Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Swissroaccutaneaction.ch
Functional Brain Imaging Alterations in Acne Patients Treated With Isotretinoin J. Douglas Bremner, M.D. Objective: Although there have been
after 4 months of treatment with isotreti-
case reports suggesting a relationship be-
noin (N=13) or an antibiotic (N=15). Negar Fani, M.S. Results: Isotretinoin but not antibiotic Ali Ashraf, M.D.
depression and suicide, this topic remains
John R. Votaw, Ph.D.
brain metabolism in the orbitofrontal cor-
controversial. In order for isotretinoin to
Marijn E. Brummer, Ph.D. Thomas Cummins, M.D.
isotretinoin on brain functioning in acne
Viola Vaccarino, M.D., Ph.D.
no differences in the severity of depres-
purpose of this study was to assess the ef-
Mark M. Goodman, Ph.D.
fects of isotretinoin on brain functioning
and antibiotic treatment groups before or
Lai Reed, M.B.A. Sajid Siddiq, M.D. Method: Brain functioning in adults was Conclusions: This study suggests that
isotretinoin treatment is associated with
Charles B. Nemeroff, M.D., Ph.D. (Am J Psychiatry 2005; 162:983–991)
Isotretinoin (13-cis-retinoic acid) is a retinoid that in- concentration, tearfulness, psychotic symptoms, and
hibits sebaceous gland functioning, keratinization, and
guilty rumination (17–19) that resolved with discontinua-
inflammatory responses and is currently approved by the
tion of vitamin A. Among reports to the World Health Or-
Food and Drug Administration (FDA) for the treatment of
ganization and the FDA of adverse events associated with
cystic acne (1, 2). Isotretinoin has been prescribed to 2
acne treatments, adverse events related to depression and
million patients in the United States and over 8 million pa-
suicide have been more common with isotretinoin than
tients worldwide and is highly effective for acne. The exact
with other treatments for acne, such as antibiotics (4, 11).
mechanism of action of isotretinoin remains unknown.
The relationship between isotretinoin treatment and
In the last several years there has been controversy over
depression and suicide, however, remains controversial.
the possible role of isotretinoin in the development of de-
Although the manufacturer, on the basis of FDA guide-
pression and suicide (3–6). Case reports in the literature
lines, lists depression as a possible side effect, there is no
describe depression that developed in conjunction with
consensus on a causal role for isotretinoin in the develop-
isotretinoin treatment, resolved with discontinuation of
ment of depression and suicide. The high incidence of de-
the medication, and in some cases returned when the
pression in the general population makes it difficult to
medication was restarted (7–14). Estimates of the inci-
identify small increases specifically related to an addi-
dence of depression following treatment with isotretinoin
tional factor, such as isotretinoin administration. One
include 1% (14), 4% (15), and 6% (10). Other reports have
large epidemiological study did not demonstrate a signifi-
noted suicidality, behavioral disturbances, and psychotic-
cantly increased risk for suicide in patients treated with
type symptoms with isotretinoin treatment in addition to
isotretinoin (3). Some authors have argued that cases of
the typical symptoms of depression (8, 12). Isotretinoin ischemically similar to the retinoid vitamin A, a fat-soluble
depression associated with isotretinoin administration
vitamin stored in high concentrations in the liver. Vitamin
are merely coincidental (20) or that isotretinoin actually
A is converted after oxidation to retinoic acid, when it has
leads to an improvement in anxiety and depression be-
biological effects. Arctic explorers who fed on polar bear
cause of the clearing of disfiguring acne (21). Studies have
liver developed symptoms of confusion and psychosis.
shown an improvement in feelings of general well-being
Large doses of vitamin A can have a number of other neu-
or self-image (22, 23) or in feelings of anxiety (20, 24–28)
rological and mental effects, including fatigue, decreased
among patients with cystic acne following isotretinoin ad-
interest, headache, and diplopia (double vision) (16, 17).
ministration, although the findings were more directly re-
Published case reports of vitamin A toxicity include symp-
lated to improvement in measures of patient satisfaction,
toms of aggression, personality changes, depression, poor
rather than clinical symptoms of depression. ISOTRETINOIN AND BRAIN FUNCTIONING
To establish a causal role of isotretinoin in the develop-
2), and erythromycin (N=1). The subjects continued treatment
ment of depression and suicide, it is critical to establish a
until they completed the second PET scan.
plausible biological pathway. This requires that isotreti-
Psychiatric diagnoses were established with the Structured
Clinical Interview for DSM-IV, Patient Edition (SCID-P) (57).
noin must enter the central nervous system (CNS) and
There were no current psychiatric conditions in any subject ac-
have an effect on the functioning of brain areas and neu-
cording to the SCID-P. Two of the subjects in the antibiotic group
rochemical systems that mediate depression. Retinoids
had past psychiatric conditions, including a past history of major
have important effects on the developing brain in animal
depression in one and a past history of bulimia and alcohol de-
studies (29, 30), and use of isotretinoin during pregnancy
pendence in another. None of the isotretinoin subjects had a cur-rent or past psychiatric disorder. None of the subjects had current
has long been known to result in CNS defects in newborns
alcohol or substance abuse or dependence.
(31). Multiple positron emission tomography (PET) andsingle photon emission computed tomography (SPECT)
Behavioral Assessment
studies have shown low metabolism and/or blood flow at
Symptoms of depression were measured by using the Hamilton
baseline in depressed subjects in the left (32–35) and bilat-
Depression Rating Scale at baseline and every month after the ini-
eral (36–43) dorsolateral prefrontal cortex and medial pre-
tiation of treatment (58). The severity of acne was measured witha clinician-administered acne questionnaire before and after
frontal cortex/anterior cingulate (34, 38, 41–48) or blunted
treatment, on a scale of 0 (no acne) to 6 (very bad acne). The pa-
activation with cognitive tasks in the anterior cingulate (49,
tients’ subjective evaluations of the severity of acne on the face
50). Other PET and SPECT studies of patients with unipolar
and back and their feelings of depression related to their acne, on
depression showed low metabolism and/or blood flow in
a scale of 0 (not at all) to 4 (very severe), were recorded before and
the caudate (36–41, 51, 52), thalamus (37), temporal cortex
after treatment by using the Skindex questionnaire (59). The Skin-dex is a 16-item self-report questionnaire with questions about
(37, 38, 51, 53, 54), parietal cortex (34, 40, 51), and left puta-
emotional, functional, and symptomatic aspects of acne that has
men (37). Experimental induction of depression resulted
been validated for use in acne patient populations. It was also ad-
in a specific decrease in metabolism in the orbitofrontal
ministered before and after treatment. The patients were also
cortex (part of the prefrontal cortex) (55, 56). The purpose
evaluated during the course of treatment for symptoms related to
of the current study was to assess the effects of isotretinoin
treatment on brain functioning. We hypothesized that
PET and MRI Scanning
treatment with isotretinoin, but not antibiotic, would be
Two PET scans of resting brain metabolism were performed 4
associated with a decrease in orbitofrontal cortical brain
months apart, before and after treatment with isotretinoin or an-
metabolism as measured with [18F]fluorodeoxyglucose
tibiotic. The PET scans took place at 11:00 a.m. The subjects were
scanned with an ECAT EXACT 921 PET camera (CTI MolecularImaging, Knoxville, Tenn.). The ECAT EXACT has an axial field ofview of 16.2 cm, the total system sensitivity is 216 kcps/µCi per ml
for a 20-cm cylinder phantom in two dimensions, and the ap-proximate axial resolution is 5.0 mm (60). Each subject was
Subjects
placed in a preparation room adjacent to the PET scanner room,
The study participants included 28 healthy men and women
and an intravenous line was inserted in the hand and warmed
between the ages of 18 and 50 years with treatment-resistant
with a heating pad for measurement of arterialized venous blood
acne, as defined by a failed 3-month antibiotic trial, who were
samples. This method has been shown to yield metabolic values
seeking a second trial of an antibiotic or isotretinoin. Subjects
equivalent to those obtained by arterial line placement (61). The
were recruited by advertisement. They were not randomly as-
subject then received an intravenous injection of 10 mCi (370
signed to treatment with isotretinoin or placebo; they had de-
MBq) of FDG in a single bolus. Twenty-three arterialized venous
cided with their physicians to take either a second trial of an anti-
blood samples were obtained at multiple time points after injec-
biotic or a trial of isotretinoin. Because of the side effects of
tion for measurements of radioactivity in the plasma, which were
isotretinoin (severe skin dryness) it was decided that it would not
used for construction of a plasma time activity curve. Three blood
be possible to blind the subjects or the raters to treatment condi-
samples were also obtained for measurement of plasma glucose
tion. Subjects with serious medical or neurological illness, or-
concentrations. The subject was then placed in the scanner with
ganic mental disorder or current psychiatric illness according to
his or her head held in a head holder to minimize patient motion.
the Structured Clinical Interview for DSM-IV (57), premenstrual
The head was positioned with the canthomeatal line parallel to
dysphoric disorder, current alcohol or substance abuse or depen-
the external laser light. Following positioning within the camera
dence, retained metal that would prevent magnetic resonance
gantry, postinjection transmission data were collected by using
imaging (MRI) scanning, a history of head trauma or loss of con-
rod windowing with three orbiting 67Ga/68Ge rod sources (60).
sciousness, a history of cerebral infectious disease, or dyslexia
These data were used to correct the emission data for attenuation
were excluded. Postmenopausal women were excluded.
due to overlying bone and soft tissue. The subject underwent
This project was approved by the Emory University Human
emission scanning of the brain over the 40–60 minutes after injec-
Investigation Committee. All subjects provided written in-
tion with his or her eyes open in a dimly lit room. Brain and tissue
formed consent for participation. The subjects were paid for
measurements were used to estimate the cerebral glucose meta-
bolic rate (in milligrams per minute per 100 milliliters) (62, 63). In
Each subject received a PET brain scan at baseline and again
one patient blood samples could not be obtained, and this pa-
after 4 months of treatment with an antibiotic (N=15) or isotretin-
tient’s data were used only for the analysis of the ratio of regional
oin (N=13). The subjects were treated by their outpatient physi-
metabolism to whole brain metabolism. A 20-cm cylindrical
cians with 1 mg/kg of isotretinoin or with an antibiotic in a stan-
fluid-filled phantom with a known amount of radioactivity was
dard 4-month course of treatment for acne. The antibiotics used
scanned in order to obtain calibration factors for conversion of
included doxycycline (N=10), minocycline (N=2), tetracycline (N=
native pixel values into units of millicuries per milliliter. BREMNER, FANI, ASHRAF, ET AL.
MRI scans were obtained in all subjects for coregistration with
FIGURE 1. Flow of Subjects in a Brain Imaging Study of
the PET scans and determination of regions of interest from the
Patients Receiving Isotretinoin or Antibiotic Treatment for
MRI scans resliced to correspond to the PET slices. MRI scans in
the same subjects were obtained on a 1.5-T Philips Gyroscan In-tera device (Philips Medical Systems, Andover, Mass.). Axial im-
Initially screened for participation (N=88)
ages were acquired with a T1-weighted gradient echo three-di-mensional sequence with TR=35 msec, TE=12 msec, flip angle=
35°, number of excitations=2, matrix=256×256, field of view=22
Lack of follow-up/lack of interest (N=30)
Image Processing and Analysis
Current or previous isotretinoin treatment (N=10) Psychiatric disorder (N=1)
The PET and MRI scans were transferred to a workstation for
analysis. A surface-matching algorithm and the ANALYZE soft-
Met criteria for participation, signed informed consent
ware package (Mayo Clinic, Rochester, Minn.) were used for
statement, and were identified for treatment (N=44)
coregistration of images (64). Brain surfaces from PET and MRIwere matched by using this program. The MRI scan was reslicedto correspond to the PET slices. Using this technique (65), we
have shown a registration error of 2.86 mm. Regions of interest
were drawn on the resliced MRI scans by a blinded rater usingspecific criteria based on anatomical landmarks with a method
that we have shown to be highly reliable (66). Multiple brain re-
gions were selected for analysis, including the temporal cortex,
inferior, middle, and superior frontal gyri, superior portion of the
dorsolateral prefrontal cortex, thalamus, putamen, caudate, oc-
cipital cortex, subcallosal gyrus, orbitofrontal cortex, anteriorcingulate, postcentral gyrus, hippocampus, amygdala, and mid-
brain. These regions correspond to the regions measured in our
prior studies of neural findings associated with a return of depres-sive symptoms induced by tryptophan depletion (55) and alpha-
Dropped out (N=2): Lack of follow-through
methylparatyrosine (56), since a primary aim of the current study
was to replicate the brain findings of those prior studies. Global
brain metabolism was calculated as the mean of brain tissue ac-tivity in all slices, including gray and white matter and the ventric-
Data Analysis
The brain regions were separated into those that were and were
not hypothesized to change with isotretinoin. The region most
consistently affected in our two prior studies of depression wasthe orbitofrontal cortex (55, 56). This region has also been re-
ported to be smaller in volume in depressed patients than in
The data were analyzed to determine differences in the
changes from pre- to posttreatment in regional brain metabolic
a Of the 88 subjects screened initially, 44 were identified to start
rates between the isotretinoin and antibiotic treatment groups,
treatment with isotretinoin or antibiotics. Sixteen later dropped out
by using repeated-measures analysis of variance with time (be-
because of medical conditions (N=2), psychiatric diagnoses as de-
fore and after treatment) as the repeated factor and treatment sta-
termined with the Structured Clinical Interview for DSM-IV (N=6), a
tus (isotretinoin versus antibiotic) and hemisphere (left versus
change of mind about the study (N=2), or a lack of follow-through
right) as factors in the analysis. The interaction between treat-
ment status and time was examined in this model. Secondaryanalysis examined the ratio of regional to whole brain metabo-lism, and it added baseline global metabolism as a factor in the
the Skindex. Corrections were made for multiple comparisons (p=
model. Bonferroni corrections were performed to correct for mul-
tiple comparisons (p=0.05/12=0.004).
The data were analyzed by using the SAS System for Windows
Correlations between brain metabolism and behavioral vari-
ables were also examined by comparing the relationships be-tween the changes, from before to after treatment, in scores on
the Hamilton depression scale, clinician-administered acnequestionnaire, Skindex, and acne severity self-report and the
Recruitment and Demographic Factors
change in regional brain metabolism (mean of left and right
of Subjects
orbitofrontal metabolism) in the isotretinoin and antibiotic treat-ment groups. Corrections were made for multiple comparisons
Eighty-eight subjects were initially screened for partici-
(p=0.05/4=0.0125). Analyses also examined the correlation be-
pation in the study. Of these, 44 met the criteria for partic-
tween baseline orbitofrontal brain metabolism and age, educa-tion, and behavioral factors related to self-assessment of acne se-
ipation according to the initial screening, signed informed
verity, depression, and emotions related to acne, measured with
consent statements, and were identified as acne patients
ISOTRETINOIN AND BRAIN FUNCTIONING TABLE 1. Pretreatment Demographic and Behavioral Characteristics of Patients Receiving Isotretinoin or Antibiotic Treatment for Acne
Score on clinician-administered acne questionnairea
Skindex (59) score for behavioral effects of acneb
a On a scale of 0 (none) to 6 (very bad). b On a scale of 0 (not at all) to 64 (very bad). c On a scale of 0 (not at all) to 4 (very severe).
who were beginning a second trial of antibiotic (N=22) or
brain metabolism (F=4.64, df=1, 110, p<0.05). A secondary
who were going to be treated with isotretinoin (N=22) (Fig-
analysis included pretreatment whole brain metabolism
ure 1). Twenty-eight subjects completed participation in
in the model and also showed greater reductions in orbito-
this protocol, including pre- and posttreatment imaging.
frontal metabolism after treatment in the isotretinoin
Of these, 13 were treated with isotretinoin and 15 with
group than in the antibiotic group (F=9.66, df=1, 104, p=
0.002). The value for the interaction between treatment
Demographic, behavioral, and acne-related variables
status (isotretinoin versus antibiotic) and time (before and
related to the two treatment groups before the initiation of
after treatment) and the percentage change in the mean
treatment are presented in Table 1. The isotretinoin sub-
metabolic value with treatment are presented for each re-
jects had fewer years of education and were younger, but
gion in Table 2. Differences in functioning between the
the latter difference was not statistically significant. They
groups at the p<0.05 level were also seen for the middle
did not differ significantly from the antibiotic group in
frontal gyrus, thalamus, hippocampus, caudate, and puta-
their reasons for receiving treatment (cystic acne, psycho-
men. These differences were not significant after correc-
logical distress, scarring, or a combination). According to
tion for multiple comparisons, however, and there were no
the clinician ratings, the isotretinoin subjects had more
differences after we corrected for whole brain metabolism
severe pretreatment acne than the subjects receiving anti-
by examining differences in the ratios of regional to whole
biotics. However, according to the self-ratings there were
no differences in acne on the face or back or in feelings of
The mean pretreatment rate of metabolism in the or-
depression related to the acne. There were no differences
bitofrontal cortex was higher for patients in the isotretinoin
between the two groups in behavioral, emotional, and
group than for those in the antibiotic group (F=2.05, df=7,
functional effects of acne as measured by the Skindex.
107, p=0.03). This was not hypothesized a priori and was
There were also no differences in baseline depressive
not significant after correction for multiple comparisons.
symptom levels as measured by the Hamilton depression
Relationship Between Behavior and Brain Metabolism Effects of Isotretinoin on Regional
Five patients treated with isotretinoin had symptoms of
Cerebral Metabolism
headache. These patients also had subtle changes in irrita-
Administration of isotretinoin but not antibiotic was as-
bility and/or mood as assessed by self, family, or the re-
sociated with decreased brain metabolism in the orbito-
search staff. These subjects all had decreases in brain
frontal cortex after 4 months of treatment (Figure 2, Figure
metabolism with isotretinoin administration (Figure 2). A
3). This effect was seen for both absolute metabolism (Fig-
representative subject is shown in Figure 3. However,
ure 2, Table 2) and for the ratio of orbitofrontal to whole
these subjects did not show clinically significant depres-
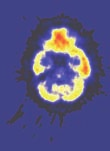
BREMNER, FANI, ASHRAF, ET AL. FIGURE 2. Effects of Isotretinoin and Antibiotics on Orbito- FIGURE 3. Effects on Re gional Brain Metabolism in a frontal Cortical Metabolism in Patients Receiving Treat- Representative Patient Receiving Isotretinoin Treatment ment for Acnea for Acnea Orbitofrontal cortex Baseline Posttreatment
a There was a visible decrease in metabolism in the orbitofrontal cor-
Glucose Metabolic Rate (mg/min per 100 g)
tex following isotretinoin administration in this patient. This pa-
tient suffered from headache, was noted by her family and clini-
cian to have disturbed behavior, and dropped out of school. She
did not, however, have a clinically significant increase in depression
Subjects Treated Subjects Treated
as measured by the Hamilton depression scale. With Isotretinoin With Antibiotics
a Isotretinoin but not antibiotic administration resulted in a signifi-
treatment in the isotretinoin group was correlated with a
cant decrease in orbitofrontal cortical metabolism (p<0.001,ANOVA). The mean percentage change with treatment within indi-
single item of the Skindex at baseline, effect of acne on
vidual subjects was –21% for isotretinoin and 2% for antibiotic.
ability to work (r=–0.67, N=9, p=0.03). This correlation wasnot significant after correction for multiple comparisons.
sion as assessed with the Hamilton depression scale (Fig-
There was no relationship between “worrying about skin
ure 4). One subject in the isotretinoin group and one in the
condition” as measured with the Skindex and orbitofron-
antibiotic group had a clinically significant increase in de-
tal metabolism at baseline or with treatment. There was
pression as measured by the Hamilton scale (greater than
no correlation between acne-related depression at base-
9-point increase); however, there were no significant in-
line and decrease in orbitofrontal cortical metabolism
creases in Hamilton depression scores in the groups as a
whole and no significant differences between groups.
There was no correlation between age or education and
Patients in the isotretinoin group had more severe acne
baseline orbitofrontal cortical metabolism or change in
as rated by clinician assessment at baseline (F=18.80, df=1,
25, p<0.05), and they had a greater improvement withisotretinoin treatment, as indicated by less severe acne ac-
Discussion
cording to the clinician-administered questionnaire after
A 4-month treatment trial with isotretinoin was associ-
treatment than before treatment, than did patients receiv-
ated with a decrease in brain functioning in the orbito-
ing antibiotics (F=22.73, df=1, 25, p<0.05). There was also a
frontal cortex, a brain region implicated in depression.
greater improvement with isotretinoin in self-reported
These changes were not seen after a similar course of
acne (F=2.62, df=4, 88, p<0.05). There were no differences
treatment with an antibiotic. After correction for differ-
in change in feelings of “depression related to acne” be-
ences in whole brain metabolism, this effect was specific
tween the groups. There was no relationship in either the
to the orbitofrontal cortex. The greatest magnitude of de-
isotretinoin or antibiotic group between baseline orbito-
crease was observed in subjects who developed symptoms
frontal cortical metabolism and depression as measured
of headache during the course of treatment with isotreti-
with the Hamilton scale, self-reported or clinician-assessed
noin. Isotretinoin was not associated, however, with any
acne severity as measured with the analogue scales, feel-
changes in depressive symptom severity as measured with
ings of depression related to acne as measured with the
analogue scale or the Skindex, effects of acne on work
Isotretinoin has a variety of effects on brain neurochem-
functioning as measured by the Skindex, or overall psy-
ical systems (69–71). Retinoids modulate gene expression
chological effects of acne as measured with the Skindex.
in the brain in a broad spectrum and have effects on sev-
The decrease in orbitofrontal cortical metabolism with
eral neurochemical systems, including the dopamine sys-
ISOTRETINOIN AND BRAIN FUNCTIONING TABLE 2. Regional Brain Metabolic Rates of Patients Before and After Isotretinoin or Antibiotic Treatment for Acne
a Percent change in mean metabolic rate. FIGURE 4. Effects of Isotretinoin and Antibiotic on Symp-
mesolimbic dopamine functioning (75). Retinoids are as-
toms of Depression in Patients Receiving Treatment for
sociated with an inhibition of neurogenesis in the hippo-
campus (76), a brain area with connections to prefrontalcortical areas, including the orbitofrontal cortex. Inhibi-
tion of neurogenesis in the hippocampus has been hy-
pothesized to play a role in depression (77–80). Retinoids
also have effects on brain trophic factors (81). These find-ings have led to the hypothesis that retinoids play a role inthe development of psychiatric disorders (69, 82).
A number of limitations of the current study are worthy
of mention. This was a pilot study designed to evaluate thepossibility of an effect of isotretinoin on brain functioning.
For this reason the study group was small, which may havecontributed to the fact that we did not observe treatment-
Mean (±SD) Score on
related changes in mood as assessed by the behavioral rat-
ings in this study. Some patients, however, complained of
Hamilton Depression Rating Scale
headache with isotretinoin, and these patients exhibitedgreater decreases in orbitofrontal brain metabolism dur-
ing isotretinoin treatment. Because of the costs of isotret-
Time of Treatment (months)
inoin we were unable to pay for this medication for all
a Depression was measured with the 21-item Hamilton Depression
subjects. Therefore, we were unable to randomly assign
Rating Scale. There was no significant effect of either isotretinoin or
subjects to treatment with isotretinoin or antibiotic and
antibiotic on depressive symptom severity.
were unable to control which antibiotic the subjects weretaking. We therefore recruited subjects who were prepar-
tem, which has been hypothesized to play a role in dys-
ing to undergo a second treatment course with an antibi-
regulation of mood and emotion (70). High levels of the
otic or to switch to isotretinoin on the basis of a decision
enzyme involved in retinoid synthesis, aldehyde dehy-
made in conjunction with the subject’s own physician.
drogenase, are found in mesostriatal and mesolimbic
This method likely contributed to the fact that the isotret-
dopamine pathways (72, 73). Dopamine mesocortical
inoin subjects had more severe acne at baseline. The
pathways involve release of dopamine transmitter in the
isotretinoin group also had less education. We examined a
orbitofrontal cortex and other parts of the prefrontal cor-
variety of demographic factors, including age, education,
tex. Isotretinoin may influence these pathways. Adminis-
psychological distress, and self- and clinician assessments
tration of retinoids causes changes in dopamine receptors
of acne severity, and found no relationships with baseline
(74), while genetic mutations of retinoid receptors are as-
orbitofrontal metabolism or change in orbitofrontal func-
sociated with deficits in dopamine receptors as well as
tioning with treatment. An unexpected finding was a pat-
BREMNER, FANI, ASHRAF, ET AL.
tern of greater baseline functioning in the orbitofrontal
sults of an international survey. Dermatology 1997; 194:351–
cortex in the isotretinoin group than in the antibiotic
2. Goulden V, Layton AM, Cunliffe WJ: Current indications for
group. One might question whether factors in the isotret-
isotretinoin as a treatment for acne vulgaris. Dermatology
inoin group, such as increased worrying related to more
severe acne, might have contributed to differences in
3. Jick SS, Kremers HM, Vasilakis-Scaramozza C: Isotretinoin use
brain functioning. Obsessive-compulsive disorder has
and risk of depression: psychotic symptoms, suicide, and at-
been associated with higher orbitofrontal metabolism
tempted suicide. Arch Dermatol 2000; 136:1231–1236
(83). However, we did not observe any differences in de-
4. Wysowski DK, Pitts M, Beitz J: An analysis of reports of depres-
sion and suicide in patients treated with isotretinoin. J Am
pression, psychological distress, or even self-rating of acne
severity between the two groups before treatment. We also
5. Byrne A, Costello M, Greene E, Zibin T: Isotretinoin therapy and
did not find a correlation between orbitofrontal metabo-
depression: evidence for an association. Irish J Psychosomatic
lism at baseline or change with treatment and the item re-
lated to “worrying about skin condition” on the Skindex.
6. Bremner JD: Does isotretinoin cause depression and suicide?
Antibiotics act by inhibiting bacterial protein synthesis.
7. Meyskens FLJ: Short clinical reports. J Am Acad Dermatol 1982;
Although they can pass the blood-brain barrier, they are
not known to have effects on brain functioning. The most
8. Duke EE, Guenther L: Psychiatric reactions to the retinoids (let-
common side effects of antibiotics are nausea, vomiting,
and diarrhea (84), and psychiatric and neurological side
9. Bigby M, Stern RS: Adverse reactions to isotretinoin. J Am Acad
effects are much more common in acne patients treated
10. Hazen PG, Carney JF, Walker AE, Stewart JJ: Depression: a side
with isotretinoin than those treated with antibiotics. For
effect of 13-cis-retinoic acid therapy. J Am Acad Dermatol
this reason it is unlikely that effects of antibiotics on brain
functioning would account for the results of the current
11. Middelkoop T: Roaccutane (isotretinoin) and the risk of sui-
study. We excluded subjects with a history of mental ill-
cide: case report and a review of the literature and pharma-
ness. This may have involved exclusion of subjects who
covigilance reports. J Pharmacy Practice 1999; 12:374–378
12. Villalobos D, Ellis M, Snodgrass WR: Isotretinoin (Accutane)-as-
were prone to the development of depression and may
sociated psychosis (letter). Vet Hum Toxicol 1989; 31:362
limit the generalizability of the findings. In summary, a
13. Bravard P, Krug M, Rzeznick JC: Isotretinoine et depression: soy-
randomized, placebo-controlled study would provide
ons vigilants (letter). Nouvelle Dermatology 1993; 12:215
more definitive results than the current study.
14. Scheinman PL, Peck GL, Rubinow DR, DiGiovanna JJ, Abangan
DL, Ravin PD: Acute depression from isotretinoin. J Am Acad
To our knowledge, this is the first study of the effects of
isotretinoin on human brain functioning. The findings
15. Hull PR, Demkiw-Bartel C: Isotretinoin use in acne: prospective
suggest that isotretinoin may affect brain functioning,
evaluation of adverse events. J Cutan Med Surg 2000; 4:66–70
providing a possible biological mechanism by which
16. Rodahl K, Moore T: Vitamin A content and toxicity of bear and
isotretinoin treatment could lead to depression in a mi-
nority of vulnerable acne patients. Future studies using
17. Restak RM: Pseudotumor cerebri, psychosis, and hypervitami-
nosis A. J Nerv Ment Dis 1972; 155:155–172
randomized designs to evaluate the effects of isotretinoin
18. McCance-Katz EF, Price LH: Depression associated with Vitamin
A intoxication (letter). Psychosomatics 1992; 33:117–118
19. Fishbane S, Frei GL, Finger M, Dressler R, Silbiger S: Hypervita-
Received April 20, 2004; revision received June 3, 2004; accepted
minosis A in two hemodialysis patients. Am J Kidney Dis 1995;
June 14, 2004. From the Departments of Psychiatry and Behavioral
Sciences, Radiology, and Medicine (Cardiology) and the Emory Center
20. Jacobs DG, Deutsch N, Brewer M: Suicide, depression, and
for Positron Emission Tomography, Emory University School of Medi-
isotretinoin: is there a causal link? J Am Acad Dermatol 2001;
cine; and the Psychiatry Service, Atlanta Department of Veterans Af-
fairs Medical Center, Decatur, Ga. Address correspondence and re-
21. Lamberg L: Acne drug depression warnings highlight need for
print requests to Dr. Bremner, Department of Psychiatry and
Behavioral Sciences, Emory University, 1256 Briarcliff Rd., Atlanta, GA
22. Cassileth BR, Lusk EJ, Tenaglia AN: A psychological comparison
of patients with malignant melanoma and other dermatologic
Supported by funding from Liam Grant, director of the Roaccu-
disorders. J Am Acad Dermatol 1982; 7:742–746
tane Action Group (80%), and by lawyers involved in Accutane litiga-tion (20%).
23. Shuster S, Fisher GH, Harris E, Binnel D: The effect of skin dis-
ease on self-image. Br J Dermatol 1978; 99:18–19
The authors thank Delicia Votaw, C.N.M.T., Michael White, C.N.M.T.,
Margie Jones, C.N.M.T., Kim Egeler, C.N.M.T., Ron Crowe, Pharm.D.,
24. Van der Meeren HLM, van der Schaar WW, van den Hurk
and Shane Waldrep, B.S., for assistance in positron emission tomog-
CMAM: The psychological impact of severe acne. Cutis 1985; 7:
25. Garrie SA, Garrie EV: Anxiety and skin diseases. Cutis 1978; 22:
References
26. Medansky RS, Handler RM, Medansky DL: Self-evaluation of
acne and emotion: a pilot study. Psychosomatics 1981; 22:
1. Cunliffe WJ, van der Kerkhof PCM, Caputo R, Caicchini S, Coo-
per A, Fyrand OL, Gollnick H, Layton AM, Leyden JJ, Mascaro J-
27. Rubinow DR, Peck GL, Squillace KM, Gantt GG: Reduced anxiety
M, Ortonne J-P, Shalita A: Roaccutane treatment guidelines: re-
and depression in cystic acne patients after successful treat-
ISOTRETINOIN AND BRAIN FUNCTIONING
ment with oral isotretinoin. J Am Acad Dermatol 1987; 17:25–
46. Mayberg HS, Starkstein SE, Peyser CE, Brandt J, Dannals RF, Fol-
stein SE: Paralimbic frontal lobe hypometabolism in depres-
28. Kellett SC, Gawkrodger DJ: The psychological and emotional
sion associated with Huntington’s disease. Neurology 1992;
impact of acne and the effect of treatment with isotretinoin. Br
47. Ring RA, Bench CJ, Trimble MR, Brooks DJ, Frackowiak RSJ,
29. Hyatt GA, Schmitt EA, Marsh-Armstrong N, McCaffery P, Drager
Dolan RJ: Depression in Parkinson’s disease: a positron emis-
UC, Dowling JE: Retinoic acid establishes ventral retinal charac-
sion study. Br J Psychiatry 1994; 165:333–339
teristics. Development 1996; 122:195–204
48. Mayberg HS, Brannan SK, Tekell JL, Silva JA, Mahurin RK,
30. Wilson L, Gale E, Maden M: The role of retinoic acid in the mor-
McGinnis S, Jerabek PA: Regional metabolic effects of fluoxet-
phogenesis of the neural tube. J Anat 2003; 203:357–368
ine in major depression: serial changes and relationship to
31. Maden M, Holder N: Retinoic acid and development of the
clinical response. Biol Psychiatry 2000; 48:830–843
central nervous system. Bioessays 1992; 14:431–438
49. Bremner JD, Vythilingam M, Vermetten E, Vaccarino V, Charney
32. Martinot JL, Hardy P, Feline A, Huret J-D, Mazoyer B, Attar-Levy
DS: Deficits in hippocampal and anterior cingulate functioning
D, Pappata S, Syrota A: Left prefrontal glucose hypometabo-
during verbal declarative memory encoding in midlife major
lism in the depressed state: a confirmation. Am J Psychiatry
depression. Am J Psychiatry 2004; 161:637–645
50. George MS, Ketter TA, Parekh PI, Rosinsky N, Ring HA, Pazzaglia
33. Baxter LR, Schwartz JM, Phelps ME, Mazziotta JC, Guze BH, Selin
PJ, Marangell LB, Callahan AM, Post RM: Blunted left cingulate
CE, Gerner RH, Smida RM: Reduction of prefrontal cortex glu-
activation in mood disorder subjects during a response inter-
cose metabolism common to three types of depression. Arch
ference task (the Stroop). J Neuropsychiatry Clin Neurosci 1997;
34. Bench CJ, Friston KJ, Brown RG, Scott LC, Frackowiak RSJ, Dolan
51. Drevets WC, Raichle ME: Neuroanatomical circuits in depres-
RJ: The anatomy of melancholia: focal abnormalities of cere-
sion: implications for treatment mechanisms. Psychopharma-
bral blood flow in major depression. Psychol Med 1992; 22:
52. Baxter LR, Phelps ME, Mazziotta JC, Schwartz JM, Gerner RH, Se-
35. Ebert D, Feistel H, Barocka A: Effects of sleep deprivation on
lin CE, Sumida RM: Cerebral metabolic rates for glucose in
the limbic system and the frontal lobes in affective disorders: a
mood disorders. Arch Gen Psychiatry 1985; 42:441–447
study with Tc-99m-HMPAO SPECT. Psychiatry Res 1991; 40:247–
53. Post RM, DeLisi LE, Holcomb HH, Uhde TW, Cohen R, Buchs-
baum MS: Glucose utilization in the temporal cortex of affec-
36. Buchsbaum MS, DeLisi LE, Holcomb H, Cappelletti J, King AC,
tively ill patients: positron emission tomography. Biol Psychia-
Johnson J, Hazlett E, Dowling-Zimmerman S, Post RM, Morihisa
J, Carpenter W, Cohen R, Pickar D, Weinberger DR, Margolin R,
54. Brody AL, Saxena S, Stoessel P, Gillies LA, Fairbanks LA, Albor-
Kessler RM: Anteroposterior gradients in cerebral glucose use
zian S, Phelps ME, Huang SC, Wu HM, Ho ML, Ho MK, Au SC,
in schizophrenia and affective disorders. Arch Gen Psychiatry
Maidment K, Baxter LR: Regional brain metabolic changes in
patients with major depression treated with either paroxetine
37. Austin MP, Dougall N, Ross M, Murray C, O’Carroll RE, Moffoot
or interpersonal therapy: preliminary findings. Arch Gen Psy-
A, Ebmeier KP, Goodwin GM: Single photon emission tomogra-
phy with 99mTc-exametazime in major depression and the
55. Bremner JD, Innis RB, Salomon RM, Staib L, Ng CK, Miller HL,
pattern of brain activity underlying the psychotic/neurotic con-
Bronen RA, Duncan J, Krystal JH, Rich D, Malison R, Price LH,
Dey H, Soufer R, Charney DS: PET measurement of cerebral
38. Mayberg HS, Lewis PJ, Regenold W, Wagner HN: Paralimbic hy-
metabolic correlates of tryptophan depletion-induced depres-
poperfusion in unipolar depression. J Nucl Med 1994; 35:929–
sive relapse. Arch Gen Psychiatry 1997; 54:364–374
56. Bremner JD, Vythilingam M, Ng CK, Vermetten E, Nazeer A,
39. Hurwitz TA, Clark C, Murphy E, Klonoff H, Martin WRW, Pate
Oren D, Berman RM, Charney DS: Regional brain metabolic
BD: Regional cerebral glucose metabolism in major depressive
correlates of positron emission tomographic measurement of
disorder. Can J Psychiatry 1990; 35:684–688
alpha-methylparatyrosine-induced depressive symptoms: im-
40. Biver F, Goldman S, Delvenne V, Luxen A, De Maertelaer V, Hu-
plications for the neural circuitry of depression. JAMA 2003;
bain P, Mendlewicz J, Lotstra F: Frontal and parietal metabolic
disturbances in unipolar depression. Biol Psychiatry 1994; 36:381–388
57. First M, Spitzer R, Williams J, Gibbon M: Structured Clinical In-
terview for DSM-IV—Patient Edition (SCID-P). Washington, DC,
41. Mayberg HS: Frontal lobe dysfunction in secondary depression.
J Neuropsychiatry Clin Neurosci 1994; 6:428–442
42. Mayberg HS, Brannan SK, Mahurin RK, Jerabek PA, Brickman
58. Hamilton M: A rating scale for depression. J Neurol Neurosurg
JS, Tekell JL, Silva JA, McGinnis S, Glass TG, Martin CC, Fox PT:
Cingulate function in depression: a potential predictor of treat-
59. Chren MM, Lasek RJ, Sahay AP, Sands LP: Measurement proper-
ment response. Neuroreport 1997; 8:1057–1061
ties of Skindex-16: a brief quality-of-life measure for patients
43. Mayberg HS, Liotti M, Brannan SK, McGinnis S, Mahurin RK, Jer-
with skin diseases. J Cutan Med Surg 2001; 5:105–110
abek PA, Silva JA, Tekell JL, Martin CC, Lancaster JL, Fox PT: Re-
60. Weinhard K, Eriksson L, Grootoonk S, Casey ME, Pietrzyk U,
ciprocal limbic-cortical function and negative mood: converg-
Heiss WD: Performance evaluation of the positron scanner
ing PET findings in depression and normal sadness. Am J
ECAT EXACT. J Comput Assist Tomogr 1992; 16:804–813
61. Brownell GL, Kearfott KJ, Kairento A-L, Elmaleh DR, Alpert NM,
44. Drevets WC, Price JL, Simpson JRJ, Todd RD, Reich T, Vannier M,
Correia JA, Wechsler L, Ackerman RH: Quantitation of regional
Raichle ME: Subgenual prefrontal cortex abnormalities in
cerebral glucose metabolism. J Comput Assist Tomogr 1983; 7:
mood disorders. Nature 1997; 386:824–827
45. Mayberg HS, Starkstein SE, Sadzot B, Preziosi T, Andrezejewski
62. Phelps ME, Huang SC, Hoffman EJ, Selin C, Sokoloff L, Kuhl DE:
PL, Dannals RF, Wagner HN, Robinson RG: Selective hypome-
Tomographic measurement of local cerebral glucose meta-
tabolism in the inferior frontal lobe in depressed patients with
bolic rate in humans with (F-18)2-fluoro-2-deoxy-D-glucose:
Parkinson’s disease. Ann Neurol 1990; 28:57–64
validation of method. Ann Neurol 1979; 6:371–388
BREMNER, FANI, ASHRAF, ET AL.
63. Sokoloff L, Reivich M, Kennedy C, Des Rosiers MH, Patlak CS,
74. Farooqui SM: Induction of adenylate cyclase sensitive dopa-
Pettigrew KD, Sakurada O, Shinohara M: The [14]deoxyglucose
mine D2 receptors in retinoic acid induced differentiated hu-
method for the measurement of local cerebral glucose utiliza-
man neuroblastoma SHSY-5Y cells. Life Sci 1994; 55:1887–
tion: theory, procedure, and normal values in the conscious
and anesthetized albino rat. J Neurochem 1977; 28:897–916
75. Krezel W, Ghyselinck N, Samad TA, Dupe V, Kastner P, Borreli E,
64. Robb RA, Hanson DP, Karwoski RA, Larson AG, Workman EL,
Chambon P: Impaired locomotion and dopamine signaling in
Stacy MC: Analyze: a comprehensive, operator-interactive soft-
retinoid receptor mutant mice. Science 1998; 279:863–867
ware package for multidimensional medical image display and
76. Crandall J, Sakai Y, Zhang J, Koul O, Mineur Y, Crusio WE, McCaf-
analysis. Comput Med Imaging Graph 1989; 13:433–454
fery P: 13-cis-retinoic acid suppresses hippocampal cell divi-
65. Zubal IG, Zhang L, Tagare B, Duncan JS: 3-D registration of
sion and hippocampal-dependent learning in mice. Proc Natl
SPECT and MRI brain images (abstract). J Nucl Medicine 1993;
77. Duman RS, Heninger GR, Nestler EJ: A molecular and cellular
66. Bremner JD, Bronen RA, de Erasquin G, Vermetten E, Staib L,
theory of depression. Arch Gen Psychiatry 1997; 54:597–606
Ng CK, Soufer R, Charney DS, Innis RB: Development and reli-
78. Santarelli L, Saxe M, Gross C, Surget A, Battaglia F, Dulawa S,
ability of a method for using magnetic resonance imaging for
Weisstaub N, Lee J, Duman R, Aranico O, Belzung C, Hen R: Re-
the definition of regions of interest for positron emission to-
quirement of hippocampal neurogenesis for the behavioral ef-
mography. Clin Positron Imaging 1998; 1:145–159
fects of antidepressants. Science 2003; 301:805–809
67. Bremner JD, Vythilingam M, Vermetten E, Nazeer A, Adil J,
79. Bremner JD, Narayan M, Anderson ER, Staib LH, Miller HL,
Khan S, Staib LH, Charney DS: Reduced volume of orbitofrontal
Charney DS: Hippocampal volume reduction in major depres-
cortex in major depression. Biol Psychiatry 2002; 51:273–279
sion. Am J Psychiatry 2000; 157:115–117
68. Lai TJ, Payne ME, Byrum CE, Steffens D, Krishnan KR: Reduction
80. Sheline YI, Wang P, Gado M, Csernansky J, Vannier M: Hippo-
of orbital frontal cortex volume in geriatric depression. Biol
campal atrophy in major depression. Proc Natl Acad Sci USA
69. Goodman AB: Three independent lines of evidence suggest re-
81. Johann V, Jeliaznik N, Schrage K, Mey J: Retinoic acid downreg-
tinoids as causal to schizophrenia. Proc Natl Acad Sci USA
ulates the expression of ciliary neurotrophic factor in rat
Schwann cells. Neurosci Lett 2003; 339:13–16
70. Jentsch JD, Roth RH, Taylor JR: Role for dopamine in the behav-
82. Goodman AB: Chromosomal locations and modes of action of
ioral functions of the prefrontal corticostriatal system: implica-
genes in the retinoid (vitamin A) system support their involve-
tions for mental disorders and psychotropic drug action. Prog
ment in the etiology of schizophrenia. Am J Med Genet Neu-
71. Risch SC, Nemeroff CB: Neurochemical alterations of seroton-
83. Rauch SL, Jenike MA, Alpert NM, Baer L, Breiter HC, Savage CR,
ergic neuronal systems in depression. J Clin Psychiatry 1992;
Fischman AJ: Regional cerebral blood flow measured during
symptom provocation in obsessive-compulsive disorder using
72. McCaffery P, Drager UC: High levels of a retinoic acid-generat-
oxygen 15-labeled carbon dioxide and positron emission to-
ing dehydrogenase in the meso-telencephalic dopamine sys-
mography. Arch Gen Psychiatry 1994; 51:62–70
tem. Proc Natl Acad Sci USA 1994; 91:7772–7776
84. Chambers HF: Chloramphenicol, tetracyclines, macrolides,
73. McCaffery P, Drager UC: Hot spots of retinoic acid synthesis in
clindamycin, and streptogramins, in Basic and Clinical Phar-
the developing spinal cord. Proc Natl Acad Sci USA 1994; 91:
macology. Edited by Katzung BG. New York, Appleton-Lange,
Journal of Biblical Ethics in Medicine – Volume 7, Number 2 Editor's Note Like termites in an oak stump, articles on euthanasiaQuite honestly, he did consider that he might be acontinue to reduce to dry powder the humbledpagan. One wonders more about his minister-friend. Heremnants of biblical precepts in medicine. The April,has "witnessed" to Dr. Walker, all right. All of our1
Podemos esperar que no esté muy lejano el día de la unidad Salón de actos del seminario de Friburgo de Brisgovia, Eminencias, Excelencias, Venerables representantes de las Iglesias Ortodoxas y Ortodoxas Orientales: Me alegra mucho que hoy estemos aquí reunidos. Les agradezco de todo corazón su presencia y la posibilidad de este encuentro amistoso. Agradezco en particular al Metropoli

 BREMNER, FANI, ASHRAF, ET AL.
BREMNER, FANI, ASHRAF, ET AL.