Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Guideline 9.2.5 first aid for asthma
AUSTRALIAN RESUSCITATION GUIDELINE 9.2.5 FIRST AID FOR ASTHMA INTRODUCTION 1
Asthma is a disorder of the smaller airways of the lungs. People with asthma have sensitive airways which can narrow when exposed to certain ‘triggers’, leading to difficulty in breathing. Three main factors cause the airways to narrow:
• The muscle around the airway tightens (bronchoconstriction).
• The inside lining of the airways becomes swollen (inflammation).
• Extra mucus (sticky fluid) may be produced.
In asthma, symptoms are made worse by 'triggers'. Every person's asthma is different and not all people will have the same triggers. Triggers can include:
• Inhaled allergens (e.g. pollens, moulds, animal dander and dust mites).
• Environmental factors (e.g. dust, pollution, wood smoke, bush fires).
• Changes in temperature and weather. • Certain medications (e.g. aspirin).
• Chemicals and strong smells (e.g. perfumes, cleaning products).
• Emotional factors (e.g. laughter, stress).
• Some foods and food preservatives, flavourings and colourings (uncommon).
RECOGNITION 1 Asthma can be recognised by the following symptoms and signs:
• A dry, irritating, persistent cough, particularly at night, early morning, with exercise or
• Wheeze (high pitched whistling sound during breathing).
Signs of a severe asthma attack include some or all of the following:
• Gasping for breath (may have little or no wheeze due to little movement of air).
• Inability to speak more than one or two words per breath.
• Feeling distressed and anxious. • Little or no improvement after using “reliever” medication.
• ‘Sucking in’ of the throat and rib muscles, use of shoulder muscles or bracing with arms to
• Blue discolouration around the lips (can be hard to see if skin colour also changes).
• Symptoms rapidly getting worse or using reliever more than every two hours.2
As well as the above symptoms, young children appear restless, unable to settle or become drowsy. A child may also ‘suck’ in muscles around the ribs and may have problems eating or drinking due to shortness of breath. A child also may have severe coughing and vomiting. An asthma attack can take anything from a few minutes to a few days to develop.
MANAGING AN ASTHMA ATTACK 3
If the victim has a personal written asthma action plan then that plan should be followed.
If there is no action plan in place then use the following Asthma First Aid plan. Asthma First Aid Plan
If a victim has any signs of a severe asthma attack, call an ambulance straight away and follow the Asthma First Aid Plan while waiting for the ambulance to arrive.
Sit the person comfortably upright. Be calm and reassuring. Do not leave the person alone.
Without delay give four separate puffs of a “reliever”. The medication is best given one puff at a time via a spacer device. If a spacer is not available, simply use the puffer.
Ask the person to take four breaths from the spacer after each puff of medication.
Use the victim’s own inhaler if possible. If not, use the first aid kit inhaler if available or borrow one from someone else.
The first aid rescuer should provide assistance with administration of a reliever if required.4 [LOE Expert Consensus Opinion]
Wait four minutes. If there is little or no improvement give another four puffs.
If there is still no improvement, call an ambulance immediately. Keep giving four puffs every four minutes until the ambulance arrives.
AUSTRALIAN RESUSCITATION COUNCIL
No harm is likely to result from giving a “reliever” puffer to someone without asthma.2 [LOE: Expert Consensus Opinion]. If oxygen is available, it should be administered at a flow rate of at least at 8 litres per minute through a face mask, by a person trained in its use.5 [LOE: Expert Consensus Opinion] If breathing stops, give resuscitation following Basic Life Support Flowchart (Guideline 8) If a severe allergic reaction is suspected, refer to ARC Guideline 9.2.7 Anaphylaxis – First Aid Management.
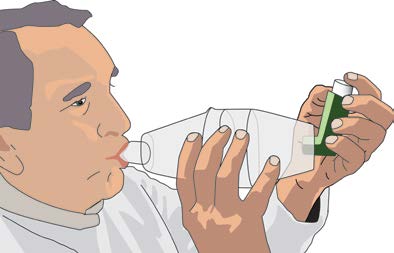
Diagrams for the use of Devices 4 WITH SPACER
Shake the inhaler and place the mouthpiece
into the spacer. Place the spacer mouthpiece
into the victim’s mouth, administer one puff
into the spacer and ask the victim to breathe in
and out normally for four breaths. Repeat this
promptly until four puffs have been given.
WITHOUT SPACER
inhaler. Place the mouthpiece into the victim’s
mouth and administer one puff as the victim inhales slowly and steadily. Ask the victim to hold their breath for four seconds and then take four normal breaths. Repeat this promptly until four puffs have been given.
The most common reliever medication is Salbutamol6. Alternative relievers that may considered for adults are terbutaline or eformoteral plus budesonide
AUSTRALIAN RESUSCITATION COUNCIL CLASS OF RECOMMENDATION
Class A - Recommended REFERENCES
1. Asthma Foundation of Victoria. Asthma, The Basic Facts. June 2006.
2. Asthma Foundation of Victoria. Asthma Action Plan. September 2007.
4. National Asthma Council. Emergency Asthma Management. First Aid for Asthma.
5. National Asthma Council Australia. Asthma Management Handbook 6th Edition 2006.
6. First Aid Science Advisory Board. Part 10: First Aid. Circulation, 2005.112:115-125. 6. http://www.betterhealth.vic.gov.au/bhcv2/bhcmed.nsf/pages/pucsalbu/$File/pucsalbu.pdf CROSS REFERENCES ARC Guideline 5 Breathing ARC Guideline 8 Cardiopulmonary Resuscitation ARC Guideline 9.2.7 Anaphylaxis – First Aid Management ARC Guideline 10.4 The Use of Oxygen in Emergencies AUSTRALIAN RESUSCITATION COUNCIL
No evidence for association between a functional promoter variantof the Norepinephrine Transporter gene SLC6A2 and ADHDin a family-based sampleT. J. Renner • T. T. Nguyen • M. Romanos •S. Walitza • C. Ro¨ser • A. Reif • H. Scha¨fer •A. Warnke • M. Gerlach • K. P. LeschReceived: 26 April 2011 / Accepted: 7 June 2011Ó Springer-Verlag 2011shown to have major influence on the
Referencelaboratorium for Kemiske Miljømålinger, Eurofins Miljø A/S Naturstyrelsen, Miljøministeriet Notater til opdatering af analysekvalitetsbekendtgørelsen Notat 11.11 EKSISTERENDE, NYE OG REVIDEREDE PRIORITEREDE STOFFER - BETYDNING FOR IGANGVÆRENDE REVISION AF BKG. OM ANALYSEKVALITET 1 Baggrund Arbejdsgruppe E om Kemiske aspekter (Kommissions DG Miljø, Direktorat D - Vand,

 AUSTRALIAN
AUSTRALIAN 

 No harm is likely to result from giving a “reliever” puffer to someone without asthma.2 [LOE: Expert Consensus Opinion]. If oxygen is available, it should be administered at a flow rate of at least at 8 litres per minute through a face mask, by a person trained in its use.5 [LOE: Expert Consensus Opinion] If breathing stops, give resuscitation following Basic Life Support Flowchart (Guideline 8) If a severe allergic reaction is suspected, refer to ARC Guideline 9.2.7 Anaphylaxis – First Aid Management.
Diagrams for the use of Devices 4
No harm is likely to result from giving a “reliever” puffer to someone without asthma.2 [LOE: Expert Consensus Opinion]. If oxygen is available, it should be administered at a flow rate of at least at 8 litres per minute through a face mask, by a person trained in its use.5 [LOE: Expert Consensus Opinion] If breathing stops, give resuscitation following Basic Life Support Flowchart (Guideline 8) If a severe allergic reaction is suspected, refer to ARC Guideline 9.2.7 Anaphylaxis – First Aid Management.
Diagrams for the use of Devices 4