Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Untitled
Liver - 03327 Original Paper Immune-related Effects of Local Hyperthermia in Patients with Primary Liver Cancer Valentina V Ostapenko1, Hiroto Tanaka2, Motoshige Miyano1, Takahiro Nishide1, Hiroki Ueda2 Iwao Nishide1, Yoshimasa Tanaka1, Masatoshi Mune2, Susumu Yukawa2
1Shouseikai Nishide Hospital, and 2Third Department of Internal Medicine
Corresponding Author: Dr. Valentina Ostapenko, Shouseikai Nishide Hospital
Tel: +81 724 32 0777, Fax: +81 724 36 3074, E-mail: [email protected]KEY WORDS: ABSTRACT Background/Aims: To investigate immune-related
decreased significantly (p<0.05), whereas the rela-
effects of local hyperthermia (HT) with hepatocellu-
tive amount of CD4+ T cells showed a tendency to
decrease (p=0.063), and CD8 - to increase (p=0.088). Methodology: Immune status after 7 HT was stud-
An activation of NK cells was observed in patients
ied in 11 patients (M/F - 9/2; 1st group). The effects
who had a low or normal pretreatment level of acti-
were also evaluated during one HT session in 4 of
vation. In the 2nd group, there was a significant
ABBREVIATIONS:
decrease in the CD4/CD8 ratio by the end of the
The HT treatment was performed by means of an 8-
treatment (p<0.05) and increased activity of NK
MHz capacitive heating device, Thermotron RF8
cells as early as 20 min after the onset of HT
(Japan). The mean time of one HT session was 60
min. HT was performed 1-2 times a week. In both
Conclusions: Our results suggest that HT stimu-
groups the percentage of T and B cells, CD4+, CD8+
lates the immunity of cancer patients by several
subsets of T cells, the CD4/CD8 ratio and activation
means and therefore may exhibit indirect anticancer
effect. In addition, activation of NK cells by HT may
Results: In the 1st group, CD4/CD8 ratio was be associated with improved quality of life. INTRODUCTION Heating: The HT treatment was performed by
The rate of hepatocellular carcinoma (HCC) has
means of an 8-MHz capacitive heating device, "Ther-
been increasing in Japan. Most cases are associated
motron RF-8" (Yamamoto Vinita Co., Ltd., Osaka,
with HCV infection. The mechanism of HCV-related
Japan). The electromagnetic power ranging from 614
carcinogenesis and disease progression are not well
to 1363 W was applied between two 30-cm electrodes
understood, although it is thought that not only virus-
placed on opposite sides of the patient's upper abdom-
induced but also immunologically mediated mecha-
inal region. Overlying water boluses were placed
between the electrode and the skin to improve the
Such local methods as transcatheter arterial
homogeneity of the heating. A saline solution main-
embolization (TAE) and percutaneous ethanol injec-
tained at 2-15°C was circulated in the boluses to avoid
tion therapy (PEIT) are widely used in the treatment
overheating of the skin. For premedication, 50mg
of inoperable HCC. However, it has been reported that
indomethacin (i.r.) was administered 30 min before
the TAE procedure might suppress a host immunity
HT. A 1% xylocaine topical gel was applied to the skin
response against cancer in HCC patients (3). Recently
to decrease the sensation of heat. Blood pressure and
local hyperthermia (HT) has been widely used for can-
pulse were monitored during treatment. The time of
cer treatment as a way to increase a tumor's radio-
one HT session was 40-60 min. HT was performed 1-2
and chemosensitivity (4,5). In contrast to most other
times a week. A total of 8 sessions delivered 1-2 times
cancer treatment modalities, HT is also known to
a week, were performed (1 course). Thermometry was
cause an activation of the immune system (6-10).
In this study, the potential of local HT to enhance
Laboratory data: In the first group (N=11), the
the cell-mediated immunity of HCC patients was
percentage of T and B cells, CD4+ and CD8+ subsets,
the CD4/CD8 ratio and activation of natural killer(NK) cells were evaluated before the 1st and 8th ses-
METHODOLOGY
sions. In the 2nd group (N=4) the same immune para-
Patients' characteristics: Clinical characteris-
meters were investigated during one 60-minute HT
tics are summarized in Table 1.
session, namely, before the onset of heating, 20 and 40
Hepato-Gastroenterology 2005; 52:1502-1506 H.G.E. Update Medical Publishing S.A., Athens-Stuttgart
Hyperthermia and Immunity in Liver Cancer
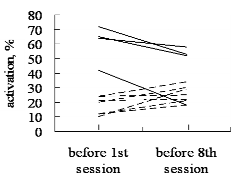
Combination FIGURE 1 NK cells activation in the course of HT in regards to Previous
pretreatment level. Normal values of activation of NK cells are 18-40%. Solid lines indicate data for patients with pretreatment level of activationexceeding normal range. Dashed lines indicate data for patients with
pretreatment level being lower or within normal range.
ation therapy; PEIT: percutaneous ethanol injection
Ascitis treatment
min after onset of heating and immediately after its
All patients were informed about the nature and
Statistics: Data were evaluated using a paired t-
test. p values <0.05 were considered as statistically
RESULTS The Effect of Seven HT Sessions on Cell- mediated Immunity
Data are summarized in Table 2. As shown, the
CD4+/CD8+ T cell ratio was significantly decreased by HT (p=0.05) (Table 1). This effect was associated
to a higher degree with decreased amount of CD4+
PIVKA-II,
cells and to a lower degree with increased amount ofCD8+ T cells (NS). The percentage of the total popu-lation of both T and B cells, as well as activation of NK
cells, did not significantly change in these series. At
the same time, we found that the pattern of activationof NK cells was likely to be dependent on its pretreat-ment status. Namely, for patients whose pretreat-
TABLE 1 Pretreatment Characteristics of the Patients and Parameters of the HT
ment level of NK activation was below or within the
Location
normal value, there was a significant additional acti-
TB: total bilirubin; Alb: albumin; PLT: platelets; TAE: transarterial emboliz
vation caused by HT treatment (15.3±6.7% to 24.3±6.3%, p<0.05) (Figure 1). On the contrary, for
those who demonstrated an increased pretreatmentactivation level, HT treatment resulted in a decreaseor lack of change of that parameter (60.8±12.9% to
45.3±18.4, NS) (Figure 1). The Effect of a Single HT Session on Cell- mediated Immunity
Corresponding data are summarized in Table 3.
The CD4/CD8 ratio showed a tendency to begin
decreasing already at 20 min of heating, demonstratea significantly low value at 40 min of heating and
lower further by the end of HT. The decrease in theCD4/CD8 ratio was mostly due to the decrease inCD4+ fraction and less due to the tendency for CD8+
Notes: Group 2 consisted of cases 1, 5, 10 and 11.
cells to increase. The total amount of T and B cells did
VV Ostapenko, H Tanaka, M Miyano, et al. TABLE 2 Immune Parameters in the Course of HT Treatment CD4/ CD8,% T cells, % B cells, % NK activation, % TABLE 3 Immune Parameters in HCC Patients during a Single HT Session CD4/ CD8, % T cells, % B cells, % NK activation, %
not change during the treatment. A significant NK
ing is beneficial because of its activation of immune
activation was evident as early as 20 min after the
responses. Various immune-related effects of local HT
onset of treatment, and continued to increase up to
can be expected, as it has already been shown in
numerous experimental and clinical investigations. Among the clinically most relevant aspects of cell-
DISCUSSION
mediated immunity are CD4+ and CD8+ populations
Both carcinogenesis and tumor progression are
of T cells, the CD4/CD8 ratio, T and B cells, and NK
associated with a depressed immune status of the
cell activity. Therefore, these parameters were chosen
host. It has been suggested that a decrease of CD56+
cells and NK cells in cirrhotic livers caused by hepati-
In the clinic, both CD4+ and CD8+ T cells were
tis C is related to susceptibility to HCC (11,12).
shown to play an important role in antitumor defense,
Depressed NK activity was also noted in patients with
although the relative clinical significance of each sub-
HCC, cancers of the kidney and urinary bladder
set might depend on the tumor type. Stawarz et al.
have shown an increase of the CD4/CD8 ratio by local
In the multimodality treatment of cancer, a local
HT in patients with advanced adenocarcinoma of the
HT has been demonstrated to potentiate radiothera-
prostate (10). In contrast, we found a decrease in the
py, some chemotherapies, and immunotherapy (15-
CD4/CD8 ratio, which was mainly due to the increase
17). Employment of HT in combination with other
in the fraction of CD8+ cells. Taking into account
modalities used in mild regimens has also been report-
other data for ovarian cancer patients, where a
ed. In treatment of HCC, the combination of HT with
decrease of CD8+ lymphocytes was shown to correlate
TAE and PEIT was found to be effective (18,19).
with the progression of the disease (26), we consider
Moreover, HT alone has also been reported to effec-
the changes observed by us as favorable ones. Inter-
estingly, HT-induced changes in CD4+, CD8+ subsets
It has been well established that immunocompe-
were found in both groups, demonstrating some simi-
tent cells, including macrophages, T-lymphocytes and
larity in early and late effects of HT. Therefore, there
natural killer (NK) cells, in vitro, are among the most
was probably both a direct activation of immunocom-
sensitive cells to temperature elevation (22,23). There-
petent cells by elevated temperature, and an indirect
fore, both whole-body and local HT may cause favor-
one, mediated by HT-induced heat-shock proteins, as
able immune changes when employed in cancer clinic.
follows from recent knowledge of the mechanisms of
HT-related immune effects were found to depend on a
heating regimen. For instance, temperature ranging
A significant increase of NK cytolytic activity was
from 39 to 41°C (fever range) was shown to confer an
noted following transrectal HT of prostate, with the
immunoregulatory advantage by enhancing the secre-
peak effect at 2 months and a subsequent decrease
tion of immunoglobulins, whereas elevation of tem-
(27). In our series, there was a selective increase of NK
perature to tumoricidal level (>42°C) led to inhibition
activation in patients whose pretreatment values were
of host competence (24,25). Therefore, a whole-body
lower or within normal range. These data fit the state-
HT, if used at tumoricidal temperature, may probably
ment of Rosberger et al., who noticed not only
cause unfavorable immune response. In the case of
immunostimulation but also an immunomodulatory
local HT, even if temperature in the tumor exceeds
effect of local HT in patients with choroidal
42°C, the surrounding normal tissue usually remain
melanoma. They showed that local HT inverted
at fever-range temperatures. This selectivity of heat-
CD4/CD8 resulting in a normalization of T-cell subset
Hyperthermia and Immunity in Liver Cancer
ratios (28). In our investigation, where the affects of
whom quality of life was demonstrated to improve by
HT on a group of patients were studied during one 60-
HT had also demonstrated remarkable activation of
min HT session (second group), we found that NK
NK cells in the course of one HT session. In contrast,
cells responded first to the local heating of the liver
those who failed to recover QOL had little change in
and showed a significant increase in activation already
NK activity (data not shown). We have a special inter-
at 20 min after the beginning of the treatment.
est to continue research in this field having being
It was demonstrated previously that HT-related
encouraged by previous finding by others that NK
effects may also be an important step in anticancer
activity in patients with anxiety about cancer was sig-
defense as augmented immune cell traffic and its
nificantly lower than that in those with no such anxi-
enhanced responsiveness and stimulatory activity,
shown in healthy volunteer study where skin was
In conclusion, local HT stimulates cell-mediated
heated in a water bath of 44°C for 3 h (6). As shown in
host immunity, involving both innate responses such
vivo for murine melanoma, local HT (43°C, 15 min)
as NK cell activation, and adopted responses, such as
induced infiltration of NK cells into the tumor (29). In
change in CD4+, CD8+ subsets. These effects take
patients with esophageal cancer, infiltration of lym-
place as early as during the HT treatment and remain
phocytes (IL) appeared to be a prognostic predictor
through the 7-session treatment schedule, lasting up
after preoperative chemoradiotherapy, while in addi-
to 2 months. NK cells respond first to the elevation of
tion, simultaneous HT significantly stimulated IL
temperature of the lower abdomen, including the
liver. However, a larger study is warranted in order to
In addition to the above-mentioned properties of
exclude the influence of such parameters as age, sex,
NK cells, we have noticed that its activity may be asso-
drug administration, and psycho-emotional condi-
ciated with quality of life. Thus, those patients in
REFERENCES 1 Cerny A, Chisari FV: Immunological aspects of HCV
involved in their susceptibility to hepatocellular carcinoma.
infection. Intervirology 1994; 37(2):119-125. 2 Chuang WL, Liu HW, Chang WY: Natural killer cell 12 Seki T, Nonaka T, Kubota Y, Mizuno T, Sameshima
activity in patients with hepatocellular carcinoma relative
Y: Ultrasonically guided percutaneous ethanol injection
to early development and tumor invasion. Cancer 1990;
therapy for hepatocellular carcinoma. Am J Gastroenterol
3 Komiyama 13 Morales A, Ottenhof PC: Clinical application of a whole
in HCC patients treated with transcatheter arterial
blood assay for human natural killer (NK) cell activity. Can-
embolization (TAE). Nippon Shokakibyo Gakkai Zasshi
14 Son K, Kew M, Rabson AR: Depressed natural killer cell 4 Matsuda T, Shimoyama T, Ohno T, Maeta M, Taka-
activity in patients with hepatocellular carcinoma. Cancer
hashi M, Tsukiyama I, Doi O, Uehara S: Local hyper-
thermia combined with chemotherapy for solid tumors:
15 Seong JS, Han EK, Han KH, Noh SH, Park CI, Loh
Analysis of joint research conducted at a number of institu-
JJ, Choi HJ: Histological studies of surgically resected
tions in Japan. In: Matsuda T (Ed.). Cancer Treatment by
hepatocellular carcinoma following combined radiotherapy
Hyperthermia, Radiation and Drugs. London: Taylor &
and hyperthermia. Yonsei Med J 1991; 32(2):147-156. 16 Kondo M, Itani K, Yoshikawa T, Tanaka Y, Watanabe 5 van der Zee J, Gonzalez Gonzalez D, van Rhoon GC, N, Hiraoka M, Noguchi M, Miura K: A prospective ran- van Dijk JD, van Putten WL, Hart AA: Comparison of
domized clinical trial comparing intra-arterial chemothera-
radiotherapy alone with radiotherapy plus hyperthermia in
py alone and in combination with hyperthermia for
locally advanced pelvic tumours: a prospective, randomised,
metastatic liver cancer. Gan to Kagaku Ryoho 1995;
multicentre trial. Dutch Deep Hyperthermia Group. Lancet
17 Maeda M, Watanabe N, Yamauchi N, Tsuji Y, Niitsu 6 Olszewski WL, Grzelak I, Ziolkowska A, Engeset A: Y: Successful treatment of a case of hepatocellular carcino-
Effect of local hyperthermia on lymph immune cells and
ma with tumor necrosis factor and local hyperthermia. Gas-
lymphokines of normal human skin. J Surg Oncol 1989;
18 Yumoto Y, Jinno K, Tokuyama K, Wada T, Kobayashi 7 Kappel M, Stadeager C, Tvede N, Galbo H, Pedersen H, Okamoto T, Toki H, Inatsuki S, Hara K, Moriwaki BK: Effects of in vivo hyperthermia on natural killer activ- S, Tuji T, Maeda H: Transcatheter hepatic arterial injec-
ity, in vitro proliferative responses and blood mononuclear
tion of lipiodol soluble anti-cancer agent SMANCS and ADR
cell subpopulations. Clin exp Immunol 1991; 84:175-180.
suspension in lipiodol combined with arterial embolization
8 Downing JF, Taylor MW: The effect of in vivo hyper-
and local hyperthermia for treatment of hepatocellular car-
thermia on selected lymphokines in man. Lymphokine Res
cinoma. Int J Hyperthermia 1991; 7(1):7-17. 19 Tanaka H, Ostapenko VV, Miyano M, Nishide T, 9 Zanker KS, Lange J: Whole body hyperthermia and nat- Sonobe M, Toda K, Nishide I, Mune M, Yukawa S:
ural killer cell activity. Lancet 1982; 1(8280):1079-1080.
Successful treatment of hepatocellular carcinoma with per-
10 Stawarz B, Zielinski H, Szmigielski S, Rappaport E,
cutaneous ethanol injection therapy and local hyperther-
Debicki P, Petrovich Z: Transrectal hyperthermia as pal-
mia. Hepatogastroenterology 2002; 49:1666-1668.
liative treatment for advanced adenocarcinoma of prostate
20 Nagata Y, Hiraoka M, Nishimura Y, Masunaga S,
and studies of cell-mediated immunity. Urology 1993;
Mitumori M, Okuno Y, Fujishiro M, Kanamori S, Horii N, Akuta K, Sasai K, Abe M, Fukuda Y: Clinical 11 Kawarabayashi N, Seki S, Hatsuse K, Ohkawa T,
results of radiofrequency hyperthermia for malignant liver
Koike Y, Aihara T, Habu Y, Nakagawa R, Ami K,
tumors. Int J Radiat Oncol Biol Phys 1997; 38(2):359-365. Hiraide H, Mochizuki H: Decrease of CD56(+)T cells and 21 Hager ED, Dziambor H, Hohmann D, Gallenbeck D,
natural killer cells in cirrhotic livers with hepatitis C may be
Stephan M, Popa C: Deep hyperthermia with radiofre-
VV Ostapenko, H Tanaka, M Miyano, et al.
quencies in patients with liver metastases from colorectal
thermia on human NK and T cell function. Int J Hyper-
cancer. Anticancer Res 1999; 19:3403-3408. 22 Szmigielski S, Janiak M: Reaction of cell-mediated 28 Rosberger DF, Coleman DJ, Silverman R, Woods S,
immunity to local hyperthermia of tumors and its potentia-
Rondeau M, Cunningham-Rundles S: Immunomodula-
tion by immunostimulation. Baltimore, Munich: Urban &
tion in choroidal melanoma: reversal of inverted CD4/CD8
ratios following treatment with ultrasonic hyperthermia. 23 Yoshioka A, Miyachi Y, Imamura S: Immunological
effects of in vitro hyperthermia. Journal of Clin and Lab
29 Nakayama J, Toyofuku K, Urabe A, Taniguchi S, Hori Y: A combined therapeutic modality with hyperther- 24 Huang YH, Haegerstrand A, Frostegard J: Effects of in
mia and locally administered rIFN-beta inhibited the
vitro hyperthermia on proliferative responses and lympho-
growth of B16 melanoma in association with the modulation
cyte activity. Clin Exp Immunol 1996; 103:61-66.
of cellular infiltrates. J Dermatol Sci 1993; 6: 240-246. 25 Shen R-N, Lu L, Young P, Shidnia H, Hornback NB, 30 Morita M, Kuwano H, Araki K, Egashira A, Broxmeyer HE: Influence of elevated temperature on nat- Kawaguchi H, Saeki H, Kitamura K, Ohno S, Sugi-
ural killer cell activity, lymphocyte-activated killer cell activ-
machi K: Prognostic significance of lymphocyte infiltration
ity and lectin-dependent cytotoxicity of human umbilical
following preoperative chemoradiotherapy and hyperther-
cord blood and adult blood cells. Int J Radiation Oncol Biol
mia for esophageal cancer. Int J Radiat Oncol Biol Phys
26 Markowska J, Lacki JK, Jaroszewski J, Wiktorowicz 31 Koga C, Itoh K, Aoki M, Suefuji Y, Yoshida M, Asosi- K: The usefulness of CD4/CD8 evaluation in monitoring of na S, Esaki K, Kameyama T: Anxiety and pain suppress
ovarian cancer patients. Eur J Oncol 1995; 16(1):54-58.
the natural killer cell activity in oral surgery outpatients. 27 Szmigielski S, Sobczynski J, Sokolska G, Stawarz B,
Oral Surg Oral Med Pathol Oral Radiol Endod 2001; 91 (6):
Zielinski H, Petrovich Z: Effect of local prostatic hyper-
Lila L. Schmidt, MD OB/GYN, Reproductive Endocrinology/Infertility 3969 4th Avenue, Suite 207 San Diego, CA 92103 619/295-4050 SanDiegoMommyMaker.com EMBRYO TRANSFER Procedures, Instructions and Expectations How is the embryo transfer performed? A speculum is placed in the vagina to provide access to your cervix, much like the way it is during your annual pap s
MEDICATION GUIDE NEXIUM (nex-e-um) (esomeprazole magnesium) Delayed-Release Capsules NEXIUM (nex-e-um) (esomeprazole magnesium) For Delayed-Release Oral Suspension Read the Medication Guide that comes with NEXIUM before you start taking NEXIUM and each time you get a refill. There may be new information. This information does not take the place of talking with you
 Hyperthermia and Immunity in Liver Cancer
Combination
Hyperthermia and Immunity in Liver Cancer
Combination