Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Bowel management
Bowel Management
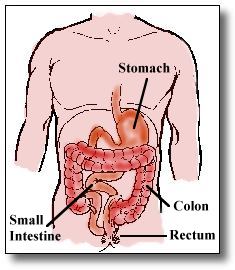
The purpose of the bowel is to absorb food to supply energy to
your body and eliminate waste matter. Your stomach prepares food for digestion, the small bowel absorbs the food your body needs, and the remaining waste matter passes into the large bowel, or colon, where extra water is removed.
Food and waste matter is propelled along the small and large bowel by a wave like contraction called peristalsis. Normally, peristalsis increases about 15 to 30 minutes after you eat a large
meal. This is called the gastrocolic reflex. When the stool reaches the end of the large bowel, the walls of the rectum stretch, which sends a message along the nervous system to the spinal cord which in turn sends a message back to the bowel to increase peristalsis and relax the anal sphincter muscle. The
brain also receives a message so that you know that you need to have a bowel movement. Your brain can voluntarily control the sphincter muscle until you are ready.
A spinal cord injury affects the voluntary control of bowel movements. Part of your rehabilitation is training your bowel movements to be regular and reliable.
The bowel program must begin with an empty bowel. This is usually done by taking one to four Senokot tablets six to eight hours prior to inserting a Bisacodyl suppository. Senokot is used because it is a gentle, natural stimulant and because it works only on the large intestine. Bisacodyl suppositories stimulate nerves in your large bowel to increase peristalsis and result in a bowel movement. After your bowel is empty, you will begin your bowel program.
The first step to a regular and reliable bowel program is timing. While
in the hospital we start you on an evening program so it will not interfere with your therapies. This means you will take your Senokot at noon followed by a suppository in the evening. You may consider using the gastrocolic reflex when planning your bowel program. This means that you would eat a meal or snack 15 to 30 minutes before you insert your suppository to try to stimulate the gastrocolic reflex.
Suppository Insertion
• Lie in bed on your left side • Open the Bisacodyl suppository. If you are using a Supp-a-sert, place the suppository in the
• Lubricate the tip of the suppository with a water-soluble lubricant such as K-Y jelly. Do NOT
use petroleum jelly (Vaseline). If K-Y jelly is not available, moisten the rectal area with tap water.
• Because you cannot see or feel the area around the rectal opening, you may find it easier to
place the tip of the suppository at the top of the buttock crease and slowly slide it toward the
rectal opening with gentle pressure. When you get to the rectal opening, the suppository should slide right in. You may also want to use a para mirror. When using a Supp-a-sert you will need to insert until the spring is fully compressed to allow adequate insertion of the suppository. The suppository must be inserted about one inch in adults.
After you have inserted your suppository, remain in this position for 15 minutes, and then transfer to
a commode chair. Sitting is the most natural position for bowel movements because gravity helps empty your bowel. A padded commode chair should be used to help avoid pressure sores.
If you have not had a bowel movement after 5 to10 minutes, stimulate peristalsis by inserting a lubricated gloved finger in to the rectum and gently rotating your finger. This will also help relax the anal sphincter muscle. This is called digital stimulation
and can be repeated as necessary at 5 to10 minute intervals. If you have limited hand function you may be able to use a Dig-i-stim. This is a device that will help you gain independence with your bowel program. Your nurse will help you learn how to use both the Supp-a-sert and Dig-i-stim.
If you have only a small bowel movement or perhaps none at all, you need to repeat your bowel program the following day. If you still have no results, drink more fluids, eat fresh fruits and vegetables, increase senokot tablets and repeat suppository until you have good results.
Remember:
Establish the same time to take your Senokot followed by a Bisacodyl suppository 6 to8 hours later. Use the sitting position and digital stimulation
Additional medications you may use:
Colace a stool softener used to prevent hard stool;
Metamucil or Citrucel, are medicines that contains fiber which absorbs water and promotes soft, easier-to-pass stool;
Fleets (Bisacodyl) or Theravac (Docusate) are liquid suppositories that work faster but are more expensive.
Learn how your bowel medication works and how to adjust the dosage if problems occur.
Understanding what your bowel habits were like before your injury will help you adjust your bowel
program. Questions like, "How often?", "How much?", and "What time?" will help decide whether your program should allow for bowel movements every day or every other day. The time of day is important, too. Although we recommend evenings for bowel programs, it might not be right for you if you have always had bowel movements in the morning. Other questions, such as "Were your bowel movements hard or soft?" or "Do some foods cause you to have diarrhea or constipation?" will
help you determine if your bowel program is effective and help identify foods or liquids you may want to use in small amounts or avoid completely.
Be aware that if emotional upsets affected your bowel movements before your injury, it may still occur even though you have a regulated bowel program.
Other factors that will influence your bowel regularity are nutrition and exercise. You should have well balanced meals that include roughage (fresh raw fruits and vegetables, whole grain breads and cereals) and fluids. These produce well-formed stool - not too hard, not too soft. Exercise and normal activities, like dressing and transfers, will help you maintain an active, rather than sluggish, bowel.
Factors that may change your bowel routine
Problems you may have with your bowel do not differ greatly from those experienced by people in the general population.
d by intolerance of foods, taking certain medications (like antibiotics), over-medication with Senokot, or perhaps even the presence of a virus. If you have diarrhea, stop taking Senokot and suppositories until the diarrhea stops, try to figure out the cause (stop eating the irritating food or change antibiotics), and then resume your usual routine.
Constipation occurs when the stool is allowed to remain in the bowel for an extended time resulting in absorption of too much water. You may experience poor appetite, a bloated stomach, and nervousness. If constipation continues, it can lead to an impaction.
An impaction means that the stool is stuck in the rectum. Although liquid stool may leak around the impaction, it should not be confused with diarrhea! The difference is that you probably will not have had good results from your bowel program several times in a row.
An impaction is a serious condition: if not removed, it can lead to a bowel obstruction and require surgical correction.
To remove an impaction, lubricate a gloved finger and insert it into the rectum. If you can feel the
hardened mass of stool, try to break it up and remove it with your finger. If the stool cannot be felt, you may need to increase your Senokot dosage or use a stool softener (like Colace) and increase your fluid intake. You may also eat prunes or other foods that usually give you diarrhea.
Hemorrhoids are a swelling of the rectal veins and are caused by irritation. They are the most frequent cause of minor rectal bleeding. It can be treated with local medication and stool softeners.
perienced by people who have spinal cord injuries above the sixth thoracic vertebrae. If a full bowel is the cause, the stool must be removed quickly and
gently. You follow the same procedure as you would to remove an impaction. One difference is that you may want to use and anesthetic lubricant such as Nupracainal ointment because the act of removing the stool may increase the symptoms of
autonomic hyperreflexia. If an anesthetic lubricant is not available, do not wait! It is important to remove the stool as gently and quickly as possible. Do not use enemas because they can stretch the bowel an lead once again to autonomic hyperreflexia.
Because there are so many factors involved in your bowel program, changes in medication, diet, or routine should be made one at a time. For example, if you develop problems with bowel accidents or
constipation, change only the food or fluid you think may be the cause of the problem. If you have have not found a solution within a week, call the outpatient nurse specialist at the University Hospital Rehabilitation Center. It is important to find a solution before a major problem develops.
A few more important points to remember about a bowel program:
• Never use a bedpan. It can produce pressure on areas
of skin where you do not have any feeling. This will lead to skin breakdown.
• Avoid routine use of enemas and harsh laxatives like
Ex-lax, Dulcolax tablets, or Magnesium Citrate unless otherwise instructed. They will stretch the bowel, cause loss of muscle tone, are less predictable, and are irritating to the bowel with long term use.
• If you are admitted to the hospital for diagnostic test,
check if they usually give enemas or harsh laxatives to clean the bowel prior to the test. If they do, ask your doctor if you could instead do your bowel program for three days in a row prior to the test. This will usually provide adequate cleansing of the bowel.
• If barium is used for a diagnostic test, be sure to do your bowel program daily until the stool
is a normal color and free of barium. This is very important because barium can harden and cause impactions.
In summary, a poorly managed bowel program can redirect the entire focus of your everyday routine. The goal of a successful bowel program is to have a regular, reliable, bowel movement with the minimum amount of time invested.
You should be knowledgeable about managing your bowel program. Ask questions, learn the principles, and work with the rehab team during your stay to set up a bowel program that works for
you. Remember, the effort you put into your bowel program will mean more time to do the things you enjoy and lead to a happier, healthier life.
In-Kind Assistance Received from Bilateral Sources 1/ 16 member Medical Team and Related SuppliesCoral reef assessment teamVolunteer teachers 2 Military aircrafts with relief supplies (mainly medicine & food)Maintenance Equipment & Personal LuggageBell x-212 Helicopter to join the relief team14 member crew (including pilots) of the Bell x-212 Helicopterground equipment maintaccessor
Norplant Qu’est-ce que c’est ? Le Norplant consiste en 6 bâtonnets de silastic (caoutchouc de silicone), chacun mesurant 3,4 cm de long et 2,4 mm de diamètre. Chaque bâtonnet est rempli d'une hormone appelée levonorgestrel, une progestérone de synthèse. Le levonorgestrel est libéré dans le sang dès que les bâtonnets sont insérés sous la peau du bras. Le Norplant est
 Bowel Management
Bowel Management 
 rectal opening with gentle pressure. When you get to the rectal opening, the suppository should slide right in. You may also want to use a para mirror. When using a Supp-a-sert you will need to insert until the spring is fully compressed to allow adequate insertion of the suppository. The suppository must be inserted about one inch in adults.
After you have inserted your suppository, remain in this position for 15 minutes, and then transfer to
a commode chair. Sitting is the most natural position for bowel movements because gravity helps empty your bowel. A padded commode chair should be used to help avoid pressure sores.
If you have not had a bowel movement after 5 to10 minutes, stimulate peristalsis by inserting a lubricated gloved finger in to the rectum and gently rotating your finger. This will also help relax the anal sphincter muscle. This is called digital stimulation
and can be repeated as necessary at 5 to10 minute intervals. If you have limited hand function you may be able to use a Dig-i-stim. This is a device that will help you gain independence with your bowel program. Your nurse will help you learn how to use both the Supp-a-sert and Dig-i-stim.
If you have only a small bowel movement or perhaps none at all, you need to repeat your bowel program the following day. If you still have no results, drink more fluids, eat fresh fruits and vegetables, increase senokot tablets and repeat suppository until you have good results.
Remember:
rectal opening with gentle pressure. When you get to the rectal opening, the suppository should slide right in. You may also want to use a para mirror. When using a Supp-a-sert you will need to insert until the spring is fully compressed to allow adequate insertion of the suppository. The suppository must be inserted about one inch in adults.
After you have inserted your suppository, remain in this position for 15 minutes, and then transfer to
a commode chair. Sitting is the most natural position for bowel movements because gravity helps empty your bowel. A padded commode chair should be used to help avoid pressure sores.
If you have not had a bowel movement after 5 to10 minutes, stimulate peristalsis by inserting a lubricated gloved finger in to the rectum and gently rotating your finger. This will also help relax the anal sphincter muscle. This is called digital stimulation
and can be repeated as necessary at 5 to10 minute intervals. If you have limited hand function you may be able to use a Dig-i-stim. This is a device that will help you gain independence with your bowel program. Your nurse will help you learn how to use both the Supp-a-sert and Dig-i-stim.
If you have only a small bowel movement or perhaps none at all, you need to repeat your bowel program the following day. If you still have no results, drink more fluids, eat fresh fruits and vegetables, increase senokot tablets and repeat suppository until you have good results.
Remember: 
 Be aware that if emotional upsets affected your bowel movements before your injury, it may still occur even though you have a regulated bowel program.
Other factors that will influence your bowel regularity are nutrition and exercise. You should have well balanced meals that include roughage (fresh raw fruits and vegetables, whole grain breads and cereals) and fluids. These produce well-formed stool - not too hard, not too soft. Exercise and normal activities, like dressing and transfers, will help you maintain an active, rather than sluggish, bowel.
Factors that may change your bowel routine
Be aware that if emotional upsets affected your bowel movements before your injury, it may still occur even though you have a regulated bowel program.
Other factors that will influence your bowel regularity are nutrition and exercise. You should have well balanced meals that include roughage (fresh raw fruits and vegetables, whole grain breads and cereals) and fluids. These produce well-formed stool - not too hard, not too soft. Exercise and normal activities, like dressing and transfers, will help you maintain an active, rather than sluggish, bowel.
Factors that may change your bowel routine  autonomic hyperreflexia. If an anesthetic lubricant is not available, do not wait! It is important to remove the stool as gently and quickly as possible. Do not use enemas because they can stretch the bowel an lead once again to autonomic hyperreflexia.
Because there are so many factors involved in your bowel program, changes in medication, diet, or routine should be made one at a time. For example, if you develop problems with bowel accidents or
constipation, change only the food or fluid you think may be the cause of the problem. If you have have not found a solution within a week, call the outpatient nurse specialist at the University Hospital Rehabilitation Center. It is important to find a solution before a major problem develops.
A few more important points to remember about a bowel program:
autonomic hyperreflexia. If an anesthetic lubricant is not available, do not wait! It is important to remove the stool as gently and quickly as possible. Do not use enemas because they can stretch the bowel an lead once again to autonomic hyperreflexia.
Because there are so many factors involved in your bowel program, changes in medication, diet, or routine should be made one at a time. For example, if you develop problems with bowel accidents or
constipation, change only the food or fluid you think may be the cause of the problem. If you have have not found a solution within a week, call the outpatient nurse specialist at the University Hospital Rehabilitation Center. It is important to find a solution before a major problem develops.
A few more important points to remember about a bowel program: