Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
121699 a randomized study of the prevention of
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
A RANDOMIZED STUDY OF THE PREVENTION OF SUDDEN DEATH IN PATIENTS WITH CORONARY ARTERY DISEASE
ALFRED E. BUXTON, M.D., KERRY L. LEE, PH.D., JOHN D. FISHER, M.D., MARK E. JOSEPHSON, M.D.,
ERIC N. PRYSTOWSKY, M.D., AND GAIL HAFLEY, M.S.,
FOR THE MULTICENTER UNSUSTAINED TACHYCARDIA TRIAL INVESTIGATORS*
ABSTRACT Background
death from cardiovascular disease, mortali-
not reduced mortality among patients with coronary
ty after discharge from the hospital remains
artery disease and asymptomatic ventricular arrhyth-
mias. Previous studies have suggested that antiar-
infarction who have substantial left ventricular dys-
rhythmic therapy guided by electrophysiologic test-
function. Among such persons, the 6-to-12-month
ing might reduce the risk of sudden death.
mortality is 10 percent or higher and the 4-to-5-year
Methods
mortality is 20 percent or higher.1-4 Sudden death
trial to test the hypothesis that electrophysiologically
accounts for approximately one third of the late mor-
guided antiarrhythmic therapy would reduce the risk
tality.2,5 The appropriate treatment for survivors of
of sudden death among patients with coronary arterydisease, a left ventricular ejection fraction of 40 per-
out-of-hospital cardiac arrest has been clarified by re-
cent or less, and asymptomatic, unsustained ventric-
cent study results. However, only 2 to 30 percent
ular tachycardia. Patients in whom sustained ventric-
of persons who have cardiac arrest survive.5,7-9 Thus,
ular tachyarrhythmias were induced by programmed
primary prevention of cardiac arrest is imperative.
stimulation were randomly assigned to receive ei-
The Multicenter Unsustained Tachycardia Trial was
ther antiarrhythmic therapy, including drugs and im-
initiated in 1989 to test the hypothesis that antiar-
plantable defibrillators, as indicated by the results of
rhythmic therapy guided by electrophysiologic testing
electrophysiologic testing, or no antiarrhythmic ther-
can reduce the risks of sudden death and cardiac ar-
apy. Angiotensin-converting–enzyme inhibitors and
rest among patients with coronary artery disease, left
beta-adrenergic–blocking agents were administered
ventricular dysfunction, and spontaneous unsustained
if the patients could tolerate them. Results
A total of 704 patients with inducible, sus-
tained ventricular tachyarrhythmias were randomly
assigned to treatment groups. Five-year Kaplan–Meier estimates of the incidence of the primary end
Patients
point of cardiac arrest or death from arrhythmia were
Patients at 85 study sites in the United States and Canada were
25 percent among those receiving electrophysiolog-
identified as having coronary artery disease, a left ventricular ejection
ically guided therapy and 32 percent among the pa-
fraction of 40 percent or less, and asymptomatic unsustained ven-
tients assigned to no antiarrhythmic therapy (relative
tricular tachycardia (lasting for three or more beats). The qualify-ing unsustained tachycardia had to occur six months or less before
risk, 0.73; 95 percent confidence interval, 0.53 to 0.99),
enrollment, and four or more days after the most recent myocardial
representing a reduction in risk of 27 percent. The
infarction or revascularization procedure. Written informed con-
five-year estimates of overall mortality were 42 per-
sent was obtained from all the patients before randomization. The
cent and 48 percent, respectively (relative risk, 0.80;
institutional review board at each study site approved the protocol.
95 percent confidence interval, 0.64 to 1.01). The risk
Either cardiac catheterization or exercise testing within six
of cardiac arrest or death from arrhythmia among the
months before enrollment was required. If exercise-induced ische-
patients who received treatment with defibrillators
mia was detected, appropriate treatment was required before enroll-
was significantly lower than that among the patients
ment. Patients with a history of syncope or sustained ventricular
discharged without receiving defibrillator treatment
tachycardia or fibrillation more than 48 hours after the onset of my-ocardial infarction were excluded, as were patients whose unsus-
(relative risk, 0.24; 95 percent confidence interval, 0.13
tained ventricular tachycardia occurred only in the setting of acute
to 0.45; P<0.001). Neither the rate of cardiac arrest or
ischemia, metabolic disorders, or drug toxicity.
death from arrhythmia nor the overall mortality ratewas lower among the patients assigned to electro-
Protocol
physiologically guided therapy and treated with an-
A detailed description of the study protocol has been published
tiarrhythmic drugs than among the patients assigned
previously.10 An electrophysiologic study that included the deliv-
Conclusions
rhythmic therapy with implantable defibrillators, but
From the Department of Medicine, Brown University School of Medi-
not with antiarrhythmic drugs, reduces the risk of sud-
cine and Rhode Island Hospital, Providence (A.E.B.); Duke University
den death in high-risk patients with coronary disease.
Clinical Research Institute, Durham, N.C. (K.L.L., G.H.); the Departmentof Medicine, Montefiore Medical Center and Albert Einstein College of
Medicine, Bronx, N.Y. (J.D.F.); the Department of Medicine, Beth Israel Dea-
1999, Massachusetts Medical Society.
coness Medical Center, Boston (M.E.J.); and Care Group, Indianapolis(E.N.P.). Address reprint requests to Dr. Buxton at the Division of Cardiol-ogy, Rhode Island Hospital, 2 Dudley St., Suite 360, Providence, RI 02905.
*Other participants in the trial are listed in the Appendix. A R A N D O M I Z E D ST U DY O F T H E P R EV E N T I O N O F S U D D E N D E AT H I N PAT I E N T S W I T H C O R O N A RY A R T E RY D I S E AS E
ery of one to three extrastimuli and burst pacing at two right ven-
than 90 percent power to detect a rate of 20 percent. We encoun-
tricular sites during two paced cycle lengths was performed in the
tered considerable difficulty in meeting the targeted sample size,
absence of antiarrhythmic drugs. Stimulation was stopped after sus-
and the enrollment of patients was stopped in October 1996, af-
tained ventricular tachyarrhythmia had been reproducibly induced.
ter 704 patients with inducible, sustained ventricular tachyarrhyth-
Patients with sustained, monomorphic ventricular tachycardia
mia had undergone randomization. The patients were to be fol-
induced by any method of stimulation and those with sustained
polymorphic ventricular tachycardia (including ventricular flutter
Treatment groups were compared in an intention-to-treat analy-
and fibrillation) induced by one or two extrastimuli were random-
sis, and all statistical tests were two-tailed. Cumulative event rates
ly assigned in equal numbers to receive either antiarrhythmic ther-
were calculated by the Kaplan–Meier method, with the time to
apy guided by the results of electrophysiologic testing or no anti-
the first event as the outcome variable.12 The significance of the
arrhythmic therapy. Patients who refused to undergo randomization
difference between treatment groups was assessed with the log-
were also followed. Patients in whom no sustained tachyarrhyth-
rank test.13 Relative risk was expressed as a hazard ratio derived
mia was induced at the base-line study were followed without an-
from the Cox proportional-hazards model.14 Interim analyses of
tiarrhythmic therapy in a registry. Treatment with beta-adrenergic–
the data were performed at regular intervals according to standard
blocking agents and angiotensin-converting–enzyme inhibitors
practices of the National Institutes of Health and were reviewed
by an independent data and safety monitoring board. Compari-
Patients assigned to electrophysiologically guided therapy un-
sons of major outcomes in the interim analyses were monitored
derwent serial drug testing with antiarrhythmic drugs approved
with two-sided, symmetric O’Brien–Fleming boundaries gener-
by the Food and Drug Administration.10 Drugs were assigned
ated with the Lan–DeMets spending-function approach to group-
randomly, with the exception of amiodarone. Amiodarone could
be tested at the discretion of the investigator in patients in whom
To compare the outcomes of the patients assigned to electro-
at least two tests had failed. After four to five half-lives (approxi-
physiologically guided therapy who received defibrillators with the
mately two to three days; amiodarone was tested after at least one
outcomes of those who did not, we performed observational com-
week of loading), programmed stimulation was repeated. If fewer
parisons. The outcomes of the patients who received defibrillators
than 15 complexes were induced, long-term therapy with that
within 90 days after enrollment and before the occurrence of any
regimen was permissible. If no drug regimen could be found that
arrhythmic event were compared with the outcomes of patients
rendered the tachyarrhythmia noninducible, the investigator could
who were not given defibrillators before that time.
discharge the patient with a drug regimen that was associated with
In addition, covariate-adjusted assessments of the effect of de-
hemodynamic stability during induced tachycardia.10 No empiri-
fibrillator therapy on major outcomes were performed with the
cal antiarrhythmic-drug therapy was used.
Cox proportional-hazards regression model, in which receipt of a
Implantation of a defibrillator could be recommended after at
defibrillator was treated as a time-dependent covariate. Covariates
least one unsuccessful drug test. This aspect of the protocol was
examined in these analyses included age; sex; race; the date of en-
changed during the course of the trial in order to reflect changes
rollment (relative to the start of the trial); whether or not the pa-
in practice. The protocol initially required that three or more drug
tient had had a prior myocardial infarction, prior bypass surgery,
tests had to fail in patients assigned to receive electrophysiologi-
prior angioplasty, palpitations, or angina; ejection fraction; and the
cally guided antiarrhythmic therapy before a defibrillator could be
use or nonuse of digitalis, beta-blockers, and angiotensin-convert-
implanted. After 358 patients with inducible tachyarrhythmia had
ing–enzyme inhibitors at base line.
been enrolled, the protocol was changed, allowing implantation ofa defibrillator after one or more unsuccessful drug trials. Patients
who declined to undergo implantation of a defibrillator were dis-
A total of 2202 patients were enrolled from No-
charged receiving no antiarrhythmic drugs. Patients were evaluat-
vember 1, 1990, to October 31, 1996. This total in-
ed one month after discharge and every three months thereafter.
cluded 767 patients with inducible, sustained ventric-
End Points
ular tachyarrhythmia, of whom 704 agreed to undergo
The primary end point was cardiac arrest or death from arrhyth-
randomization and 63 refused but were followed in
mia. Secondary end points included death from all causes, death
the registry, and 1435 patients without inducible tach-
from cardiac causes, and spontaneous, sustained ventricular tach-ycardia. A modified Hinkle–Thaler system was used to classify
yarrhythmia (as defined by the protocol). Of the 704
deaths.11 Deaths from arrhythmia included unwitnessed deaths,
patients who underwent randomization, 351 were
witnessed instantaneous deaths, nonsudden deaths due to inces-
assigned to receive electrophysiologically guided ther-
sant tachycardia, deaths considered to be sequelae of cardiac ar-
apy and 353 were assigned to receive no antiarrhyth-
rest, deaths caused by the toxic effects of antiarrhythmic drugs, anddeaths resulting from complications of implanted defibrillators. The
mic therapy. Among the patients assigned to no an-
deaths of patients with end-stage heart failure or cardiogenic shock
tiarrhythmic therapy, 96 percent received no therapy.
were not classified as deaths from arrhythmia. Cardiac arrest was
Complications of the base-line electrophysiologic
defined as sudden loss of consciousness requiring direct-current
study occurred in five of the patients with inducible,
countershock to restore consciousness or a stable blood pressure
sustained ventricular tachyarrhythmia (0.7 percent);
and rhythm. Narrative descriptions of events and hospital recordswere edited by the data-coordinating center to ensure that the out-
none were fatal. The base-line characteristics of the
comes were classified without knowledge of treatment assignment
patients in the two groups were similar (Table 1). The
or whether tachycardia could be induced in any of the patients.
median ejection fraction was 29 percent in the group
Statistical Analysis
assigned to no antiarrhythmic therapy and 30 per-
On the basis of previous reports, we anticipated a two-year rate
cent in the group assigned to electrophysiologically
of arrhythmic events of 15 to 20 percent in the group assigned
to no antiarrhythmic therapy and a reduction of at least 33 per-cent in the rate of events in the group assigned to electrophysio-
Nonantiarrhythmic Medical Therapy
logically guided therapy. Using these rates and an alpha level of
After enrollment, 40 percent of all 704 patients
0.05, we determined that a total of 900 patients with inducible,sustained tachyarrhythmia would provide the study with more than
were discharged from the hospital receiving beta-adre-
80 percent power to detect an event rate of 15 percent and more
nergic–blocking agents. Use of beta-blockers was
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
percent; amiodarone, 10 percent; and sotalol, 9 per-
TABLE 1. CLINICAL CHARACTERISTICS OF THE PATIENTS
cent) and 161 (46 percent) were given defibrillators.
Six patients (2 percent) died while they were in thehospital. Seven percent of the patients in this group
ELECTRO-
refused antiarrhythmic therapy at various points dur-
PHYSIOLOGICALLY ANTIARRHYTHMIC
ing the study. After discharge, 17 percent of the pa-
GUIDED THERAPY VARIABLE
tients assigned to electrophysiologically guided ther-apy had a change in the type of drug therapy they
were receiving and 12 percent switched from antiar-
rhythmic drugs to a defibrillator. One patient treated
with a defibrillator died as a direct result of an infec-
tion complicating the revision of the lead system 18
Follow-up
Most of the patients adhered to the therapy to
which they had been assigned. At the last follow-up,
305 patients (87 percent) assigned to electrophysio-
logically guided therapy were receiving treatment.
One hundred three patients (29 percent) were receiv-
ing antiarrhythmic drugs, and 202 patients (58 per-
cent) received defibrillators. Among the patients as-
signed to no antiarrhythmic therapy, 3 percent had
received a defibrillator by the last follow-up and 10
percent had been given antiarrhythmic drugs with-
out having had cardiac arrest, sustained ventricular
tachycardia, or syncope. Atrial fibrillation was the in-
dication for antiarrhythmic drugs in 57 percent of
The median duration of follow-up was 39 months.
All but four patients were followed for two years or
*Values in parentheses are 25th and 75th percentiles; categorical vari-
more, and all but two events could be classified on the
†Data were available for 59 percent of the patients in each treatment
basis of the information that was available. Among
group. Because of rounding, not all percentages total 100. NYHA denotes
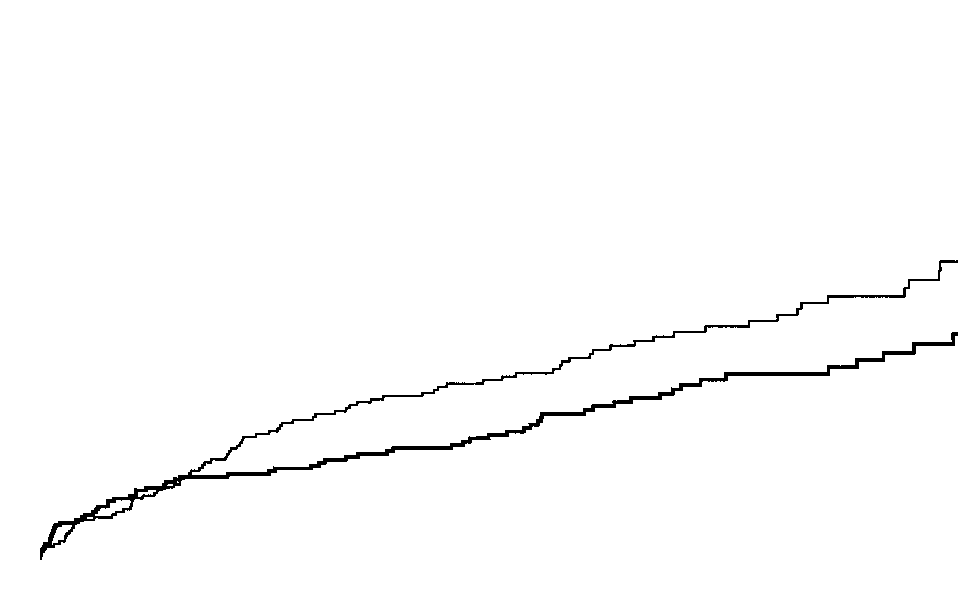
the patients assigned to no antiarrhythmic therapy,
the two-year rate of cardiac arrest or death from ar-
‡P=0.001 for the comparison with the patients assigned to no antiar-
rhythmia was 18 percent and the five-year rate was
32 percent. The corresponding rates for the patientsassigned to electrophysiologically guided therapy were12 percent and 25 percent (P=0.04 for the five-year
more frequent among the patients assigned to no an-
rates; relative risk, 0.73; 95 percent confidence inter-
tiarrhythmic therapy (Table 1). The use of antiarrhyth-
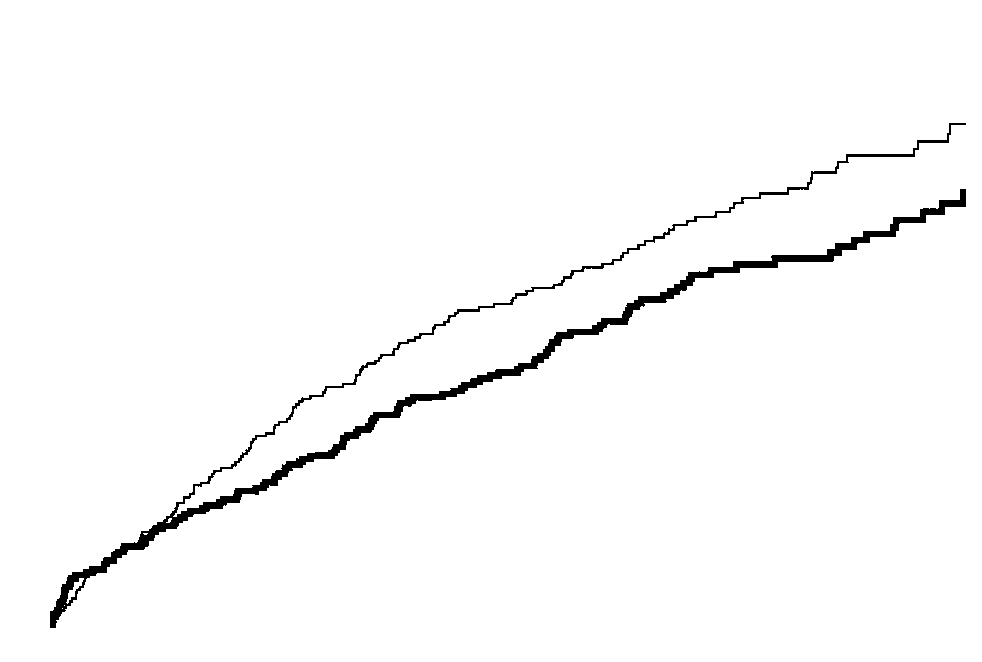
val, 0.53 to 0.99) (Fig. 1). The overall mortality rates
mic agents with beta-blocking properties accounted
after two years and after five years were 28 percent
for much of the disparity in the use of beta-blockers.
and 48 percent, respectively, for the patients assigned
In addition to the 29 percent of patients who were
to no antiarrhythmic therapy, as compared with 22
taking “pure” beta-blockers in the group assigned to
percent and 42 percent for those assigned to electro-
electrophysiologically guided therapy, 23 percent
physiologically guided therapy (P=0.06 for the five-
were taking antiarrhythmic agents with beta-block-
year rates; relative risk, 0.80; 95 percent confidence
ing properties. During follow-up, an additional 11
interval, 0.64 to 1.01) (Fig. 2). At five years, the rate
percent of the patients assigned to electrophysiolog-
of death from cardiac causes was significantly higher
ically guided therapy and 2 percent of those assigned
among the patients assigned to no antiarrhythmic
to no antiarrhythmic therapy were being treated with
therapy than among those assigned to electrophysi-
beta-blockers. The rate of use of other cardiac med-
ologically guided therapy (40 percent vs. 34 percent,
ications was similar in the two groups.
P=0.05). There was no significant difference in theincidence of spontaneous, sustained ventricular tach-
Antiarrhythmic Therapy
ycardia between the two groups (21 percent among
Among the 351 patients assigned to electrophysi-
the patients assigned to no antiarrhythmic therapy
ologically guided therapy, 158 (45 percent) were dis-
and 20 percent among those assigned to electrophys-
charged with antiarrhythmic drugs (class I agents, 26
iologically guided therapy, P=0.90). A R A N D O M I Z E D ST U DY O F T H E P R EV E N T I O N O F S U D D E N D E AT H I N PAT I E N T S W I T H C O R O N A RY A R T E RY D I S E AS E Figure 1. Kaplan–Meier Estimates of the Rates of Cardiac Arrest or Death from Arrhythmia. EPG de- notes electrophysiologically guided. Figure 2. Kaplan–Meier Estimates of the Rates of Death from All Causes. EPG denotes electrophysio- logically guided.
The lower rates of arrhythmic events among the
received a defibrillator, as compared with 37 percent
patients assigned to electrophysiologically guided
among those in this group who did not receive a de-
therapy were largely attributable to the use of defib-
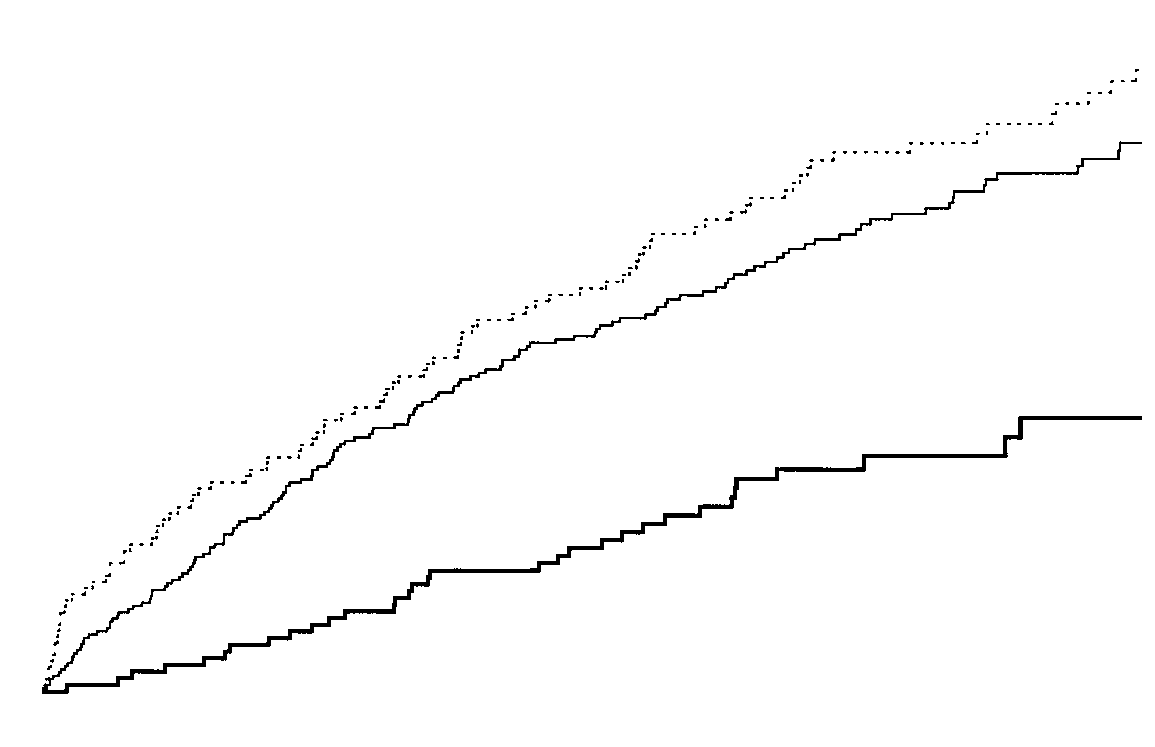
fibrillator (P<0.001) (Fig. 3). The overall mortality
rillators. The five-year rate of cardiac arrest or death
rates at five years were 24 percent among the patients
from arrhythmia was 9 percent among the patients
who received defibrillators and 55 percent among
assigned to electrophysiologically guided therapy who
those who did not (Fig. 4). The survival benefit as-
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Figure 3. Kaplan–Meier Estimates of the Rates of Cardiac Arrest or Death from Arrhythmia According to Whether the Patients Received Treatment with a Defibrillator.
The P value refers to two comparisons: between the patients in the group assigned to electrophysio-logically guided (EPG) therapy who received treatment with a defibrillator and those who did not re-ceive such treatment, and between the patients assigned to electrophysiologically guided therapy whoreceived treatment with a defibrillator and those assigned to no antiarrhythmic therapy.
Figure 4. Kaplan–Meier Estimates of the Rates of Overall Mortality According to Whether the Patients Received Treatment with a Defibrillator.
The P value refers to two comparisons: between the patients in the group assigned to electrophysio-logically guided (EPG) therapy who received treatment with a defibrillator and those who did not re-ceive such treatment, and between the patients assigned to electrophysiologically guided therapy whoreceived treatment with a defibrillator and those assigned to no antiarrhythmic therapy. A R A N D O M I Z E D ST U DY O F T H E P R EV E N T I O N O F S U D D E N D E AT H I N PAT I E N T S W I T H C O R O N A RY A R T E RY D I S E AS E TABLE 2. EFFECTS OF DEFIBRILLATOR THERAPY.* ELECTROPHYSIO- ELECTROPHYSIO- LOGICALLY GUIDED LOGICALLY GUIDED NO ANTIARRHYTH- THERAPY WITH THERAPY WITHOUT END POINT MIC THERAPY DEFIBRILLATOR DEFIBRILLATOR RELATIVE RISK OF EVENT WITH DEFIBRILLATOR THERAPY (95% CI)
0.24 (0.13–0.43) 0.24 (0.13–0.45) 0.28 (0.16–0.49) 0.27 (0.15–0.47)
0.42 (0.29–0.61) 0.40 (0.27–0.59) 0.49 (0.35–0.69) 0.45 (0.32–0.63)
*P<0.001 for both unadjusted and adjusted estimates of relative risk for each end point. CI denotes confidence interval.
sociated with defibrillator treatment remained signif-
Electrophysiologic testing has been studied to
icant (P<0.001) after Cox regression analysis, in which
predict the risk of sudden death in patients with a
adjustments were made for all available prognostic
recent myocardial infarction and in patients who have
clinical factors (Table 2). As compared with the pa-
unsustained ventricular tachycardia after myocardial
tients who were assigned to electrophysiologically
infarction. Electrophysiologic testing after a recent
guided therapy and who did not receive defibrilla-
myocardial infarction has been reported to induce
tors, those who received such treatment had an ad-
tachyarrhythmia in 9 to 20 percent of patients.19-21
justed relative risk of arrhythmic events of 0.24 (95
Arrhythmic events have occurred in 14 to 36 percent
percent confidence interval, 0.13 to 0.45), and an
of patients with inducible, sustained tachyarrhythmia
adjusted relative risk of overall mortality of 0.40 (95
over a period of one to two years.19-23 The rate of in-
percent confidence interval, 0.27 to 0.59) (Table 2).
ducible ventricular tachyarrhythmia was higher in ourstudy, suggesting that the presence of a reduced
DISCUSSION
ejection fraction and unsustained ventricular tachy-
We found that the risk of cardiac arrest or sudden
cardia identifies patients who are more likely to have
death was substantial among patients with coronary
inducible tachyarrhythmia. The median time from
artery disease, a left ventricular ejection fraction of
acute myocardial infarction to enrollment in the cur-
40 percent or less, spontaneous, unsustained ventric-
rent trial was longer than in the previous studies, but
ular tachycardia, and sustained tachyarrhythmia in-
there was no effect of the length of time between
duced by programmed stimulation. Antiarrhythmic
myocardial infarction and enrollment on whether
therapy guided by the results of electrophysiologic
sustained ventricular tachyarrhythmia could be in-
testing led to an absolute reduction in the risk of
duced.24 The rate of cardiac arrest or death from ar-
cardiac arrest or death from arrhythmia of 7 percent
rhythmia in the group that was assigned to no anti-
after five years of follow-up. The survival benefit as-
arrhythmic therapy (18 percent at two years) was
sociated with electrophysiologically guided therapy
similar to the rates in the earlier studies, in which use
was due solely to the use of defibrillators, not to an-
of antiarrhythmic drugs was variable.19-23 The high
tiarrhythmic drugs. Defibrillators not only reduced
rate of arrhythmic events observed in our study is re-
the risks of cardiac arrest and sudden death from ar-
markable, given that the median time between myo-
rhythmia, but also improved overall survival.
cardial infarction and enrollment was 39 months.
The study included a diverse group of patients
Inducible sustained tachyarrhythmia in patients
from many study sites throughout the United States
presenting with unsustained ventricular tachycardia
and Canada, including private practices not affiliated
and chronic coronary disease has previously been ob-
with a university, medical schools, and Veterans Af-
served in 20 to 45 percent of cases, a finding similar
fairs hospitals. The electrocardiographic characteris-
to the rate of 35 percent that we observed.25-28 Pre-
tics of the patients with unsustained ventricular tach-
vious studies reported rates of arrhythmic events of
ycardia were virtually identical to those of patients
11 to 88 percent over a period of 14 to 30 months
enrolled in the Cardiac Arrhythmia Suppression Tri-
among patients with inducible tachycardia. None of
al.17,18 Thus, in this regard, the patients enrolled in
these earlier reports systematically included untreat-
our trial were representative of all patients with un-
ed patients. Our study demonstrated a risk of cardiac
sustained ventricular tachycardia after myocardial
arrest or death from arrhythmia of 18 percent among
patients with inducible sustained tachyarrhythmia
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
when no antiarrhythmic therapy was administered
than three years after myocardial infarction are un-
clear. The electrophysiologists participating in the
The rate of response to antiarrhythmic drugs in
study were not the patients’ primary cardiologists in
our study, as ascertained by electrophysiologic test-
many cases, and there was widespread reluctance
ing, is consistent with the rates reported in previous
among primary physicians to administer beta-block-
studies.23-26 Such a response did not translate into a
ing agents to patients with markedly abnormal left
reduction in the risk of cardiac arrest or death from
arrhythmia. In fact, the survival benefit associated with
The primary end point in this trial was cardiac arrest
electrophysiologically guided therapy was due to the
or death from arrhythmia — which, as used in this
use of defibrillators. The patients who received de-
study, meant instantaneous or unwitnessed death, ex-
fibrillators had at least one unsuccessful antiarrhyth-
cept in the case of patients who died of incessant ven-
mic-drug test, suggesting that they might have had a
tricular tachycardia or complications of antiarrhythmic
poorer prognosis than those who did not receive de-
therapy. We use this category for terminal events, but
fibrillators. However, the patients who received defib-
we can make no claim as to the mechanism by which
rillators had better rates of survival than those who did
such deaths occur. It is likely that some sudden deaths
not receive such treatment. Previous studies have dem-
were due to acute ischemic events. We tried to mini-
onstrated that empirical antiarrhythmic-drug therapy
mize this possibility by requiring evaluation and appro-
and therapy guided by the results of Holter moni-
priate therapy for myocardial ischemia before patients
toring do not improve survival after myocardial in-
were enrolled. In addition, the proportion of arrhyth-
farction.29-32 Our study demonstrates that antiarrhyth-
mias mediated by ischemia should have been rough-
mic-drug therapy guided by electrophysiologic testing
ly equal between the treated and untreated groups.
The patients assigned to electrophysiologically
The reasons for the failure of this approach to im-
guided therapy were not randomly assigned to drug
prove survival are not clear. The criteria we used to
therapy or defibrillator therapy. Thus, although the
ascertain drug response by electrophysiologic tests
reductions in the relative risk of arrhythmic events
may have been inadequate.33 Daily variability in the
and overall mortality in patients treated with defib-
inducibility of tachycardia may result in false predic-
rillators are large, caution should be used in inter-
tions of drug efficacy. The inconsistency of the effects
preting the true magnitude of the benefit. Extensive
of antiarrhythmic drugs (possibly owing to noncom-
analyses in which adjustments were made for poten-
pliance) may contribute. Finally, progression of dis-
tial prognostic factors that could have influenced
ease over the course of the trial may have altered the
outcome still demonstrate better survival among the
patients’ responsiveness to the drugs.
patients given defibrillators than among those given
The Multicenter Automatic Defibrillator Implan-
drugs. This trial was not designed to test the efficacy
tation Trial examined the efficacy of defibrillators in
of individual antiarrhythmic agents but rather the
preventing sudden death in patients similar to those
usefulness of electrophysiologic testing to guide an-
enrolled in our trial.34 That small study (involving 196
tiarrhythmic therapy. Most patients discharged re-
patients) lacked a control group of untreated patients
ceiving antiarrhythmic drugs were treated with class
and involved an average follow-up period of only 27
I agents. It is not clear whether greater use of class
months. The two-year mortality of 32 percent among
III agents would have improved outcomes among
the patients treated with antiarrhythmic drugs (pri-
the patients treated with antiarrhythmic drugs.
marily empirical therapy with amiodarone) in that
The results of this study establish that patients
study was slightly higher than the two-year mortality
with coronary disease, an ejection fraction of 40 per-
among our untreated patients (28 percent), but sim-
cent or less, asymptomatic, unsustained ventricular
ilar to the mortality among the patients in our study
tachycardia, and inducible sustained ventricular tach-
who were assigned to electrophysiologically guided
yarrhythmia have substantial mortality due to arrhyth-
therapy and who did not receive defibrillators (33
mia. The rate of death among patients with induc-
percent). The two-year mortality among the patients
ible sustained tachyarrhythmia is reduced by the use
who received defibrillators was similar in both trials
of defibrillators but not by the use of antiarrhythmic-
— approximately 10 percent. These similarities in
drug therapy based on the results of electrophysio-
survival are noteworthy, especially since the rate of
logic testing. Thus, it is reasonable to perform elec-
beta-blocker use among the patients in our trial was
trophysiologic testing in patients who meet the entry
about twice that of the patients in the earlier study.
criteria of this trial. If sustained ventricular tachyar-
Beta-blockers and angiotensin-converting–enzyme
rhythmia can be induced in a clinical setting similar
inhibitors have been proved to reduce mortality in
to that of this study, implantation of a defibrillator
patient populations similar to ours. Our patient pop-
is warranted. Further studies are necessary to clarify
ulation, with a median ejection fraction of approxi-
the mechanisms that cause sudden death among pa-
mately 29 percent, should benefit from both types
tients with coronary disease and to permit the devel-
of drugs. However, the benefits of beta-blockers more
opment of improved, less costly treatments. A R A N D O M I Z E D ST U DY O F T H E P R EV E N T I O N O F S U D D E N D E AT H I N PAT I E N T S W I T H C O R O N A RY A R T E RY D I S E AS E
Supported by grants from the National Heart, Lung, and Blood Insti-
Heezen; Illinois Masonic Medical Center, Chicago: R. Kehoe, S. Crandall,
tute (UO1 HL45700 and UO1 HL45726), C.R. Bard, Berlex Laborato-
L. Farwell; University of Alabama at Birmingham, Birmingham: S. Dailey,
ries, Boehringer–Ingelheim Pharmaceuticals, Guidant–Cardiac Pacemak-
R. Bubien, C. Tidwell; St. Francis Medical Center, Pittsburgh: A. Ticzon,
ers, Knoll Pharmaceutical, Medtronic, Searle, Ventritex–St. Jude Medical,
C. DiGiocomo, L. Predis; University of New Mexico Health Science Center,Albuquerque: G.M. Greenberg, R.M. Cataldo, T. Hudson, L. Beeman; Vet-erans Affairs Medical Center, Ann Arbor, Mich.: W. Kou, D. Randall; Uni-APPENDIX versity of Florida, Gainesville: A.B. Curtis, M. Mardis, M. LaTour; StatenIsland University Hospital, Staten Island, N.Y.: S. Bekheit-Saad, M.L.
In addition to the authors, the following persons and institutions partic-
Brezsnyak, A.V. Porter, H. Walsh; North Shore University Hospital, Manhas-
ipated in the trial: Michigan Heart, Ann Arbor: L. DiCarlo, S. Winston, D. set, N.Y.: R. Jadonath, T. Cohen, B. Goldner, D. Kalenderian, L. Chepurko;
Myers; University of Maryland, Baltimore: M.R. Gold, S. Shorofsky, R. Pe-
Heart Center, Sarasota, Fla.: W. Hepp, M. Healy, H. Taylor; Wichita Insti-
ters, D. Froman, H. Scott; Arkansas Cardiology Clinic, Little Rock: G.S. tute for Clinical Research, Wichita, Kans.: G. Turitto, J.E. Val-Mejias, D. Klo-
Greer, J. Daly; Temple University Hospital School of Medicine, Philadelphia:
nis, P. Patterson; St. Vincent Medical Center, Toledo, Ohio: S. Brownstein,
J.M. Miller, H.H. Hsia, S.A. Rothman, G. Harper, L. Siddoway, S. Zuker-
V. Duthinh, J. Morris, R. Oberhaus; Clearwater Cardiovascular Consult-
man, D. Whitley, C. Slater, M. Gastineau, J. Edinger, D. Ackerman, N. ants, Largo, Fla.: J. Gallastegui, K. Livingston; Medical Center of Delaware,
Bowe; Northside Cardiology, Indianapolis: J. Evans, L. Jacobs, L. Janeira,
Newark: H. Weiner, R. Vitullo, A. DiSabitino, S. Feehs; University of Vir-
M. Markel, R.I. Fogel; Midwest Heart Research Foundation, Lombard, Ill.:ginia Medical School, Charlottesville: J. DiMarco, S. Thompson; New York
M.F. O’Toole, M.O. Nora, E. Enger, J. Gurgone, K. Treckler; University ofHospital–Cornell Medical Center, New York: B. Lerman, M. Sarmiento;
Ottawa Heart Institute, Ottawa, Ont., Canada: A. Tang, M. Green, C. Cardiology Care Specialists, Allentown, Pa.: L. Constantin, C. Kern, C.
Carey; University of Pennsylvania, Philadelphia: M. Hanna, N. Britton, K.
Fedak; University of Pittsburgh, Pittsburgh: K. Anderson, S. Fahrig, B. Mik-
Gephardt, L. Goffredo; Montefiore Medical Center, Bronx, N.Y.: K. Ferrick,
los; Robert Wood Johnson Medical School, New Brunswick, N.J.: M. Prem-
S. Kim, J. Roth, L. Chinitz, T. Glotzer, A. Ferrick, J. Durkin; Columbia
inger, N. Cosgrove; Carle Clinic Association, Urbana, Ill.: A. Kocherill, J. University, New York: J. Coromilas, J. Zimmerman, K. Hickey, J. Reiffel, F.
Shane, S. Lofrano; and Mid-Florida Cardiology Specialists, Orlando, Fla.:
Livelli; Montreal Heart Institute, Montreal: M. Talajic, D. Roy, M. Dubuc,
M. Hazday, L. Jopperi. Executive Committee: A.E. Buxton, K.L. Lee
B. Thibault, D. Beaudoin, J. Marquis; Electrophysiology Consultants, Detroit:
(principal investigators), J.D. Fisher, M.E. Josephson, E.N. Prystowsky, L.
M.H. Lehmann, R.T. Steinman, J.J. Baga, L.A. Pires, C.D. Schuger, D.
Dicarlo, D. Echt, G.S. Greer, D. Packer, M. Talajic, and D. Pryor (until
Frankovich, J. Fresard; Southern New Hampshire Cardiology Center,
1994); Events Committee: J.D. Fisher (chair), P. Denes, J. DiMarco, D. Manchester: B. Hook, L. Brown; Cardiology Associates, Johnson City, N.Y.:
Echt, M. Lehmann, D. Packer, and D. Roy; Data Coordinating Center:
N. Stamato, D. Whiting; Tulane University School of Medicine, New Orleans:
Duke Clinical Research Institute, Durham, N.C. — K.L. Lee (director),
M. Prior, J. Talano, N. Wicker; Mayo Foundation, Rochester, Minn.: D. Pack-
G. Hafley, K. Pieper, and G. Marcucci (statisticians), S. Cress (data man-
er, S.C. Hammil, C. Stevens; Thoracic and Cardiovascular Institute, Lan-
ager), V. Christian, J. Wehbie, T. Gentry, E. Rives, J. Spittler, and L. Wood-
sing, Mich.: J.H. Ip, D. Grimes, T. Magnum, B. McAndrews; Vanderbilt
lief (project coordinators); P. Smith, J. Wood, M. Palcisko, and G. Esposito
University, Nashville: D. Echt, D. Roden, N. Conners; New York Medical
(nurse monitors); Consultant — J. Mason; National Heart, Lung, and College, White Plains: D.A. Rubin, C. Sorbera, A. McAllister; Hôpital duBlood Institute: M. Domanski (project officer), M. Proschan (statisti- Sacré-Coeur de Montréal, Montreal: T. Kus, R. Nadeau, G. Gaudette, J. Fou-
cian); Data and Safety Monitoring Board: B. Chaitman (chair), K.
quette; Lancaster Heart Foundation, Lancaster, Pa.: S. Worley, G. Rubright,
Bailey, B. Brody, J. Cohn, H.L. Greene, A. Hallstrom, and R. Lazzara.
J. Tuzi, K. Knepper; Yale University, New Haven, Conn.: W.P. Batsford, C. McPherson, A. Van Zetta, G. Elwood; University of Texas SouthwesternREFERENCES Medical Center, Dallas: R.L. Page, J.A. Joglar, G. Erwin, L. Nelson; St. Luke’s Hospital, Kansas City, Mo.: R. Lemery, D. Steinhaus, D. Cardinale;
1. Tavazzi L, Volpi A. Remarks about postinfarction prognosis in light of Hoag Memorial Hospital–Presbyterian Medical Center, Newport Beach, Cal-
the experience with the Gruppo Italiano per lo Studio della Sopravvivenza
if.: B. Kennelly, G. Mirabal, K. Porter; University of Calgary, Calgary, Al-
nell’ Infarto Miocardico (GISSI) trials. Circulation 1997;95:1341-5. ta., Canada: D.G. Wyse, H.J. Duff, A.M. Gillis, L.B. Mitchell, J.M. Roth-
2. Rouleau JL, Talajic M, Sussex B, et al. Myocardial infarction patients in
schild, R.S. Sheldon, J. Kellen, D. Ritchie, B. Baptie, L. Bracken; Audubon
the 1990s — their risk factors, stratification and survival in Canada: the Ca-
Regional Medical Center, Louisville, Ky.: J.M. Kammerling, V. Payne, J.
nadian Assessment of Myocardial Infarction (CAMI) Study. J Am Coll
Hanrahan; Albany Medical College, Albany, N.Y.: A. Portnow, J. Nattama,
D. O’Dea, C. Ocampo, I. Megas-Nowak; University of Connecticut Health3. Simoons ML, Vos J, Tijssen JGP, et al. Long-term benefit of early Center, Farmington: E. Berns, M.B. Barry, L. Kearney, P. Stefanow, P. Ma-
thrombolytic therapy in patients with acute myocardial infarction: 5 year
lone; Mt. Sinai Medical Center, New York: J.A. Gomes, S.L. Winters, E. Pe;
follow-up of a trial conducted by the Interuniversity Cardiology Institute
Sentara Norfolk General Hospital, Norfolk, Va.: R.C. Bernstein, J.M. Herre,
of the Netherlands. J Am Coll Cardiol 1989;14:1609-15.
J. Onufer, L. McGowan, L. Klevan, C. Townsend; University of Massachu-4. Cerqueira MD, Maynard C, Ritchie JL, Davis KB, Kennedy JW. setts, Worcester: R.S. Mittleman, S.K.S. Huang, A.B. Wagshal, K.A. Rofino,
Long-term survival in 618 patients from the Western Washington Strepto-
K. Rofino; Cooper Hospital–University Medical Center, Camden, N.J.: A.M.
kinase in Myocardial Infarction trials. J Am Coll Cardiol 1992;20:1452-9.
Russo, H. Waxman, C. Stubin, T. Meehan; Cardiology Foundation of Lan-5. de Vreede-Swagemakers JJM, Gorgels APM, Dubois-Arbouw WI, et al. kenau Hospital, Wynnewood, Pa.: P. Kowey, R.A. Marinchak, S.J. Rials,
Out-of-hospital cardiac arrest in the 1990s: a population-based study in the
A.R. Chikowski, H. Criner; State University of New York Health Science
Maastricht area on incidence, characteristics and survival. J Am Coll Car-
Center, Brooklyn: N. El-Sherif, G. Turitto, L. Knudson; Sutter Institute forMedical Research, Sacramento, Calif.: G. O’Neill, A. Sharma, A. Skadsen;
6. The Antiarrhythmics versus Implantable Defibrillators (AVID) Investi- Pepin Heart and Vascular Institute, Tampa, Fla.: C. Machado, S. Mester,
gators. A comparison of antiarrhythmic-drug therapy with implantable de-
C. Sullivan; West Virginia University, Morgantown: S.B. Schmidt; Cardiac
fibrillators in patients resuscitated from near-fatal ventricular arrhythmias.
Disease Specialists, Atlanta: T. Deering, S. Holt; Rockford ElectrophysiologyConsultants, Rockford, Ill.: M. Hiser, T. Pham, E. Silva, P. Dittmar; Iowa7. Liberthson RR , Nagel EL, Hirschman JC, Nussenfeld SR. Prehospital Heart Center, Des Moines: W.B. Johnson, M. Core-Bier, T. Coulson; Rhode
ventricular defibrillation: prognosis and follow-up course. N Engl J Med
Island Hospital, Providence: R. Lemery, E. Berger, C.A. Chmielewski, D.
Badger, E. Connolly; Presbyterian Hospital of Dallas, Dallas: J. Hurwitz, B. 8. Weaver WD, Hill D, Fahrenbruch CE, et al. Use of the automatic ex-
Wimberly, D. Capper; Veterans Affairs Medical Center, Washington, D.C.:
ternal defibrillator in the management of out-of-hospital cardiac arrest.
S. Singh, R. Fletcher, R. Woosley, D. Byrns, B. Bennett; Duke UniversityMedical Center, Durham, N.C.: R.A. Greenfield, H. Daniels, C. Grill; Uni-9. Becker LB, Han BH, Meyer PM, et al. Racial differences in the incidence versity of Louisville School of Medicine, Louisville, Ky.: I. Singer, S. Blair, A.
of cardiac arrest and subsequent survival. N Engl J Med 1993;329:600-6.
Cicic; University of Nebraska Medical Center, Omaha: J. Windle, W. Baring-
10. Buxton AE, Fisher JD, Josephson ME, et al. Prevention of sudden
ton, A. Easley, L. Smith; Beth Israel Deaconess Medical Center, Boston: M.E.
death in patients with coronary artery disease: the Multicenter Unsustained
Josephson, R. Bayer, V. Schreckengost; Washington University, St. Louis:
Tachycardia Trial (MUSTT). Prog Cardiovasc Dis 1993;36:215-26.
M.E. Cain, J. Osborn; Sinai Hospital of Baltimore, Baltimore: J. Reilly, D.J. 11. Hinkle LE Jr, Thaler HT. Clinical classification of cardiac deaths. Cir-
Schamp, V. O’Mara; Maine Medical Center, Portland: J. Cutler, J. Love, C.
Berg; Medical Center Hospital of Vermont, Burlington: M.A. Capeless, M. 12. Kaplan EL, Meier P. Nonparametric estimation from incomplete ob-
Rowen; Virginia Commonwealth University, Richmond: M. Wood, K. El-
servations. J Am Stat Assoc 1958;53:457-81.
lenbogen, B. Stambler, R. Sperry, M. Belz, V. Gillock, C. Dietrich, N. 13. Cox DR. Regression models and life-tables. J R Stat Soc [B] 1972;34:
Michaels, D. Sargent; Cardiology of Tulsa, Tulsa, Okla.: J. Swartz, D.W. Fra-
zier, W.O. Adkisson, R.D. Ensley, S. Dewald, L. Klahr; Riverside Regional14. Kalbfleisch JD, Prentice RL. The statistical analysis of failure time da- Medical Center, Newport News, Va.: A. Murphy, S. Gessner, M. Barton, L.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
15. O’Brien PC, Fleming TR. A multiple testing procedure for clinical tri- 25. Gomes JAC, Hariman RI, Kang PS, El-Sherif N, Chowdhry I, Lyons J.
Programmed electrical stimulation in patients with high-grade ventricular
16. Lan KKG, DeMets DL. Discrete sequential boundaries for clinical tri-
ectopy: electrophysiologic findings and prognosis for survival. Circulation
17. Buxton AE, Lee KL, DiCarlo L, et al. Nonsustained ventricular tachy- 26. Buxton AE, Marchlinski FE, Flores BT, Miller JM, Doherty JU, Jo-
cardia in coronary artery disease: relation to inducible sustained ventricular
sephson ME. Nonsustained ventricular tachyarrhythmia in patients with
tachycardia. Ann Intern Med 1996;125:35-9.
coronary artery disease: role of electrophysiologic study. Circulation 1987;
18. Denes P, Gillis AM, Pawitan Y, Kammerling JM, Wilhelmsen L, Sa-
lerno DM. Prevalence, characteristics and significance of ventricular prema-
27. Klein RC, Machell C. Use of electrophysiologic testing in patients with
ture complexes and ventricular tachycardia detected by 24-hour continuous
nonsustained ventricular tachycardia: prognostic and therapeutic implica-
electrocardiographic recording in the Cardiac Arrhythmia Suppression Tri-
tions. J Am Coll Cardiol 1989;14:155-61. 28. Wilber DJ, Olshansky B, Moran JF, Scanlon PJ. Electrophysiological 19. Denniss AR , Richards DA, Cody DV, et al. Prognostic significance of
testing and nonsustained ventricular tachycardia: use and limitations in pa-
ventricular tachycardia and fibrillation induced at programmed stimulation
tients with coronary artery disease and impaired ventricular function. Cir-
and delayed potentials detected on the signal-averaged electrocardiograms
of survivors of acute myocardial infarction. Circulation 1986;74:731-45. 29. Hine WK, Laird NM, Hewitt P, Chalmers TC. Meta-analysis of em- 20. Richards D, Taylor A, Fahey P, et al. Identification of patients at risk
pirical long-term antiarrhythmic therapy after myocardial infarction. JAMA
of sudden death after myocardial infarction: the continued Australian ex-
perience. In: Brugada P, Wellens HJJ, eds. Cardiac arrhythmias: where to
30. Julian DG, Camm AJ, Frangin G, et al. Randomised trial of effect of
go from here? Mount Kisco, N.Y.: Futura Publishing, 1987:329-41.
amiodarone on mortality in patients with left-ventricular dysfunction after
21. Roy D, Marchand E, Theroux P, Waters DD, Pelletier GB, Bourassa
recent myocardial infarction: EMIAT. Lancet 1997;349:667-74. [Errata,
MG. Programmed ventricular stimulation in survivors of an acute myocar-
dial infarction. Circulation 1985;72:487-94. 31. Cairns JA, Connolly SJ, Roberts R , Gent M. Randomised trial of out- 22. Iesaka Y, Nogami A, Aonuma K, et al. Prognostic significance of sus-
come after myocardial infarction in patients with frequent or repetitive ven-
tained monomorphic ventricular tachycardia induced by programmed ven-
tricular premature depolarisations: CAMIAT. Lancet 1997;349:675-82.
tricular stimulation using up to triple extrastimuli in survivors of acute my-
ocardial infarction. Am J Cardiol 1990;65:1057-63. 32. Echt DS, Liebson PR , Mitchell LB, et al. Mortality and morbidity in 23. Bourke JP, Richards DA, Ross DL, Wallace EM, McGuire MA, Uther
patients receiving encainide, flecainide, or placebo: the Cardiac Arrhythmia
JB. Routine programmed electrical stimulation in survivors of acute myo-
Suppression Trial. N Engl J Med 1991;324:781-8.
cardial infarction for prediction of spontaneous ventricular tachyarrhyth-
33. Mitchell LB, Sheldon RS, Gillis AM, et al. Definition of predicted ef-
mias during follow-up: results, optimal stimulation protocol and cost-
fective antiarrhythmic drug therapy for ventricular tachyarrhythmias by the
effective screening. J Am Coll Cardiol 1991;18:780-8.
electrophysiologic study approach: randomized comparison of patient re-
24. Buxton AE, Hafley GE, Lehmann MH, et al. Prediction of sustained
sponse criteria. J Am Coll Cardiol 1997;30:1346-53.
ventricular tachycardia inducible by programmed stimulation in patients
34. Moss AJ, Hall WJ, Cannom DS, et al. Improved survival with an im-
with coronary artery disease: utility of clinical variables. Circulation 1999;
planted defibrillator in patients with coronary disease at high risk for ven-
tricular arrhythmia. N Engl J Med 1996;335:1933-40.
ELECTRONIC ACCESS TO THE JOURNAL’ S CUMULATIVE INDEX
At the Journal’s site on the World Wide Web (http://www.nejm.org) you can search anindex of all articles published since January 1990. You can search by author, subject, title,type of article, or date. The results will include the citations for the articles plus links to theabstracts of articles published since 1993. Single articles and past issues of the Journal canalso be ordered for a fee through the Internet (http://www.nejm.org /customer/).
(Rev. Esp. Anestesiol. Reanim. 2005; 52: 109-114) CASO CLÍNICO Tratamiento con radiofrecuencia pulsada en dos casos de neuralgiaglosofaríngea idiopática y secundaria. Resultados preliminaresD. Abejón*, S. García del Valle**, C. Nieto*, C. Delgado***, J. I. Gómez-Arnau****Área de Anestesia, Reanimación y Cuidados Críticos. Unidad de Dolor. Fundación Hospital Alcorcón. Alcorcón. Madr
Contents 1. Introduction 2. Acupuncture and Fertility Management 2.1 Fertility Management without assisted conception 2.1.1 Female benefits 2.1.2 Male Benefits 2.2 Assisted Reproductive Techniques 2.2.1 Effects when performed on day of embryo transfer 2.3 Psychological Impact on Patients undergoing ART 3. Gynecological Problems 3.1 Polycystic Ovary
 A R A N D O M I Z E D ST U DY O F T H E P R EV E N T I O N O F S U D D E N D E AT H I N PAT I E N T S W I T H C O R O N A RY A R T E RY D I S E AS E
A R A N D O M I Z E D ST U DY O F T H E P R EV E N T I O N O F S U D D E N D E AT H I N PAT I E N T S W I T H C O R O N A RY A R T E RY D I S E AS E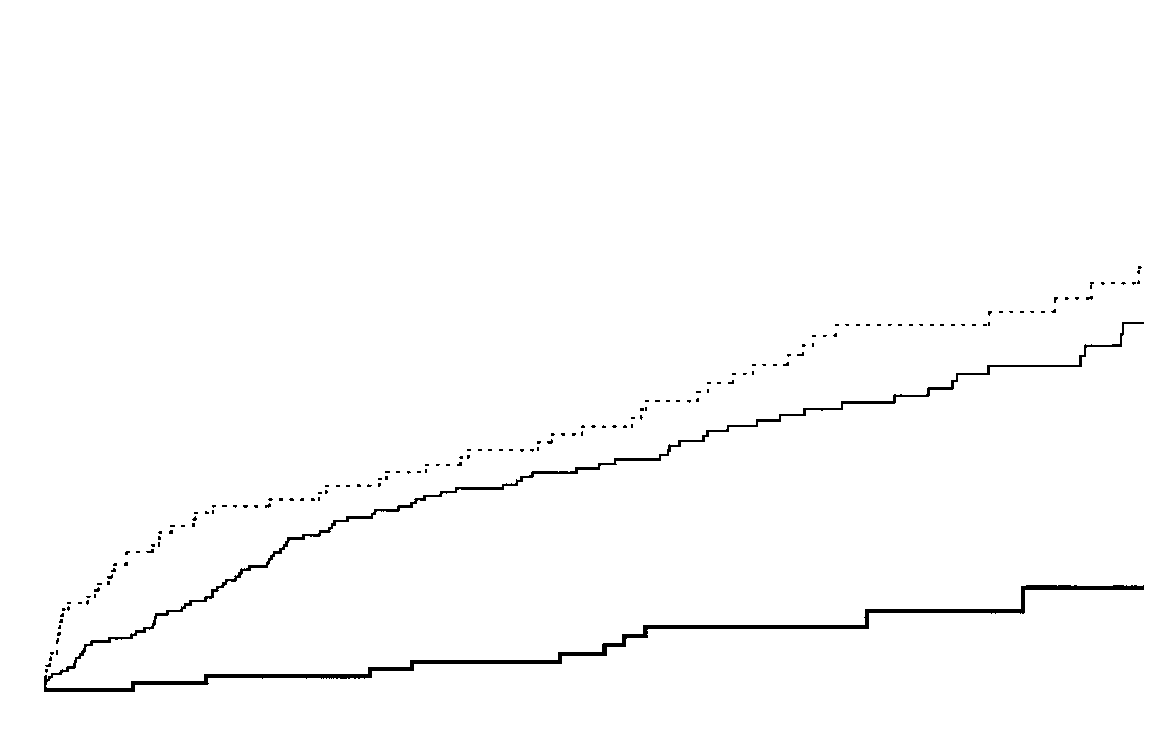
 The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Figure 3. Kaplan–Meier Estimates of the Rates of Cardiac Arrest or Death from Arrhythmia According
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Figure 3. Kaplan–Meier Estimates of the Rates of Cardiac Arrest or Death from Arrhythmia According