill showed preservation of dopaminergic cell bodies and
terminals11,13 associated with improved running distance and speed,12 indicating a neuroprotective
effect of exercise. Conversely, nonuse of a limb induced by casting in parkinsonian rats increased
motor deficits as well as loss of dopaminergic terminals.11 Aerobic exercise, such as treadmill training
and walking programs, has been tested in individuals with PD and has been shown to improve gait
parameters, quality of life, and levadopa efficacy.14–16 However, it is not clear whether aerobic training,
by itself, is the best approach to improving mobility, which depends upon dynamic balance, dual
tasking, negotiating complex environments, quick changes in movement direction, and other
sensorimotor skills affected by PD. It is possible that treadmill training, for example, could be even
more effective for addressing complex mobility issues for people with PD if the therapist could
incorporate tasks such as dual tasking, balance training, and set-switching into a treadmill program.
There currently are many untested exercise programs available for people with PD17–19 as well as
several randomized controlled studies that test specific exercises, such as strength (force-generating
capacity) training or gait training.20–29 The approach presented in this article is focused on exercises
that challenge sensorimotor control of dynamic balance and gait to improve mobility in people with PD.
There are many other aspects of PD that also must be addressed in rehabilitation.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664996/?tool=pubmed
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 3 of 13
Drive Neuroplasticity With Task-Specific Agility Exercise
Studies in rats have demonstrated that task-specific agility training (eg, acrobatic, environmental
enrichment-type, high-beam balance course) results in larger improvements in motor skills as well as
larger changes in synaptic plasticity than simple, repetitive aerobic training such as running on
treadmills.30–35 Task-specific exercise also has been shown to be more effective than aerobic or
general exercise to improve task performance in patients with stroke.36,37 Task-specific exercises
targeted at a single, specific balance or gait impairment in patients with PD have been shown to be
effective. For example, exercises targeted at improving small step size, poor axial mobility, difficulty
with postural transitions, small movement amplitude, or slow speed of compensatory stepping have
individually been shown to be effective in improving each particular aspect of mobility.18,22,38–42 We have
borrowed singular techniques from several successful programs and combined them with task-specific
components of mobility and systematic sensorimotor challenges into a comprehensive exercise
program directed at delaying and reducing mobility problems in individuals with PD. Reduce Mobility Constraints With Exercise
People with mild or newly diagnosed PD often do not have obvious muscle weakness or poor
balance.43 Nevertheless, the literature suggests that muscle weakness, secondary to abnormal muscle
activation associated with bradykinesia and rigidity, can be present at all stages of PD.44–47 Similarly,
balance and mobility problems may be present in people with mild PD but only become apparent when
more-complex coordination is required under challenging conditions.48,49 For example, mobility
problems may only be apparent when an individual with PD is attempting to walk quickly in a cluttered
environment while talking on a cell phone. As the disease progresses, balance problems become more
apparent, just as patients begin to show impaired kinesthesia and inability to quickly change postural
strategies.50,51 The basal ganglia affect balance and gait by contributing to automaticity, self-initiated
gait and postural transitions, changing motor programs quickly, sequencing actions, and using
proprioceptive information for kinesthesia and multisegmental coordination.52–54 During the progression
of PD, mobility is progressively constrained by rigidity, bradykinesia, freezing, sensory integration,
inflexible motor program selection, and attention and cognition.2 Table 1 summarizes constraints on
mobility due to PD, the impact of these constraints on mobility, and the goals of exercises that could
potentially reduce the impact of each constraint.
Parkinsonian Constraints Affecting Mobility and Exercise Principles
Designed to Reduce These ConstraintsaConstraints Affecting Mobility in People With PD, With Implications for the Sensorimotor Agility Program Rigidity
Parkinsonian rigidity is characterized by an increased resistance to passive movement throughout the
entire range of motion, in both agonist and antagonist muscle groups.55–57 The functional outcomes of
rigidity, in general, include a flexed posture,58 lack of trunk rotation,59,60 and reduced joint range of
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664996/?tool=pubmed
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 4 of 13
movement during postural transitions and gait.56,61 Electromyography studies have shown that people
with PD have high tonic background activity, especially in the flexors, and co-contraction of muscles
during movement, especially in the axial muscles.56,57 In addition, antagonist muscle activation is larger
and earlier, resulting in coactivation of muscle groups during automatic postural responses.61
Another characteristic of parkinsonian rigidity is axial rigidity, which results in a loss of natural vertebral,
pelvis/shoulder girdle, and femur/pelvis flexibility and range of motion that accompanies efficient
postural and locomotor activities.60,62 Wright et al55 found that rigidity in the neck, torso, and hips of
standing subjects was 3 to 5 times greater in subjects with PD than in age-matched control subjects
when measuring the torsional resistance to passive movement along the longitudinal axis during
twisting movements. Levodopa medication did not improve their axial rigidity.55 The high axial tone
(velocity-dependent resistance to stretch) in patients with PD contributes to their characteristic “en bloc”
trunk motions, which make it difficult for them to perform activities such as rolling over in bed or turning
Schenkman et al63 showed that exercise can increase trunk flexibility in people with PD. We propose an
agility program that includes movements that minimize agonist-antagonist muscle co-contraction (ie,
reciprocal movements), promote axial rotation, lengthen the flexor muscles, and strengthen the
extensor muscles to promote an erect posture. Rigidity can potentially be addressed with kayaking, an
exercise in which the person counter-rotates the shoulder and pelvic girdle; tai chi, a set of exercises
that focuses on the individual's awareness of postural alignment during postural transitions; and pre-
Pilates, a series of exercises aimed at increasing spinal mobility and lengthening flexor muscles
groups. In addition, the program should include strategies for turning and transitioning from a standing
position to sitting on the floor and back again that emphasize trunk and head rotation (Tabs. 2 and 3
Representative Agility Exercise Program, With Progressions
Bradykinesia
Bradykinesia is most commonly defined as slowness of voluntary movement,43 but it also is associated
with slow and weak postural responses to perturbations and anticipatory postural adjustments.
Reactive postural responses to surface translations61,64 and anticipatory postural movements prior to
rising onto toes65 and prior to step initiation66 are bradykinetic in patients with PD. Bradykinetic
voluntary stepping and postural compensatory stepping are characterized by a delayed time to lift the
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664996/?tool=pubmed
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 5 of 13
swing limb, a weak push-off, reduced leg lift, a small stride length, and lack of arm swing.61,64,66,67
Bradykinesia also is apparent in reduced voluntary and reactive limits of stability, especially in the
backward direction.64,68 The characteristic narrow stance of patients with PD may be compensatory for
bradykinetic anticipatory postural adjustments prior to a step, at the expense of reduced lateral postural
stability.67,69 Bradykinetic postural responses in people with PD generally are not improved by
antiparkinsonian medications, highlighting the need for an exercise approach to this constraint on
mobility.6 Bradykinesia also is seen in postural transitions such as turning70 and the supine-to-stand
manuever,59 as well as in single-joint movements71 and multi-joint reaching movements72 in people with
Bradykinesia is evident in slowed rate of increase and decrease of muscle activation patterns.73
Reduction in muscle strength in people with PD has been attributed primarily to reduced cortical drive
to muscles because voluntary contraction, but not muscle response to nerve stimulation, is weak in
these individuals.74,75 Electromyographic activity in bradykinetic muscles often is fractionated into
multiple bursts and is not well scaled for changes in movement distance or velocity.71 Years of
bradykinesia from abnormal, centrally driven muscle control and abnormal, inefficient patterns of
muscle recruitment limit functional mobility and eventually may result in focal muscle weakness.
Because bradykinesia is due to impaired central neural drive, rehabilitation to reduce bradykinesia
should focus on teaching patients to increase the speed, amplitude, and temporal pacing of their self-
initiated and reactive limb and body center-of-mass (CoM) movements. Table 2 presents representative
exercises aimed at reducing bradykinesia for mobility. These exercises may promote weight-shift
control and postural adjustments in anticipation of voluntary movements such as lunges, kicks, and
quick boxing movements. Patients also practice taking large, protective steps while tilting past their
limits of stability and in response to external displacements associated with hitting or punching a boxing
bag. To reduce bradykinesia, patients should be encouraged to “think big”42 while increasing the speed
and amplitude of large arm and leg movements throughout agility courses and during multidirectional
). Walking sticks may help patients attend to the large, symmetrical
arm swing that is coordinated with strides during gait. Freezing
Freezing of gait manifests as a movement hesitation in which a delay or complete inability to initiate a
step occurs.76 Freezing not only slows walking, but it also is a major contributor to falls in people with
PD.77 It is a poorly understood phenomenon that is associated with executive disorders in people with
PD.76,78 Freezing during gait occurs more often when a person is negotiating a crowded environment or
narrow doorway, when making a turn, or when attention is diverted by a secondary task.77,79 Jacobs
and Horak80 recently found that freezing or “start hesitation” in step initiation is associated with
repetitive, anticipatory, lateral weight shifts and that people who are healthy can be made to “freeze”
when they do not have time to preplan which foot to use when initiating a compensatory or voluntary
step. Therefore, freezing may be related to difficulties in shifts of attention, preplanning movement
strategies, or quickly selecting a correct central motor program.
To help people in the early stages of PD reduce their chances of being affected by freezing, agility
exercises should be performed in environments in which freezing typically occurs. As shown in
Tables 2 and 3, exercises that involve high stepping, skipping, or taking large steps in different directions through doorways and over and around obstacles, such as between chairs placed shoulder-
width apart, could potentially reduce freezing episodes. Quick turns should be practiced in corners and
near walls. Individuals with PD could perform these exercises in the home or gym, where obstacle
courses have been set up that require turning quickly, negotiating narrow and tight spaces such as
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664996/?tool=pubmed
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 6 of 13
corners, ducking under and stepping over obstacles, picking up objects while walking, and quickly
changing directions and foot placement. Once a person successfully performs the agility exercises on
an obstacle course, more-advanced progressions could be introduced, such as performing dual
cognitive tasks while maintaining form and speed on agility tasks. Inflexible Program Selection and Poor Sequential Coordination
Research suggests that the basal ganglia play an important role in task switching, motor program
selection, and suppression of irrelevant information before executing an action.52 The inability to quickly
switch motor programs has been demonstrated in individuals with PD by an inability to change postural
response synergies in the first perturbation trial after a change in support, change in instructions, or
change in perturbation direction.51,81 Dopamine replacement does not improve inflexible program
selection.82,83 The difficulty with switching motor programs manifests in difficulty maneuvering in new
and challenging environments and in changes in postural transitions, such as turning, standing from a
sitting position, and rolling over.84 In addition to difficulty switching motor programs, people with PD
have difficulty sequencing motor actions.65,85,86 Patients with PD show a delay between their
anticipatory postural adjustments and voluntary movements, such as rising onto toes65 or a voluntary
step.66 These findings suggest that mobility in people with PD is constrained by poor coordination
among body parts and between voluntary movements and their associated postural adjustments, as
well as by difficulty in switching motor programs appropriate for changes in task constraints.
Consequently, an exercise program should include complex, multisegmental, whole-body movements
and should include tasks requiring quick selection and sequencing of motor programs such as
practicing postural transitions (eg, moving from stance to the floor, rolling, and arising from the floor to
stance). As shown in Table 2, one such exercise approach is tai chi, which helps patients to learn
increasingly complex sequences of movement and to focus on smooth timing and synchronization of
whole-body movements. Incorporating boxing actions into a remembered sequence is another way to
practice the quick selection and sequencing of complex motor programs for mobility. To address
problems of quick program selection, lunges and agility exercises also provide practice changing motor
strategies during stopping, starting, changing direction, changing stepping limb, and changing the size
Sensory Integration
There is strong evidence that the basal ganglia are critical for high-level integration of somatosensory
and visual information necessary to form an internal representation of the body and the
environment.87,88 Despite clinical examinations of patients with PD revealing only inconsistent, subtle
signs of abnormal sensory perception,89,90 an increasing number of studies are showing abnormal
kinesthesia and use of proprioception in people with PD. For example, Wright et al55 and Horak et al64
found that individuals with PD have an impaired ability to detect the rotation of a surface or the passive
rotation of the torso and that this poor kinesthesia is worsened by levodopa medication. Individuals with
PD also show impaired perception of arm position and movement and decreased response to muscle
vibration.91–93 The poor use of proprioceptive information and decreased perception of movement are
associated with over-estimation of body motion (bradykinesia) and over-dependence on vision.50,94
To facilitate use of proprioceptive information and reduce over-reliance on vision, an agility program
should progress balancing and walking tasks by: (1) wearing dark sunglasses to reduce visual contrast
sensitivity and (2) use of “no body” glasses to obscure the bottom half of the visual field so the body
cannot be seen. In addition, many of the exercises can be performed on a variety of surfaces to require
adaptation to altered somatosensory information from the surface. External feedback and sensory cues
from the therapist regarding quality and size of the movements should be used initially and
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664996/?tool=pubmed
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 7 of 13
progressively decreased as patients develop a more accurate internal sense of body position. As
shown in Table 3, the sensorimotor agility program used as an example in this article progresses with
traditional progressive challenges95 (increasing resistance, speed of gait, endurance, and so on) and
with sensorimotor challenges (dual tasking and changes in base of support, visual input, and surface
Cognitive Constraints
The inability to simultaneously carry out a cognitive task and a balance or walking task has been found
to be a predictor of falls in elderly people.96 It is even more difficult for a person with PD than age-
matched elderly people to perform multiple tasks,86 possibly because the basal ganglia are responsible
for allowing automatic control of balance and gait and for switching attention between tasks.52,86
Postural sway increases most in individuals with PD who have a history of falls when a cognitive task is
added to the task of quiet stance.97 These findings suggest that the ability to carry out a secondary
cognitive or motor tasks while walking or balancing is a critical element of mobility that is a particular
An agility program could progress task difficulty by adding cognitive or motor tasks that teach patients
with PD to maintain postural stability during performance of secondary tasks. Table 3 presents
exercises in which it is safe and appropriate to add a dual cognitive or motor task. The exercises at
level 1 have no dual tasks, level 2 has a motor task (eg, bouncing a ball) added to the basic exercise
such as an agility course, and level 3 has a cognitive task (eg, performing math or memory problems)
added to the same basic exercise. The progression of adding secondary tasks to gait and balance
tasks serves as a training device as well as a tool to help patients understand the relationship between
safe mobility and secondary tasks in everyday life. A Sensorimotor Agility Program for People With PD
In this article, we propose a novel sensorimotor agility program targeted at constraints on mobility in
people with PD. The expertise that contributed to the program includes an internationally recognized
neurologist specializing in movement disorders for more 35 years and 5 physical therapists
experienced in treating people with PD, including 3 with PhDs with a focus on PD. Six certified athletic
trainers who regularly work with people with PD also were helpful in designing the program. We
propose that the exercise program outlined in Table 2 could last 60 minutes, with about 10 minutes for
each category of exercise. The exercises in the 6 categories were selected to target one or more of the
Although not all people with PD have all of the constraints addressed in this article, it may be that
exercise should target all of these constraints, as each constraint generally is associated with the
progression of PD and eventually has a marked effect on mobility. Addressing constraints early may
delay the onset of related mobility deficits. Category I, “tai chi,” is a whole-body exercise that focuses
on developing a sense of body kinesthesia, improving postural alignment, and sequencing of whole-
body movements that move the CoM. Category II, “kayaking,” focuses on trunk and cervical rotation
and speed, with large, coordinated arm movements. Category III, “agility course,” focuses on quickly
changing motor programs such as quick turns, sequencing actions, and overcoming freezing. Category
IV, “boxing,” focuses on building the patient's agility and speed, backward walking, and components of
anticipatory and reactive postural adjustments in response to a moving bag. Category V, “lunges,”
helps patients with PD practice large CoM movements, multidirectional limits of stability, and steps for
postural correction. Category VI, “pre-Pilates,” is a set of exercises that help patients with PD extend
and strengthen the spine, as well as practice postural transitions such as sit-to-stand maneuvers, floor
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664996/?tool=pubmed
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 8 of 13
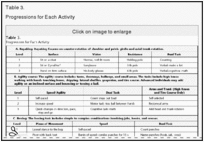
The sensorimotor progressions of exercises II through V follow 3 levels of difficulty (Tab. 3).
Progressions include: (1) reducing the base of support, (2) increasing surface compliance to reduce
surface somatosensory information for postural orientation, (3) increasing speed or resistance with
weights, (4) adding secondary cognitive tasks to automate posture and gait, and (5) limiting visual input
of the body with “no body” glasses or of the environment with dark sunglasses to increase use of
kinesthetic information. Category I (tai chi) and category Vl (pre-Pilates) exercises progress by
increasing the length of remembered sequences and improving the form of each subcomponent of the
movements. All of these sensorimotor progressions were chosen specifically to target the predictable
constraints on mobility due to PD, and testing of the program is currently under way.
We present a progressive sensorimotor agility exercise program for prevention of mobility disability in
people with PD. The program is based on the role of the basal ganglia in posture and gait, the
principles of neural plasticity, and the inevitable constraints of PD that ultimately affect dynamic balance
and mobility. These principles of the program include a focus on self-initiated movements, big and
quick movements, large and flexible CoM control, reciprocal and coordinated movements of arms and
legs, and rotational movements of torso over pelvis and pelvis over legs. Flexible, rotational axial
motion of trunk and neck are stressed to achieve erect postural alignment, strengthening of extensors,
and lengthening of flexors. Our program is designed to facilitate sensory integration for balance,
emphasizing the use of somatosensory information to move the body's CoM quickly and effectively for
balance and mobility. Secondary cognitive tasks are added to mobility tasks to automatize control of
balance and gait. This sensorimotor agility approach to mobility training is intended for prevention of
mobility disability but may be modified for patients at later stages of PD progression to improve their
Both authors provided concept/idea/project design, writing, and project management. Dr Horak provided fund procurement,
facilities/equipment, institutional liaisons, and consultation (including review of manuscript before submission).
The exercise program developed out of brainstorming sessions with the following expert neurologists, scientists, physical therapists, and
trainers: Fay B Horak, PT, PhD, Jay Nutt, MD, Laurie A King, PT, PhD, Sue Scott, CT, Andrea Serdar, PT, CNS, Chad Swanson, CT,
Valerie Kelly, PT, PhD, Ashley Scott, CT, David Vecto, CT, Triana Nagel-Nelson, CT, Kimberly Berg, CT, Nandini Deshpande, PT, PhD,
and Cristiane Zampieri, PT, PhD. Strawberry Gatts, PhD, provided expert advice to select and modify tai chi moves for people with
This work was supported by a grant from the Kinetics Foundation and by a grant from the National Institute on Aging (AG006457).
Dr Horak was a consultant for the Kinetics Foundation. This potential conflict of interest has been reviewed and managed by Oregon
References 1. Keus SH, Bloem BR, Hendriks EJ, et al. Evidence-based analysis of physical therapy in Parkinson's disease with
recommendations for practice and research. Mov Disord. 2007;22:451–460. [PubMed]
2. Morris ME. Movement disorders in people with Parkinson disease: a model for physical therapy. Phys Ther. 2000;80:578–597.
3. Wood BH, Bilclough JA, Bowron A, Walker RW. Incidence and prediction of falls in Parkinson's disease: a prospective
multidisciplinary study. J Neurol Neurosurg Psychiatry. 2002;72:721–725. [PMC free article] [PubMed]
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664996/?tool=pubmed
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 9 of 13
4. Patla AE, Shumway-Cook A. Dimensions of mobility: defining the complexity and difficulty associated with community mobility.
J Aging Phys Act. 1998;7:7–19. 5. Shumway-Cook A, Woollacott M. Motor Control: Theory and Practical Applications. Baltimore, MD: Williams & Wilkins; 1995. 6. Horak FB, Macphearson MJ. Postural orientation and equilibrium. In: Rowell LB, Shepherd JR, eds. Handbook of Physiology, Section 12: Exercise: Regulation and Integration of Multiple Systems. New York, NY: Oxford University Press; 1996:255–292. 7. Bloem BR, van Vugt JP, Beckley DJ. Postural instability and falls in Parkinson's disease. Adv Neurol. 2001;87:209–223.
8. van Praag H, Kempermann G, Gage FH. Running increases cell proliferation and neurogenesis in the adult mouse dentate
gyrus. Nat Neurosci. 1999;2:266–270. [PubMed]
9. Heyes MP, Garnett ES, Coates G. Nigrostriatal dopaminergic activity is increased during exhaustive exercise stress in rats.
Life Sci. 1988;42:1537–1542. [PubMed]
10. Meeusen R, De Meirleir K. Microdialysis as a method to measure central catecholamines during exercise. Med Sci Sports 11. Tillerson JL, Cohen AD, Caudle WM, et al. Forced nonuse in unilateral parkinsonian rats exacerbates injury. Neuroscience.
12. Fisher BE, Petzinger GM, Nixon K, et al. Exercise-induced behavioral recovery and neuroplasticity in the 1-methyl-4-phenyl-
1,2,3,6-tetrahydropyridine-lesioned mouse basal ganglia. J Neurosci Res. 2004;77:378–390. [PubMed]
13. Tillerson JL, Caudle WM, Reveron ME, Miller GW. Exercise induced behavioral recovery and attenuates neurochemical
deficits in rodent models of Parkinson's disease. Neuroscience. 2003;119:899–911. [PubMed]
14. Herman T, Giladi N, Gruendlinger L, Hausdorff JM. Six weeks of intensive treadmill training improves gait and quality of life in
patients with Parkinson's disease: a pilot study. Arch Phys Med Rehabil. 2007;88:1154–1158. [PubMed]
15. van Eijkeren FJ, Reijmers RS, Kleinveld MJ, et al. Nordic walking improves mobility in Parkinson's disease. Mov Disord.
16. Muhlack S, Welnic J, Woitalla D, Muller T. Exercise improves efficacy of levodopa in patients with Parkinson's disease. Mov Disord. 2007;22:427–430. [PubMed]
17. Cianci H. Parkinson's Disease: Fitness Counts. 3rd ed. Miami, FL: National Parkinson Foundation; 2006. 18. Argue J. Parkinson's Disease and the Art of Moving. Oakland, CA: New Harbinger Publications; 2000. 19. Zid D. Delay the Disease: Exercise and Parkinson's Disease. Columbus, OH: Columbus Health Works Production; 2007. 20. Palmer SS, Mortimer JA, Webster DD, et al. Exercise therapy for Parkinson's disease. Arch Phys Med Rehabil. 1986;67:741–
21. Comella CL, Stebbins GT, Brown-Toms N, Goetz CG. Physical therapy and Parkinson's disease: a controlled clinical trial.
Neurology. 1994;44(3 pt 1):376–378. [PubMed]
22. Schenkman M, Cutson TM, Kuchibhatla M, et al. Exercise to improve spinal flexibility and function for people with Parkinson's
disease: a randomized controlled trial. J Am Geriatr Soc. 1998;46:1207–1216. [PubMed]
23. Hirsch MA, Toole T, Maitland CG, Rider RA. The effects of balance training and high-intensity resistance training on persons
with idiopathic Parkinson's disease. Arch Phys Med Rehabil. 2003;84:1109–1117. [PubMed]
24. Ellis T, de Goede CJ, Feldman RG, et al. Efficacy of physical therapy program in patients with Parkinson's disease: a
randomized controlled trial. Arch Phys Med Rehabil. 2005;86:626–632. [PubMed]
25. Protas EJ, Mitchell K, Williams A, et al. Gait and step training to reduce falls in Parkinson's disease. NeuroRehabilitation.
26. Burini D, Farabollini B, Iacucci S, et al. A randomised controlled cross-over trial of aerobic training versus Qigong in advanced
Parkinson's disease. Eura Medicophys. 2006;42:231–238. [PubMed]
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664996/?tool=pubmed
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimot. Page 10 of 13
27. Dibble LE, Hale TF, Marcus RL, et al. High-intensity resistance training amplifies muscle hypertrophy and functional gains in
persons with Parkinson's disease. Mov Disord. 2006;21:1444–1452. [PubMed]
28. Schmitz-Hubsch T, Pyfer D, Kielwein K, et al. Qigong exercise for the symptoms of Parkinson's disease: a randomized,
controlled pilot study. Mov Disord. 2006;21:543–548. [PubMed]
29. Ashburn A, Fazakarley L, Ballinger C, et al. A randomised controlled trial of a home based exercise programme to reduce the
risk of falling among people with Parkinson's disease. J Neurol Neurosurg Psychiatry. 2007;78:678–684. [PMC free article]
30. Schmidt RA. Motor Control and Learning: A Behavioral Emphasis. Champaign, IL: Human Kinetics Inc; 1982. 31. Chu CJ, Jones TA. Experience-dependent structural plasticity in cortex heterotopic to focal sensorimotor cortical damage.
Exp Neurol. 2000;166:403–414. [PubMed]
32. Isaacs KR, Anderson BJ, Alcantara AA, et al. Exercise and the brain: angiogenesis in the adult rat cerebellum after vigorous
physical activity and motor skill learning. J Cereb Blood Flow Metab. 1992;12:110–119. [PubMed]
33. Colcombe S, Kramer AF. Fitness effects on the cognitive function of older adults: a meta-analytic study. Psychol Sci.
34. Black JE, Isaacs KR, Anderson BJ, et al. Learning causes synaptogenesis, whereas motor activity causes angiogenesis, in
cerebellar cortex of adult rats. Proc Natl Acad Sci USA. 1990;87:5568–5572. [PMC free article] [PubMed]
35. Anderson BJ, Alcantara AA, Greenough WT. Motor-skill learning: changes in synaptic organization of the rat cerebellar
cortex. Neurobiol Learn Mem. 1996;66:221–229. [PubMed]
36. Sullivan KJ, Brown DA, Klassen T, et al. Effects of task-specific locomotor and strength training in adults who were
ambulatory after stroke: results of the STEPS randomized clinical trial. Phys Ther. 2007;87:1580–1602; discussion 1603–1587.
37. Wolf SL, Winstein CJ, Miller JP, et al. Retention of upper limb function in stroke survivors who have received constraint-
induced movement therapy: the EXCITE randomised trial. Lancet Neurol. 2008;7:33–40. [PMC free article] [PubMed]
38. Morris M, Iansek R, Matyas TA, Summers JJ. Stride length regulation in Parkinson's disease normalization strategies and
underlying mechanisms. Brain. 1996;119:551–568. [PubMed]
39. Viliani T, Pasquetti P, Magnolfi S, et al. Effects of physical training on straightening-up processes in patients with Parkinson's
disease. Disabil Rehabil. 1999;21:68–73. [PubMed]
40. Mak MK, Hui-Chan CW. Cued task-specific training is better than exercise in improving sit-to-stand in patients with
Parkinson's disease: a randomized controlled trial. Mov Disord. 2008;23:501–509. [PubMed]
41. Jobges M, Heuschkel G, Pretzel C, et al. Repetitive training of compensatory steps: a therapeutic approach for postural
instability in Parkinson's disease. J Neurol Neurosurg Psychiatry. 2004;75:1682–1687. [PMC free article] [PubMed]
42. Farley BG, Koshland GF. Training BIG to move faster: the application of the speed-amplitude relation as a rehabilitation
strategy for people with Parkinson's disease. Exp Brain Res. 2005;167:462–467. [PubMed]
43. Melnick M. Neurologic Rehabilitation. 3rd ed. St Louis, MO: Mosby; 1995. 44. Wierzbicka MM, Wiegner AW, Logigian EL, Young RR. Abnormal most-rapid isometric contractions in patients with
Parkinson's disease. J Neurol Neurosurg Psychiatry. 1991;54:210–216. [PMC free article] [PubMed]
45. Stelmach GE, Teasdale N, Phillips J, Worringham CJ. Force production characteristics in Parkinson's disease. Exp Brain 46. Corcos DM, Chen CM, Quinn NP, et al. Strength in Parkinson's disease: relationship to rate of force generation and clinical
status. Ann Neurol. 1996;39:79–88. [PubMed]
47. Inkster LM, Eng JJ, MacIntyre DL, Stoessl AJ. Leg muscle strength is reduced in Parkinson's disease and relates to the ability
to rise from a chair Mov Disord. 2003;18:157–162. [PubMed]
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664996/?tool=pubmed
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimot. Page 11 of 13
48. Carpinella I, Crenna P, Calabrese E, et al. Locomotor function in the early stage of Parkinson's disease. IEEE Trans Neural Syst Rehabil Eng. 2007;15:543–551. [PubMed]
49. Rochester L, Hetherington V, Jones D, et al. Attending to the task: interference effects of functional tasks on walking in
Parkinson's disease and the roles of cognition, depression, fatigue, and balance. Arch Phys Med Rehabil. 2004;85:1578–1585.
50. Maschke M, Gomez CM, Tuite PJ, Konczak J. Dysfunction of the basal ganglia, but not the cerebellum, impairs kinaesthesia.
Brain. 2003;126(pt 10):2312–2322. [PubMed]
51. Chong RK, Horak FB, Woollacott MH. Parkinson's disease impairs the ability to change set quickly. J Neurol Sci. 2000;175:57
52. Yehene E, Meiran N, Soroker N. Basal ganglia play a unique role in task switching within the frontal-subcortical circuits:
evidence from patients with focal lesions. J Cogn Neurosci. 2008;20:1079–1093. [PubMed]
53. Taniwaki T, Okayama A, Yoshiura T, et al. Reappraisal of the motor role of basal ganglia: a functional magnetic resonance
image study. J Neurosci. 2003;23:3432–3438. [PubMed]
54. Brown P, Marsden CD. What do the basal ganglia do? Lancet. 1998;351(9118):1801–1804. [PubMed]
55. Wright WG, Gurfinkel VS, Nutt JG, et al. Axial hypertonicity in Parkinson's disease: direct measurements of trunk and hip
torque. Exp Neurol. 2007;208:38–46. [PMC free article] [PubMed]
56. Burleigh A, Horak FB, Nutt JG, Frank JS. Levodopa reduces muscle tone and lower extremity tremor in Parkinson's disease.
Can J Neurol Sci. 1995;22:280–285. [PubMed]
57. Mak MK, Wong EC, Hui-Chan CW. Quantitative measurement of trunk rigidity in parkinsonian patients. J Neurol.
58. Jacobs JV, Dimitrova DM, Nutt JG, Horak FB. Can stooped posture explain multidirectional postural instability in patients with
Parkinson's disease? Exp Brain Res. 2005;166:78–88. [PMC free article] [PubMed]
59. Schenkman ML, Morey M, Kuchibhatla M. Spinal flexibility and balance control among community-dwelling adults with and
without Parkinson's disease. J Gerontol A Biol Sci Med Sci. 2000;55:M441–M445. [PubMed]
60. Schenkman ML, Clark K, Xie T, et al. Spinal movement and performance of a standing reach task in participants with and
without Parkinson disease. Phys Ther. 2001;81:1400–1411. [PubMed]
61. Dimitrova D, Horak FB, Nutt JG. Postural muscle responses to multidirectional translations in patients with Parkinson's
disease. J Neurophysiol. 2004;91:489–501. [PubMed]
62. Vaugoyeau M, Viallet F, Aurenty R, et al. Axial rotation in Parkinson's disease. J Neurol Neurosurg Psychiatry. 2006;77:815–
63. Schenkman ML, Cutson TM, Kuchibhatla M, et al. Exercise to improve spinal flexibility and function for people with
Parkinson's disease: a randomized, controlled trial. J Am Geriatr Soc. 1998;46:1207–1216. [PubMed]
64. Horak FB, Dimitrova D, Nutt JG. Direction-specific postural instability in subjects with Parkinson's disease. Exp Neurol.
65. Frank JS, Horak FB, Nutt JG. Centrally initiated postural adjustments in parkinsonian patients on and off levodopa. J Neurophysiol. 2000;84:2440–2448. [PubMed]
66. Burleigh-Jacobs A, Horak FB, Nutt JG, Obeso JA. Step initiation in Parkinson's disease: influence of levodopa and external
sensory triggers. Mov Disord. 1997;12:206–215. [PubMed]
67. King LA, Horak FB. Lateral stepping for postural correction in Parkinson's disease. Arch Phys Med Rehabil. 2008;89:492–
68. Mancini M, Rocchi L, Horak FB, Chiari L. Effects of Parkinson's disease and levodopa on functional limits of stability. Clin Biomech (Bristol, Avon). 2008;23:450–458.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664996/?tool=pubmed
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimot. Page 12 of 13
69. Rocchi L, Chiari L, Mancini M, et al. Step initiation in Parkinson's disease: influence of initial stance conditions. Neurosci Let.
70. Mak MK, Patla A, Hui-Chan C. Sudden turn during walking is impaired in people with Parkinson's disease. Exp Brain Res.
71. Pfann KD, Buchman AS, Comella CL, Corcos DM. Control of movement distance in Parkinson's disease. Mov Disord.
72. Farley BG, Sherman S, Koshland GF. Shoulder muscle activity in Parkinson's disease during multijoint arm movements
across a range of speeds. Exp Brain Res. 2004;154:160–175. [PubMed]
73. Glendinning DS, Enoka RM. Motor unit behavior in Parkinson's disease. Phys Ther. 1994;74:61–70. [PubMed]
74. Salenius S, Avikainen S, Kaakkola S, et al. Defective cortical drive to muscles in Parkinson's disease and its improvements
with levadopa. Brain. 2002;125:491–500. [PubMed]
75. Yanagawa S, Shindo M, Yanagisawa N. Muscular Weakness in Parkinson's Disease. Vol. 53. NewYork, NY: Raven Press;
76. Giladi N, Kao R, Fahn S. Freezing phenomenon in patients with parkinsonian syndromes. Mov Disord. 1997;12:302–305.
77. Bloem BR, Hausdorff JM, Visser JE, Giladi N. Falls and freezing of gait in Parkinson's disease: a review of two
interconnected, episodic phenomena. Mov Disord. 2004;19:871–884. [PubMed]
78. Giladi N, McDermott MP, Fahn S, et al. Freezing of gait in PD: prospective assessment in the DATATOP cohort. Neurology.
79. Giladi N, Hausdorff JM. The role of mental function in the pathogenesis of freezing of gait in Parkinson's disease. J Neurol 80. Jacobs JV, Horak FB. External postural perturbations induce multiple anticipatory postural adjustments when subjects cannot
pre-select their stepping foot. Exp Brain Res. 2007;179:29–42. [PubMed]
81. Chong RKY, Jones CL, Horak FB. Postural set for balance control is normal in Alzheimer's but not in Parkinson's Disease. J Gerontol A Biol Sci med Sci. 1999;54:M129–M135. [PubMed]
82. Tunik E, Feldman AG, Poizner H. Dopamine replacement therapy does not restore the ability of Parkinsonian patients to
make rapid adjustments in motor strategies according to changing sensorimotor contexts. Parkinsonism Relat Disord.
2007;13:425–433. [PMC free article] [PubMed]
83. Horak FB, Nutt JG, Nashner LM. Postural inflexibility in parkinsonian subjects. J Neurol Sci. 1992;111:46–58. [PubMed]
84. Steiger MJ, Thompson PD, Marsden CD. Disordered axial movement in Parkinson's disease. J Neurol Neurosurg Psychiatry.
1996;61:645–648. [PMC free article] [PubMed]
85. Brown RG, Marsden CD. Dual-task performance and processing resources in normal subjects and patients with Parkinson's
disease. Brain. 1991;114(pt 1A):215–231. [PubMed]
86. Bloem BR, Grimbergen YA, van Dijk JG, Munneke M. The “posture second” strategy: a review of wrong priorities in
Parkinson's disease. J Neurol Sci. 2006;248:196–204. [PubMed]
87. DeLong MR. The neurophysiologic basis of abnormal movement in basal ganglia disorders. Neurobehav Toxicol Teratol.
88. Lidsky T, Manetto C, Schneider J. A consideration of sensory factors involved in motor functions of the basal ganglia. Brain 89. Snider SR, Isgreen WP, Cote LJ. Primary sensory systems in Parkinsonism. Neurology. 1976;26:423–429. [PubMed]
90. Diamond SG, Schneider JS, Markham CH. Oral sensorimotor defects in patients with Parkinson's disease. Adv Neurol.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664996/?tool=pubmed
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimot. Page 13 of 13
91. Jobst EE, Melnick ME, Byl NN, et al. Sensory perception in Parkinson's disease. Arch Neurol. 1997;54:450–454. [PubMed]
92. Zia S, Cody FWJ, O'Boyle DJ. Disturbance of human joint position sense in Parkinson's disease. J Physiol. 1997;504:117–
93. Zia S, Cody FWJ, O'Boyle DJ. Impairment of discrimination of bilateral differences in the loci of tactile stimuli in Parkinson's
disease. J Physiol. 1998;509:180–181. 94. Klockgether T, Borutta M, Rapp H, et al. A defect of kinesthesia in Parkinson's disease. Mov Disord. 1995;10:460–465.
95. O'Sullivan SB, Schmitz TJ. Physical Rehabilitation: Assessment and Treatment. Philadelphia: FA Davis Company; 1994. 96. Lundin-Olsson L, Nyberg L, Gustafson Y. “Stops walking when talking” as a predictor of falls in elderly people. Lancet.
97. Marchese R, Bove M, Abbruzzese G. Effect of cognitive and motor tasks on postural stability in Parkinson's disease: a
posturographic study. Mov Disord. 2003;18:652–658. [PubMed]
Articles from Physical Therapy are provided here courtesy of
American Physical Therapy Association
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664996/?tool=pubmed
East Denver Orthodox Synagogue Rabbi Daniel Rapp 198 S. Holly St., Denver, CO 80246 President, Michael Wolfe 303-322-7943 Gabbai, Shlomo Fried Wednesday Thursday Readings EDOS Classes This Week e extend a warm welcome to everyone who is We hope everyone enjoys our Carlebach davening Thank You Thank you to those providing Divrei Torah this week! These include Rabb
TROPICAL STORM ISAAC STILL LEAVES RISK IN ITS WAKE TAKE PRECAUTIONS TO AVOID MOSQUITO BITES! PALM BEACH COUNTY, FL –Palm Beach County has experienced heavy rainfall as a result of Tropical Storm Isaac which could signal an increase in mosquito activity. The Palm Beach County Health Department is urging residents to avoid being bitten by mosquitoes and prevent mosquito-borne illness. Pr









 Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 1 of 13
Phys Ther. 2009 April; 89(4): 384–393.
Copyright 2009, American Physical Therapy Association
Delaying Mobility Disability in People With Parkinson Disease Using a
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 1 of 13
Phys Ther. 2009 April; 89(4): 384–393.
Copyright 2009, American Physical Therapy Association
Delaying Mobility Disability in People With Parkinson Disease Using a 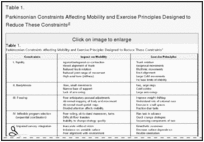 Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 3 of 13
Drive Neuroplasticity With Task-Specific Agility Exercise
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 3 of 13
Drive Neuroplasticity With Task-Specific Agility Exercise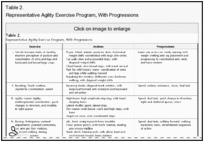
 Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 4 of 13
movement during postural transitions and gait.56,61 Electromyography studies have shown that people
with PD have high tonic background activity, especially in the flexors, and co-contraction of muscles
during movement, especially in the axial muscles.56,57 In addition, antagonist muscle activation is larger
and earlier, resulting in coactivation of muscle groups during automatic postural responses.61
Another characteristic of parkinsonian rigidity is axial rigidity, which results in a loss of natural vertebral,
pelvis/shoulder girdle, and femur/pelvis flexibility and range of motion that accompanies efficient
postural and locomotor activities.60,62 Wright et al55 found that rigidity in the neck, torso, and hips of
standing subjects was 3 to 5 times greater in subjects with PD than in age-matched control subjects
when measuring the torsional resistance to passive movement along the longitudinal axis during
twisting movements. Levodopa medication did not improve their axial rigidity.55 The high axial tone
(velocity-dependent resistance to stretch) in patients with PD contributes to their characteristic “en bloc”
trunk motions, which make it difficult for them to perform activities such as rolling over in bed or turning
Schenkman et al63 showed that exercise can increase trunk flexibility in people with PD. We propose an
agility program that includes movements that minimize agonist-antagonist muscle co-contraction (ie,
reciprocal movements), promote axial rotation, lengthen the flexor muscles, and strengthen the
extensor muscles to promote an erect posture. Rigidity can potentially be addressed with kayaking, an
exercise in which the person counter-rotates the shoulder and pelvic girdle; tai chi, a set of exercises
that focuses on the individual's awareness of postural alignment during postural transitions; and pre-
Pilates, a series of exercises aimed at increasing spinal mobility and lengthening flexor muscles
groups. In addition, the program should include strategies for turning and transitioning from a standing
position to sitting on the floor and back again that emphasize trunk and head rotation (Tabs. 2 and 3
Representative Agility Exercise Program, With Progressions
Bradykinesia
Delaying Mobility Disability in People With Parkinson Disease Using a Sensorimotor . Page 4 of 13
movement during postural transitions and gait.56,61 Electromyography studies have shown that people
with PD have high tonic background activity, especially in the flexors, and co-contraction of muscles
during movement, especially in the axial muscles.56,57 In addition, antagonist muscle activation is larger
and earlier, resulting in coactivation of muscle groups during automatic postural responses.61
Another characteristic of parkinsonian rigidity is axial rigidity, which results in a loss of natural vertebral,
pelvis/shoulder girdle, and femur/pelvis flexibility and range of motion that accompanies efficient
postural and locomotor activities.60,62 Wright et al55 found that rigidity in the neck, torso, and hips of
standing subjects was 3 to 5 times greater in subjects with PD than in age-matched control subjects
when measuring the torsional resistance to passive movement along the longitudinal axis during
twisting movements. Levodopa medication did not improve their axial rigidity.55 The high axial tone
(velocity-dependent resistance to stretch) in patients with PD contributes to their characteristic “en bloc”
trunk motions, which make it difficult for them to perform activities such as rolling over in bed or turning
Schenkman et al63 showed that exercise can increase trunk flexibility in people with PD. We propose an
agility program that includes movements that minimize agonist-antagonist muscle co-contraction (ie,
reciprocal movements), promote axial rotation, lengthen the flexor muscles, and strengthen the
extensor muscles to promote an erect posture. Rigidity can potentially be addressed with kayaking, an
exercise in which the person counter-rotates the shoulder and pelvic girdle; tai chi, a set of exercises
that focuses on the individual's awareness of postural alignment during postural transitions; and pre-
Pilates, a series of exercises aimed at increasing spinal mobility and lengthening flexor muscles
groups. In addition, the program should include strategies for turning and transitioning from a standing
position to sitting on the floor and back again that emphasize trunk and head rotation (Tabs. 2 and 3
Representative Agility Exercise Program, With Progressions
Bradykinesia