Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Untitled
British Medical Bulletin Advance Access published July 11, 2007
Repetitive shock wave therapy for lateralelbow tendinopathy (tennis elbow): asystematic and qualitative analysis
†OrthoTrauma Evaluation Center, Hans-Zoeller-Str. 83, D-55130 Mainz, Germany, and‡Department of Trauma and Orthopaedic Surgery, Keele University School of Medicine,Thornburrow Drive, Hartshill, Stoke on Trent, ST4 7QB Staffordshire, UK
Objective: Pooled meta-analyses of statistically and clinically heterogeneous dataof randomised-controlled studies are difficult to interpret. Therefore, aqualitative study-by-study assessment was thought to be of greater relevance, tophysicians confronted with a therapy-resistant tennis elbow patient, todetermine the effectiveness of shock wave therapy (SWT) for lateral elbowtendinopathy.
Methods: Randomized trials were identified from a current search of TheCochrane Bone, Joint and Muscle Trauma Group specialized register of trials, theCochrane Central Register of Controlled Trials, MEDLINE and reference lists ofarticles and dissertations. We included 10 trials that randomized 948 participantsto SWT or placebo or treatment control. For each trial, two independentreviewers assessed the methodological quality and extracted data. Methodological quality criteria included appropriate randomization, allocationconcealment, blinding, number lost to follow-up and intention-to-treat analysis.
Results: Conflicting results of the 10 studies were found. There was considerableheterogeneity in terms of methodological quality; treatment regimen; patientselection and follow-up period, precluding pooled analyses. Instead, individualtrial results were described in the text. Only six trials had a high-qualitymethodology. Two independent high-quality randomized placebo-controlledtrials (196 participants) reported significant success of SWT over placebo(65 versus 28%; 61 versus 29%). Design of both trials included enrolment ofchronic recalcitrant patients only; 1500 – 2000 shocks of low-energy flux density(0.1 mJ/mm2) applied to the site of maximal discomfort (clinical focusing) in
weekly intervals; no use of local anaesthesia and main follow-up at least
3 months after the last application. Three other independent high-quality trials
(406 participants) did not find any benefit of SWT over placebo (32 versus 33%;
35 versus 34%; 39 versus 31%). In these three trials, study designs deviated from
the design described earlier, enrolling acute patients or applying SWT under
& The Author 2007. Published by Oxford University Press.
All rights reserved. For permissions, please e-mail: [email protected]
local anaesthesia or expanding the application intervals to 4 weeks, whilereducing the main follow-up to 4 weeks.
Conclusions: With current studies heterogeneous in terms of the duration of thedisorder; type, frequency and total dose of SWT; period of time between SWT;type of management and control group; timing of follow-up and outcomesassessed, a pooled meta-analysis of SWT for lateral elbow tendinopathy wasconsidered inappropriate. In a qualitative systematic per-study analysisidentifying common and diverging details of 10 randomized-controlled trials,evidence was found for effectiveness of shock wave treatment for tennis elbowunder well-defined, restrictive conditions only.
Keywords: lateral elbow tendinopathy/tennis elbow/shock wave treatment/qualitative analysis
With an incidence of $1% per 1000 patients per year and a prevalenceof 1 –3% of adults per year, tennis elbow is one of the most often diag-nosed pathology of the upper extremity.1 – 7 New research shows thatthe typical histological pattern of an angiofibroblastic proliferation ismore characteristic of a failed healing response rather than of aninflammatory process.1,5,8–12
Although tennis elbow is more prevalent, few of the treatments used
rest on scientific evidence and none has been proved more effectivethan the others.13 –25
Low-energy shock wave therapy (SWT) to address the failed healing
response of a tendon is not widely known among the medical commu-nity. The rationale for its clinical use being stimulation of soft tissuehealing and inhibition of pain receptors, and hence, SWT has beenthoroughly investigated experimentally during the past decade.
To determine its clinical effectiveness and safety for lateral elbow
pain in the frame of a meta-analysis, Buchbinder et al.26 searchedvarious registers. They included nine trials that randomized 1006 par-ticipants to SWT or control and one trial that randomized 93 partici-pants to SWT or steroid injection. Results of the nine controlled trialsdiffered, as did patient selection, treatment regimen, outcome assess-ment and main follow-up period. When available data from those trialswere pooled, they found ‘platinum’ level evidence that SWT providedlittle or no benefit in terms of pain and function in lateral elbow pain.3
A meta-analysis, however, cannot improve the quality or reporting of
the original studies. Other limitations come from misapplications ofthe method, such as when study diversity is ignored or mishandled in theanalysis or when the variability of patient populations, the quality of the
Repetitive SWT for lateral elbow tendinopathy
data and the potential for underlying biases are not addressed. If relevantvalid data are statistically and clinically too heterogeneous, ameta-analysis should be avoided and reviewers should perform a qualitat-ive review in a systematic manner.3,27 Following the QUOROM rec-ommendations,28 a checklist organized into 21 headings and subheadingswas used to gather information on items such as search methodology,study selection, data abstraction, study characteristics and data analysis.
As described by Buchbinder et al.,26 randomized trials were identifiedfrom a current search of The Cochrane Bone, Joint and MuscleTrauma Group specialized register of trials (December 2006), theCochrane Central Register of Controlled Trials (The Cochrane Library,2006), MEDLINE (from 1966 to December 2006) and reference listsof articles and dissertations. Only English, French and Germanlanguage publications were considered. Further citations were soughtfrom the reference sections of papers retrieved and from contactingexperts in the field to identify studies ‘in the pipeline’.
The following search strategy was used to search. It was decided to
include search terms for specific interventions. The reference lists of allidentified studies and correspondence relating to those studies werealso searched:
Shock wave therapy or shockwave therapy or shock wave treatment;
AND tennis elbow or elbow pain or epicondylitis;
Table 1 Summary of the search strategy used and the number of hits for eachitem and total.
Two reviewers independently reviewed the identified trials to deter-
mine those that met the inclusion criteria. Full articles describing trialswere obtained and the same two reviewers independently applied theselection criteria to the studies. Only trials reporting repetitive SWTwere included. There was complete consensus concerning the finalinclusion of randomized controlled trial (RCTs).
The methodological quality of each RCT was independently assessedby two reviewers. It was planned to use consensus to resolve disagree-ments with a third reviewer to be consulted if disagreements persisted;however, there were no disagreements.
As proposed by Buchbinder et al.,26 the methodological quality of
included trials was assessed on the basis of whether the trials met keycriteria (appropriate randomization, allocation concealment, blinding,number lost to follow-up and intention-to-treat analysis). Allocationconcealment was ranked adequate, unclear or inadequate.
Two reviewers independently extracted the data on the study character-istics including source of funding, study population, intervention, ana-lyses and outcomes using standardized data extraction forms.26,28
In order to assess efficacy, raw data for outcomes of interest (mean
values and standard deviations for continuous outcomes and numberof events for binary outcomes) were extracted where available in thepublished reports.
The studies were first assessed for clinical heterogeneity with respect tothe disease severity of participants (acute versus chronic); type of SWTdevice (electromagnetic versus radial versus multiple); dose or intensityof the intervention (energy flux density: low energy versus high energy,number of impulses of SWT, number of applications: single versusrepetitive, application intervals: weekly versus monthly, SWT withversus without local anaesthesia); definition of outcome and assess-ment; control group and main follow-up (1 month versus .3 months).
All studies differed in various variables. The decision not to combine
the studies in a meta-analysis was based on the setting, participants,interventions and outcomes of the included trials (great clinical diver-sity) and on the methods used to perform the trial varying in a way
Repetitive SWT for lateral elbow tendinopathy
that was likely to overly influence the results (great methodologicaldiversity). The studies were therefore not combined in a pooled analy-sis, but described separately.
This review identified six placebo-controlled trials involving 60, 271,74, 114, 78 and 75 participants, respectively.29 –34 Two trials involving100 and 62 patients compared a standard SWT concept with a low-number application.35,36 One trial, involving 93 participants, of SWTversus steroid injection was found.37 One trial compared a lateralversus dorsal tangential SWT application technique in 41 patients.38The trials were performed in Germany,33,35 Germany and Austria,30the UK,31,34,37 Canada,29 the USA32 and Italy.36,38
One article was excluded for not reporting exclusively data of SWT
for lateral elbow tendinopathy in less than 30 participants,39 onearticle reported single-session SWT19 and one was a long-timefollow-up report8 (Fig. 1).
DevicesA variety of devices were used to generate shock waves in the differenttrials with heterogeneous sets of shock wave parameters. Seven trialsgenerated shock waves electromagnetically29,31 –35,38; in one trial, thetype of shock waves was not specified37 and one trial used eight differ-ent shock wave devices at different sites.30 Spacca et al.36 used a radialshock wave device.
Use of local anaesthesiaNine of 10 trials were performed without local anaesthesia and onlyone trial administered local anaesthetics (LAs).30
Intervals of applicationIn all 10 trials, SWT was administered repetitively. In eight trials, theinterval between treatments was weekly.29,31 –33,35– 38 Only in onetrial, the interval was monthly.34 The interval between treatments wasnot provided for one trial.31
Fig. 1 QUOROM statement diagram flow.
Control groupsThe placebo control group generally comprised a physical block to theshock waves (i.e. sound-reflecting polyethylene foil filled with air toreject the shock waves, or no skin contact of the treatment head). Unlike in Buchbinder’s Cochrane analysis, a subtherapeutic dose ofSWT (i.e. 10 or 20 low-energy impulses)35,36 was not regarded as shamtreatment.
One trial compared SWT with 20 mg triamcinolone made up to
1.5 ml with 1% lignocaine injected into the point of maximal tender-ness at the extensor origin of the lateral epicondyle of the humerus.37One trial compared lateral tangential focusing with dorsal tangentialfocusing.38
Repetitive SWT for lateral elbow tendinopathy
Nearly all trials recruited similar study populations. All participantshad lateral elbow pain with most studies also requiring evidence oflocalized tenderness at or near the common extensor tendon insertionat the lateral epicondyle and reproduction of pain with resisted move-ments. Six trials specified that participants had to have had a varyingnumber and/or duration of unsuccessful conservative treatment(s) priorto trial inclusion,30,31 –33,35,36 whereas one trial specifically includedonly participants who had not previously received any treatment.29One trial only included recreational tennis players defined as playingrecreational tennis for at least 1 h per week before symptoms occurred,with chronic symptoms of at least a year, and highly resistant to otherforms of treatment.33
Period of symptoms required for inclusion in the studies differedlargely. Trials required that study participants have a minimum of3 months,34 4 months,37 6 months,30,32,35 10 months36 or 12 months33duration of symptoms prior to inclusion in the trial.
Two trials did not specify a minimum duration of symptoms.31,38
One trial specified that symptoms had to have been present for morethan 3 weeks and less than a year.29
Accordingly, the symptoms of study participants varied between
20 and 30 months. The mean duration of symptoms was much shorterin one trial (5 months).29 The duration of symptoms of study partici-pants was not reported in two trials.31,37
Follow-up assessments were performed at varying time points acrossthe trials, from during treatment to 12 months after the final treatment. Haake et al.30 performed follow-up assessments at 6 and 12 weeks and12 months after the final treatment. Melikyan et al.31 performedassessments at 1, 3 and 12 months after the final treatment. Rompeet al.35 performed assessments immediately after completion of treat-ment and at 3, 6 and 24 weeks after completion of treatment. Speedet al.34 performed assessments prior to the second and third treatments(at 1 and 2 months, respectively) and at 1 month after the final treat-ment. Crowther et al.37 performed assessments at 6 weeks and3 months after either steroid injection or at the end of completion of3 weekly treatments of SWT. Chung and Wiley29 performed
assessments at 1 and 5 weeks after the completion of treatment. Rompe et al.33 performed assessments at 3 and 12 months after com-pletion of treatment, although participants and assessors wereunblinded at 3 months. Pettrone and McCall32 performed assessmentsat 1, 4, 8 and 12 weeks and 6 months and 12 months after the com-pletion of treatment, although participants and assessors could beunblinded at 12 weeks if participants had not achieved at least a 50%reduction in pain, compared with baseline. Spacca et al.36 performedthree assessments: before therapy, after therapy and at 6 months afterthe final SWT.
Outcome assessment was very heterogeneous. Six trials specified aprimary endpoint.29,30,32–34,36 Haake et al.30 specified the primaryendpoint as success rate after 12 weeks, defined as subjective pain scoreof 1 or 2 on the Roles and Maudsley scale [1 ¼ excellent (no pain, fullmovement and activity) and 2 ¼ good (occasional discomfort, full move-ment, full activity and no additional conservative or surgical treatment)]. Another trial35 also used the Roles and Maudsley scale and determinedfailure of treatment at 12 weeks, defined as a score of 4 ¼ poor (painlimiting activities). Speed et al.34 specified the primary endpoint to be a50% improvement in pain from baseline at 1 month after the end of treat-ment. Chung and Wiley29 specified the primary endpoint as treatmentsuccess at 8 weeks (5 weeks after the completion of treatment), defined asfulfilment of all of the following three criteria: (i) at least a 50%reduction in overall elbow pain as measured by overall pain visual analogscale (VAS); (ii) maximum allowable overall elbow pain score of 4.0 cmand (iii) no use of pain medications for lateral elbow pain for 2 weeksbefore the 8-week evaluation. Pettrone and McCall32 and Rompe et al.33specified the primary endpoint as reduction in pain elicited by provocativeThomsen testing recorded on VAS at 12 weeks following completion oftreatment, compared with baseline. Spacca et al.36 defined the primaryendpoint as a reduction of 3 points during resisted wrist extension.
Pain scales included in the trials were heterogeneous. Three studies usedvalidated measures of function—the Disabilities of Arm, Shoulder andHand (DASH)31,36 or the upper extremity functional scale (UEFS).32,33
Three trials30,33,35 used the Roles and Maudsley scale that combines
assessment of pain and satisfaction with treatment into a 4-point categ-orical scale.
Repetitive SWT for lateral elbow tendinopathy
Rompe et al.33 measured overall satisfaction by asking participants
whether they were able to perform activities at the desired level and tocontinue to play recreational tennis.
One study used the thermometer subsection of the EuroQol 5D
(EQ5D) quality-of-life instrument to assess quality of life.29
Pettrone and McCall32 also used a ‘patient-specific activity score’ by
asking participants to identify two activities from the UEFS that theyfound particularly difficult to perform and rate their difficulty from 1(no difficulty) to 10 (cannot perform) and an overall participant evalu-ation of their disease status on a 100 mm VAS.
Melegati et al.38 collected subjective data before the treatment and
after 6 months using the Total Elbow Scoring System.
Two studies measured analgesic use29,31 and one study recorded the
number of participants who proceeded to surgery.31
Overall, the studies were clinically heterogeneous with respect to the
duration of the disorder; type, frequency and total dose of SWT;period of time between SWT; type of management and control group;timing of follow-up and outcomes assessed.
Although all 10 trials were described as randomized, only four trialsdescribed their method of randomization.29,30,33,37
Concealment of treatment allocation was adequate in two trials29,30and adequate to 12 weeks following completion of treatment in twotrials.32,33 Concealment was considered unclear in the remaining sixtrials.31,34 –38
Participants were reported to be blinded in six trials,29,30– 34 and theassessment of outcome was blinded in eight trials.29,30– 36
The trial comparing steroid injection with SWT was not patient-
blinded,37 as were both trials comparing SWT with low-numberSWT.35,39
One trial unblinded all participants and outcome assessors at 12
weeks after the completion of treatment.33 Restrictions of treatmentwere lifted at this time and participants in the placebo group with per-sisting symptoms were offered active treatment. One trial alsounblinded participants at 12 weeks after the completion of treatment if
there had not been at least a 50% improvement in pain elicited by theThomsen test, compared with baseline.32 Participants in the placebogroup were also offered the active treatment at this time and outcomeassessors were unblinded if participants received cross-over treatment. It is not known whether unimproved participants in the active group(who were unblinded at 12 weeks) could receive additional treatment.
Six trials reported that the analysis was performed on the basis ofintention to treat.29,30,32 –34,36 This could not be verified for twotrials.34,36 Three trials performed a completers analysis only.31,35,37
Four trials reported a sample size calculation.29,30,32,33 Haake et al.30had sufficient power to demonstrate a 20% difference in outcome ofthe primary endpoint (success rate at 12 weeks), and Chung andWiley29 calculated that a sample size of 30 participants per groupwould have sufficient power to detect a 2-fold difference in the pro-portion of treatment successes at 8 weeks (5 weeks after the completionof treatment), assuming that 20% of the placebo group would have atreatment success (i.e. 60% success rate in the active group), allowingfor a 20% dropout/loss to follow-up rate. They considered that treat-ment successes in 60% of the SWT group would constitute a clinicallyrelevant and successful result. Rompe et al.33 reported that a samplesize of 35 patients per group would have 80% power in detecting adifference of 2 points in average pain rating to resisted wrist extensionat the 3-month assessment (i.e. assuming pain is 5 + 2 points in theplacebo group and will be 3 + 2 in the active group) with a two-sidedsignificance level of 0.01. Pettrone and McCall32 calculated that asample size of 45 participants per group would provide sufficientpower to demonstrate a 30% difference between the proportion of par-ticipants who improved by at least 50% from baseline to 12 weeksafter the completion of treatment assuming a 50% success in placebo(80% success in active SWT) and number was increased to 114 assum-ing a retention rate of at least 80%.
Per-study methodological quality assessment
Rompe et al.35 have published a randomized-controlled trial investi-gating SWT for lateral elbow pain performed at a single centre in
Repetitive SWT for lateral elbow tendinopathy
Germany. They report the results of 115 chronic recalcitrant partici-pants treated over a 3-year period.
The treatment group received 3Â1000 low-energy impulses without
local anaesthesia at weekly intervals and the control group received3Â10 identical impulses at weekly intervals. Main follow-up was 6months.
Fifteen participants were reported to discontinue treatment during
the first 6 weeks and were not subsequently included in the analysis(dropouts 15/115 ¼ 13%). Follow-up was reported at 3, 6, 24 and 52weeks. The trial was reported to be randomized, but the method ofrandomization was not described and therefore it is unclear whetherallocation concealment was adequate. Both the participants and theoutcome assessors were reported to be blinded to treatment allocation. The analysis was performed for completers of the trial only (n ¼ 100)and the treatment allocation for the 15 participants (13%) whodropped out was not reported.
Crowther et al.37 performed a randomized controlled trial in the UK
including 93 chronic recalcitrant participants.
The treatment group received 3Â2000 low-energy impulses without
local anaesthesia at weekly intervals and the control group received aninjection of 20 mg of triamcinolone made up to 1.5 ml with 1% lido-caine. Main follow-up was 3 months.
Patients in the trial were randomized using closed unmarked envel-
opes. It is unclear whether allocation concealment was adequate. Itappears that the patients were not blinded and it is not stated whetheroutcome assessment was blinded. Three of 51 (5.9%) participants ran-domized to SWT withdrew prior to completion of treatment and 17 of52 (32.7%) participants randomized to steroid injection refused partici-pation after randomization. Patients who had been included in thestudy
Haake et al.30 performed a multicentre randomized placebo-
controlled study in Germany and Austria including 271 participants.
The treatment group received 3Â2000 low-energy impulses at weekly
intervals under local anaesthesia and the control group received3Â2000 sham impulses at weekly intervals under local anaesthesia. Main follow-up was 3 months.
It was reported to be single-blind on the basis that the participants
were blinded to intervention, but the provider of the intervention wasnot blinded. However, blinded outcome assessors were used. Allocation concealment was adequate. Randomization occurred cen-trally by phone, using random permuted blocks of sizes six and fourwith separate randomization lists for each centre. Intention-to-treatanalysis was used, and loss to follow-up was reported for 10 (7.5%)
and 15 (10.9%) participants in the active and placebo groups,respectively.
Speed et al.34 performed a single-centre randomized controlled trial
in the UK including 75 participants. The treatment group received3Â1500 low-energy impulses without local anaesthesia at monthlyintervals and the control group received 3Â1500 sham impulses atmonthly intervals. Main follow-up was 1 month.
The trial was reported to be randomized, but the method of ran-
domization was not described and therefore it is unclear whether allo-cation concealment was adequate. Both participants and outcomeassessors were reported to be blinded to treatment allocation. Four(5.3%) withdrew from the trial (two in the active group after two treat-ments because of worsening symptoms and two in the placebo groupfor reasons which were unclear). Data were reported to be analysed onan intention-to-treat basis, but it is unclear how missing data for thefour participants who withdrew were handled in the analysis.
Melikyan et al.31 performed a randomized-controlled trial in the UK
including 86 chronic recalcitrant participants.
The treatment group received 3Â a variable number of low-energy
impulses without local anaesthesia at weekly intervals and the controlgroup received sham impulses at weekly intervals. Main follow-up was6 months.
The trial was reported to be randomized, but the method of ran-
domization was not described and therefore it is unclear whether allo-cation concealment was adequate. Both participants and outcomeassessors were reported to be blinded to treatment allocation. Elevenparticipants did not complete a full course of treatment and anadditional participant did not attend for follow-up (12/86, 14%). These 12 participants were not included in the efficacy assessment anda completers-only analysis was performed.
Melegati et al.38 performed a randomized-controlled trial including
41 participants. The treatment group received 3Â1800 low-energyimpulses without local anaesthesia at weekly intervals using tangentialfocusing and the control group received identical impulses using dorsalfocusing. Main follow-up was 6 months.
The randomization procedure was not described. It is unclear
whether allocation concealment was adequate. It appears that thepatients were not blinded and it is not stated whether outcome assess-ment was blinded. No patient was lost to follow-up. Allocation con-cealment was considered unclear.
Chung and Wiley29 performed a randomized-controlled trial in
Canada including 60 subchronic previously untreated participants.
The treatment group received 3Â2000 low-energy impulses of a
varying intensity without local anaesthesia at weekly intervals and the
Repetitive SWT for lateral elbow tendinopathy
control group received 2000 sham impulses. Main follow-up was 3months.
Trial participants were randomized according to block randomiz-
ation. All participants and outcome assessors were blinded to treatmentallocation.
Participants were not aware that there was a placebo treatment, butwere informed the study was comparing two different therapy proto-cols. The authors stated that this deception was performed to preservesubject blinding because of widespread accessibility of information onSWT protocols, particularly information regarding discomfort duringtherapy. Four participants (6.7%) were lost to follow-up. Analysis wasaccording to intention to treat with last observation used for missingoutcome data.
Rompe et al.33 performed a randomized-controlled trial in Germany
including 78 chronic recalcitrant participants, all of whom were rec-reational tennis players with symptoms for at least 12 months.
The treatment group received 3Â2000 low-energy impulses without
local anaesthesia at weekly intervals and the control group receivedsham impulses at weekly intervals. Main follow-up was 3 months.
Trial participants were randomized according to a computer-
generated random numbers list and only the person performing theintervention knew the treatment allocation. Both participants andoutcome assessors were blinded up until the 3-month assessment, butwere unblinded at this time point. Eight participants (10.3%) did notprovide 3-month data. A further six participants were lost to follow-upfor the 12-month assessment. Analysis was according to intention totreat with last observation used for missing outcome data. Allocationconcealment was considered adequate.
Pettrone and McCall32 performed a randomized-controlled trial in
three centres in the US including 114 chronic recalcitrant participantsonly.
The treatment group received 3Â2000 low-energy impulses without
local anaesthesia at weekly intervals and the control group receivedsham impulses at weekly intervals. Main follow-up was 3 months.
Treatment allocation concealment was adequate as at randomization
and each participant was given a unique study number and a sealedenvelope with their study number on it. All participants and outcomeassessors were blinded to treatment allocation up to 12 weeks follow-ing the completion of treatment. Six participants (5.3%) withdrewbefore the 12-week assessment. Analysis was according to intention totreat with last observation used for missing outcome data.
Spacca et al.36 performed a randomized controlled trial in Italy
including 62 chronic recalcitrant participants.
The treatment group received 3Â2000 low-energy impulses without
local anaesthesia at weekly intervals and the control group received3Â20 low-energy impulses. Main follow-up was 6 months.
The procedure of randomization was not described. It is unclear
whether allocation concealment was adequate. Patients were notblinded and it is not stated whether outcome assessment was blinded. There was no loss to follow-up until the primary endpoint at 6 months.
To allow easier understanding of the key elements of the individual
studies, a summarizing assessment was performed according toChalmers et al.,40 with two evaluation forms which include 29 indivi-dually scored items, allowing a maximum score of 100. Following therecommendation from Stasinopoulos and Johnson,3 a score of 70% isconsidered to be the minimum required for a high-quality design forcontrolled therapeutic trials. If the score is below 40% (0– 39), thedesign of the study is of low quality, and, if it is 40 –69%, it issatisfactory.
Table 2 summarizes the evaluation for the 10 included trials. The
average Chalmers’ score was 62.5%, with a minimum of 47% for theweakest study design38 and a maximum of 75% for the strongestones.30,32 All studies had at least a satisfactory quality design.
Two placebo-controlled trials reported significant differences in
favour of SWT for all or most measured endpoints.32,33 Involving 196participants, both studies observed the following principles: (i) chronicrecalcitrant cases; (ii) 2000 low-energy impulses; (iii) 3Â in weeklyintervals; (iv) clinical focusing, no local anaesthesia and (v) mainfollow-up of 3 months. In the study by Rompe et al.,33 at 3 months65% of patients achieved at least a 50% reduction in pain, comparedwith 28% of patients in the sham group. Using exactly the treatmentregimen of Pettrone and McCall,32 they found a statistically significantdifference in pain reduction at 12 weeks. Sixty-one per cent of active-treated patients showed at least 50% improvement in pain, comparedwith 29% in the placebo group. This was found to persist for 1 year.
Success rates of SWT groups, undergoing a comparable treatment
regimen in three treatment-controlled trials, were 48,35 6037 and84%.36
Three trials did not find any benefit of SWT over placebo.29,30,34 All
deviated from the concept of application outlined earlier.
Haake et al.30 reported a multicentre, randomized, placebo-
controlled study on chronic recalcitrant participants. The treatmentgroup received 3Â2000 low-energy impulses at weekly intervals underlocal anaesthesia and the control group received 3Â2000 shamimpulses under local anaesthesia at weekly intervals. Main follow-upwas 3 months. Overall, therapeutic success rate 12 weeks after inter-vention ( primary endpoint) was 32% in the SWT and 33% in the
Bold: most important differences in the study design. SWT, shock wave treatment.
Repetitive SWT for lateral elbow tendinopathy
placebo group. The authors concluded that this treatment did not haveany added therapeutic benefit beyond placebo.
Speed et al.34 performed a single-centre, randomized-controlled trial
in the UK including 75 participants. The treatment group received3Â1500 low-energy impulses without local anaesthesia at monthlyintervals and the control group received 3Â1500 sham impulses atmonthly intervals. Main follow-up was 1 month.
Chung and Wiley29 did not deviate from the treatment regimen out-
lined earlier. However, they changed the selection of patients fromchronic recalcitrant to acute, previously untreated cases. Mainfollow-up was 2 months, and success rates in the sham and activetherapy groups were 31 and 39%, respectively.
Low-energy SWT for tendinopathies is not widely known among themedical community. The rationale for its clinical use being stimulationof soft tissue healing and inhibition of pain receptors, and hence, it hasbeen thoroughly investigated experimentally during the past decade. Ohtori et al.41 demonstrated that after low-energy shock wave appli-cation, the number of sensory fibres in the epidermis decreased signifi-cantly as indicated by the loss of immunoreactivity for calcitoningene-related peptide. Re-innervation of the epidermis started 2 weeksafter treatment. When repeating shock wave application after 14 daysin another experiment, Takahashi et al.42 described the delay ofre-innervation for as long as 42 days, significantly longer than aftersingle shock wave application. Wang et al.43 found that low-energySWT positively influenced neovascularization at the tendon –bone junc-tion in rabbits, producing a significantly higher number of neo-vesselsand angiogenesis-related markers, including endothelial nitric oxidesynthase, vessel endothelial growth factor and proliferating cell nuclearantigen. Chen et al.44 reported that low-energy SWT promoted healingof Achilles tendinopathy. Proliferation of tenocytes adjunct to hypertro-phied cell aggregate and newly formed tendon tissue coincided withintensive TGF-beta1 and IGF-I expression. The effect of shock wavesappeared to be time-dependent.
Although experimentally positive effects of SWT on tendon healing
and pain modulation have become undebatable, conflicting resultswere found in this qualitative review of randomized controlled trials onthe effectiveness of SWT for lateral elbow tendinopathy.
Ten controlled trials including 948 participants, reporting conflicting
results, were included in this systematic review. Overall, the studieswere clinically heterogeneous with respect to the duration of the
disorder; type, frequency and total dose of SWT; period of timebetween SWT; type of management and control group; timing offollow-up and outcomes assessed.
Confronted with clinical and methodological heterogeneity, the stat-
isticians involved thought it would be better to present this systematicreview using a more qualitative approach instead of combining results. A systematic descriptive analysis was given preference.
Two placebo-controlled trials32,33 reported highly significant differ-
ences in favour of SWT and three did not.29,30,34 Three moretreatment-controlled trials reported effectiveness of SWT35,36,38 andtwo did not.31,37
The discrepancy in the results between the positive and negative trials
in our review may be explainable on the basis of differing trial quality. The largest negative trial (271 participants) was of high quality with avalid randomization method, adequate concealment of treatment allo-cation,
intention-to-treat analysis. It reported both a prespecified primary end-point and sample size calculation.30 The second negative trial (75 par-ticipants) did not report its method of randomization, but did blindboth participants and outcome assessors, reported a prespecifiedprimary endpoint and performed an intention-to-treat analysis,although it is not clear whether it was adequately powered to detect aclinically important difference between groups as no sample size calcu-lation was reported.34 Owing to inadequate reporting of results, oneplacebo-controlled trial published in 2003 did not provide conclusivedata, but supported the ineffectiveness of SWT.31 The two positivetrials32,33 allowed either all patients to be unblinded at 12 weeks33 orunblinding at 12 weeks for those without an adequate response.32 Inboth trials, placebo patients were also offered cross-over into the activegroup at 12 weeks and unblinded patients were allowed additionaltherapy. Restriction on other treatments was also lifted at this time,although additional treatments received by unimproved participants inthe active group were not reported. Owing to a diminished number ofblinded participants, and the possibility of confounding of any treat-ment effects, it was impossible to interpret the long-term results ofthese trials.
This review also included one trial comparing steroid injection with
SWT, which demonstrated a benefit of steroid injection over SWT at3 months with respect to 50% reduction in pain.37 However, followingrandomization, a considerable number of patients allocated to injectiontherapy withdrew from the study, making interpretation of the resultsdifficult.
We found a lack of uniformity in both the timing of follow-up and
the outcomes that were measured. All studies measured pain, with
Repetitive SWT for lateral elbow tendinopathy
some including varying aspects of pain. Three trials used the Roles andMaudsley scale which incorporates both pain and an assessment ofwhether pain limits activities into a 4-point categorical scale,30,33,35although Rompe et al.33 analysed the results as a continuous ratherthan categorical data. Three trials included an upper-arm-specific dis-ability measure (the DASH)31,36 or the UEFS,32,33 and no trial includeda generic quality-of-life instrument. An international consensus for theuse of a standard set of outcome measures in clinical trials for lateralelbow pain that are valid, reliable and sensitive to change wouldimprove our ability to interpret and compare the results of differentstudies.19,20,45,46 These might include overall pain with or without pro-vocation, a measure of upper extremity function (such as the UEFS),ability to carry out usual activities, work and/or sport and possiblyalso a measure of quality of life.
There continues to be considerable debate relating to the use of SWT
in soft tissue musculoskeletal complaints: the optimal shock wave treat-ment regimes; dosing intervals and whether focusing of SWT to thesite of pathology can be improved by fluoroscopy or ultrasound. Someexperts argue that the shock waves should be focused on the site ofmaximal tenderness as determined by the patient and imaging mayresult in errors in localization of the pathology; whereas the contraryview is that imaging, together with clinical input from the patient, mayimprove the accuracy and therefore the efficacy of SWT.26
One of the most interesting questions is whether application of an
LA has a negative effect on the outcome of tendinopathies afterSWT.47 These interventions are sometimes used as the treatment,which is uncomfortable and sometimes painful. Recently, two interest-ing papers were published, comparing the use of SWT with andwithout local anaesthesia in patients with chronic plantar fasciopathy.
Labek et al.48 reported that they had enrolled 60 patients with a
chronic plantar fasciitis in a triple-arm randomized trial. Patients wererandomly assigned to receive repetitive low-energy SWT without localanaesthesia (group I) or repetitive SWT (energy flux density doubled)with local anaesthesia (group II) or repetitive low-energy SWT withlocal anaesthesia (group III). At 6 weeks, there was significant improve-ment in pain during first steps in the morning in all groups, by 4.2points in group I, by 2.6 points in group II and by 2.4 points in groupIII. A reduction in pain of at least 50% was achieved in 60% ofpatients in group I, in 36% of patients in group II and in 29% ofpatients in group III. In conclusion, at 6 weeks, success rates after low-energy SWT with local anaesthesia were significantly lower than thatafter identical low-energy SWT without local anaesthesia.
A current randomized-controlled study from Germany49 confirmed
their observation. The average pain score for patients who received
SWT without local anaesthesia (group I) was 6.9 points at baseline and2.2 points at 3 months. The average pain score for patients whoreceived SWT with local anaesthesia (group II) was 6.7 points at base-line and 4.1 points at 3 months. At 3 months in group I, 67% ofpatients achieved at least a 50% reduction in pain, compared with29% of patients in group II.
In the only human experiment in this field so far, Klonschinski
et al.50 investigated whether the biological effects of SWT differbetween application with and without an LA in humans. SWT wasapplied to the skin after local pretreatment either with lidocain creamLA or without LA to the corresponding location of the contralaterallimb. Increasing energy flux density led to a significant increase ofpain. LA significantly attenuated this pain and significantly inhibitedC-fibre activity, with a significant reduction in local vasodilation. Reduction in vasodilation correlated positively with the amount ofenergy flux density applied. SWT without LA resulted in a dose-dependent lower pressure pain threshold, i.e. sensitization, than didSWT with LA. Together, SWT in a dose-dependent fashion activatedand sensitized primary afferent nociceptive C-fibres in human skin. LAsubstantially altered the biological responses after SWT.
Obviously, accurate targeting of the pathology at the spot of
maximal point tenderness, as described to the examiner by the patient,is crucial for optimal application of low-energy shock waves. This isimpossible after application of local anaesthesia.
Studies that directly compare one machine with another or compare
dosing intervals and so on may be able to determine whether there areany differences in outcome. In part, physical differences between thedevices used for the individual trials may explain for the heterogeneityof outcomes. One trial has compared two different ultrasound localiz-ing techniques and reported no difference in outcome.38
A second, related point of difference is whether imaging such as
ultrasound or magnetic resonance imaging (MRI) has a role in estab-lishing the presence of pathology at the site of tendon insertions suchas the common extensor origin in patients with lateral elbow pain. Forexample, the recent trial by Rompe et al.33 required a positive MRI(increased signal intensity of extensors) for study inclusion. This mayincrease the homogeneity of the study population, increase the likeli-hood of being able to demonstrate benefit of a new therapy if oneexists and enable valid comparisons to be made between studies.26
As already pointed out by Buchbinder et al.,26 all trials included in
this review reported improvement in outcome in both the treated andnon-treated populations. These observed treatment effects might beexplained on the basis of placebo effects related to participating in atrial or the self-limiting natural history of the condition. Proponents of
Repetitive SWT for lateral elbow tendinopathy
SWT, highlighting the favourable natural history of this condition withits high rate of spontaneous improvement,51 have asserted that thistreatment should be reserved for patients with chronic recalcitrantcases that have failed to respond to a multitude of other conservativetreatments such as NSAIDs, corticosteroid injections, orthotics andphysiotherapeutic modalities.32,33,35,36 The trial by Chung and Wiley29who failed to find any evidence of benefit of SWT for patients withsymptoms of lateral elbow pain who had not previously been treatedsupports this opinion.
The assumption that a meta-analysis routinely represents the final andaccurate viewpoint in an area of research is not warranted. The authorsneed to determine how broadly their conclusions can be applied and towhat patient groups. The addition of study protocols that are signifi-cantly different from one another can make a meta-analysis less reliable.
Because of the multiple variables inherent in the use of SWT in the
management of lateral elbow tendinopathy (LET), pooled comparisonsof published results appear problematic. Currently, there is no consen-sus on the use of repetitive low-energy SWT, which does not requirelocal anaesthesia, and on the use of high-energy SWT, which requireslocal or regional anaesthesia. There is no consensus for differentiatingbetween low-energy and high-energy shock waves as multiple physicalvariables are involved.
What are the implications for clinical practice?On the basis of well-designed studies showing favourable or
unfavourable results, it seems that the literature supports a therapeuticbenefit of SWT for managing chronic lateral elbow tendinopathy underrestricted conditions only. In this context, this qualitative review ident-ified common variables going along with satisfying results of SWT inthe range of 60%:
repetitive application of 2000 low-energy SWT at weekly intervals for3 – 6 weeks;
follow-up at least 3 months after last application.
Our research has further identified components that may possibly havean adverse effect on the clinical outcome: enrolment of acute, pre-viously untreated patients; repetitive application of low-energy SWT at
monthly intervals; use of local anaesthesia and follow-up less than3 months.
Accordingly, SWT is recommended only after routine therapy
options have failed and when the patients are confronted with the indi-cation of a surgical intervention.
Clearly, we are in a situation where there is still uncertainty (not
enough trials of high quality and contradictory evidence from a groupof trials). Clearly, there is a need for further research in order to gainsufficient evidence to assess the effects of SWT of lateral elbow tendi-nopathy. This further research needs to be targeted to specific issuesthat have arisen out of this review (homogenous intervention; identicaloutcome
follow-up evaluation). In the end, a large-scale high-quality controlledtrial comparing repetitive low-energy SWT applied without local anaes-thesia with a standard surgical approach in patients with a previouslyrecalcitrant lateral elbow tendinopathy is the ultimate goal.
Ashe MC, McCauley T, Khan KM (2004) Tendinopathies of the upper extremity. A paradigmshift. J Hand Ther, 17, 329– 334.
Smidt N, Lewis M, van der Windt DA et al. (2006) Lateral epicondylitis in general practice:course and prognostic indicators for outcome. J Rheumatol, 33, 2053–2059.
Stasinopoulos D, Johnson MI (2005) Effectiveness of extracorporeal shock wave therapy fortennis elbow (lateral epicondylitis). Br J Sports Med, 39, 132–136.
Teitz CC, Garrett WE, Miniaci A et al. (1997) Tendon problems in athletic individuals. JBJS,79-A, 138–152.
Theis C, Herber S, Meurer A et al. (2004) Evidence-based evaluation of present guidelinesfor the treatment of tennis elbow—a review. Zentralbl Chir, 129, 252– 260.
Walker-Bone K, Palmer KT, Reading I et al. (2004) Prevalence and impact of musculoskeletaldisorders of the upper limb in the general population. Arthritis Rheum, 51, 642–651.
Whaley AL, Baker CL (2004) Lateral epicondylitis. Clin Sports Med, 23, 677–691.
Erak S, Day R, Wang A (2004) The role of supinator in the pathogenesis of chronic lateralelbow pain: a biomechanical study. J Hand Surg [Br], 29, 461– 464.
Kraushaar BS, Nirschl RP (1999) Tendinosis of the elbow (tennis elbow). Clinical featuresand findings of histological, immunohistochemical, and electron microscopy studies. JBJS,81-A, 259–278.
Nirschl RP, Rodin DM, Ochiai DH et al. (2003) Iontophoretic administration of dexametha-sone sodium phosphate for acute epicondylitis. Am J Sports Med, 31, 189–194.
Scott A, Khan KM, Roberts CR et al. (2004) What do we mean by the term ‘inflammation’?A contemporary basic science update for sports medicine. Br J Sports Med, 38, 372– 380.
Sems A, Dimeff R, Ianotti JP (2006) Extracorporeal shock wave therapy in the treatment ofchronic tendinopathies. J Am Acad Orthop Surg, 14, 195–204.
Boyer MI, Hastings H (1999) Lateral tennis elbow: is there any science out there? J ShoulderElbow Surg, 8, 481–491.
Buchbinder R, Green S, Bell S et al. (2002) Surgery for lateral elbow pain (Cochrane review). Cochrane Database Syst Rev, CD003525.
Cole BJ, Schumacher HR (2005) Injectable corticosteroids in modern practice. J Am AcadOrthop Surg, 13, 37–46.
Repetitive SWT for lateral elbow tendinopathy
Fink M, Wolkenstein E, Karst M et al. (2002) Acupuncture in chronic epicondylitis: a ran-domized controlled trial. Rheumatology (Oxford), 41, 205– 209.
Green S, Buchbinder R, Barnsley L et al. (2002) Acupuncture for lateral elbow pain(Cochrane review). Cochrane Database Syst Rev, CD003527.
Green S, Buchbinder R, Barnsley L et al. (2002) Non-steroidal anti-inflammatory drugs(NSAIDs) for treating lateral elbow pain in adults. Cochrane Database Syst Rev, CD003686.
Macdermid J (2005) Update: the patient-rated forearm evaluation questionnaire is now thepatient-rated tennis elbow evaluation. J Hand Ther, 18, 407 –410.
Newcomer KL, Martinez-Silvestrini JA, Schaefer MP et al. (2005) Sensitivity of thepatient-rated forearm evaluation questionnaire in lateral epicondylitis. J Hand Ther, 18,400–406.
Sharma P, Maffulli N (2005) Tendon injury and tendinopathy: healing and repair. JBJS,87-A, 187– 202.
Smidt N, Assendelft WJ, van der Windt DA et al. (2002) Corticosteroid injections for lateralepicondylitis: a systematic review. Pain, 96, 23 –40.
Smidt N, van der Windt DA, Assendelft WJ et al. (2002) Corticosteroid injections, phy-siotherapy, or a wait-and-see policy for lateral epicondylitis: a randomised controlled trial. Lancet, 359, 657– 662.
Struijs PA, Smidt N, Arola H et al. (2002) Orthotic devices for the treatment of tennis elbow(Cochrane review). Cochrane Database Syst Rev, CD001821.
Van de Streek MD, van der Schans CP, De Greef MH et al. (2004) The effect of a forearm/hand splint compared with an elbow band as a treatment for lateral epicondylitis. ProsthetOrthot Int, 28, 183– 189.
Buchbinder R, Green S, White M et al. (2005) Shock wave therapy for lateral elbow pain(review). Cochrane Database Syst Rev.
Van Tulder MW, Furlan A, Bombardier C et al. (2003) Updated method guidelines for sys-tematic reviews in the cochrane collaboration back review group. Spine, 28, 1290–1299.
Moher D, Cook DJ, Eastwood S et al. (1999) Improving the quality of reports ofmeta-analyses of randomised controlled trials: the QUOROM statement. Lancet, 354,1896–1900.
Chung B, Wiley JP (2004) Effectiveness of extracorporeal shock wave therapy in the treat-ment of previously untreated lateral epicondylitis: a randomized controlled trial. Am J SportsMed, 32, 1660–1667.
Haake M, Koenig IR, Decker T et al. (2002) Extracorporeal shock wave therapy in the treat-ment of lateral epicondylitis. JBJS, 84-A, 1982–1991.
Melikyan EY, Shahin E, Miles K et al. (2003) Extracorporeal shock wave therapy for tenniselbow. A randomized double blind study. JBJS, 85-B, 852–855.
Pettrone F, McCall B (2005) Extracorporeal shock wave therapy without local anaesthesiafor chronic lateral epicondylitis. JBJS, 87-A, 1297– 1304.
Rompe JD, Decking J, Schoellner C et al. (2004) Repetitive low energy shock wave treatmentfor chronic lateral epicondylitis in tennis players. Am J Sports Med, 32, 734– 743.
Speed C, Nichols D, Richards C et al. (2002) Extracorporeal shock wave therapy for lateralepicondylitis: a double blind randomized controlled trial. J Orthop Res, 20, 895–898.
Rompe JD, Hopf C, Kullmer K et al. (1996) Analgesic effects of extracorporeal shock wavetherapy on chronic tennis elbow. J Bone Joint Surg, 78-B, 233– 237.
Spacca G, Necozione S, Cacchio A (2005) Radial shock wave therapy for lateral epicondyli-tis: a prospective randomised controlled single-blind study. Eur Med Phys, 41, 17 –25.
Crowther A, Bannister GC, Huma H et al. (2002) A prospective study to compare extracor-poreal shock wave therapy and injection of steroid for the treatment of tennis elbow. JBJS,84-B, 678–679.
Melegati G, Tornese D, Bandi M et al. (2004) Comparison of two ultrasonographic localiz-ation techniques for the treatment of lateral epicondylitis with extracorporeal shock wavetherapy: a randomized study. Clin Rehabil, 18, 366– 370.
Mehra A, Zaman T, Jenkin AI (2003) The use of a mobile lithotripter in the treatment oftennis elbow and plantar fasciitis. Surg J R Coll Surg Edinb Irel, 1, 290–292.
Chalmers TC, Smith H, Blackburn B et al. (1981) A method for assessing the quality of arandomized control trial. Control Clin Trials, 2, 31 –49.
Ohtori S, Inoue G, Mannoji C et al. (2001) Shock wave application to rat skin inducesdegeneration and reinnervation of sensory nerve fibres. Neurosci Lett, 315, 57 –60.
Takahashi N, Ohtori S, Saisu T et al. (2006) Second application of low-energy shock waveshas a cumulative effect on free nerve endings. Clin Orthop, 443, 315– 319.
Wang CJ, Wang FS, Yang KD et al. (2003) Shock wave therapy induces neovascularization atthe tendon– bone junction. A study in rabbits. J Orthop Res, 21, 984– 989.
Chen YJ, Wang CJ, Yang KD et al. (2004) Extracorporeal shock waves promote healing ofcollagenase-induced Achilles tendinitis and increase TGF-beta1 and IGF-I expression. J Orthop Res, 22, 854–861.
Overend TJ, Wuori-Fearn JL, Kramer JF et al. (1999) Reliability of a patient-rated forearmevaluation questionnaire for patients with lateral epicondylitis. J Hand Ther, 12, 31– 37.
Rompe JD, Overend TJ, MacDermid JC (2007) Validation of the patient-rated tennis elbowevaluation questionnaire. J Hand Ther, 20, 3 –10.
Rompe JD, Furia J, Weil L et al. (2007) Shock wave therapy for chronic plantar fasciopathy. Br Med Bull, 81– 82, 183– 208.
Labek G, Auersperg V, Ziernhold M et al. (2005) Influence of local anesthesia and energylevel on the clinical outcome of extracorporeal shock wave-treatment of chronic plantarfasciitis. Z Orthop Ihre Grenzgeb, 143, 240–246.
Rompe J, Meurer A, Nafe B et al. (2005) Repetitive low-energy shock wave applicationwithout local anesthesia is more efficient than repetitive low-energy shock wave applicationwith local anesthesia in the treatment of chronic plantar fasciitis. J Orthop Res, 23,931–941.
Klonschinski T, Schleret T, Birklein F et al. (2005) Reduced efficiency of low-energy extracor-poreal shock wave (SWT) under use of local anesthesia—explanation of efficiency. Presentation at the 7th EFORT Congress, 4 – 7 June, Lisbon, Portugal.
Canoso JJ (2006) The healing power of time: the case of lateral epicondylitis. J Rheumatol,33, 1928–1930.
Levitt RL (2004) Shockwave therapy for chronic lateral epicondylitis—an FDA study. PaperPresented at AOSSM Specialty Day, AAOS Annual Meeting, 13 March, San Francisco, CA,US Food and Drug Administration. Healthtronics Ossatron, Summary of safety and effective-ness, available at http://www.fda.gov/cdrh/pdf/ p990086s003.html (accessed 17 December2006).
Chung B, Wiley JP (2005) Long-term effectiveness of extracorporeal shockwave therapy inthe treatment of previously untreated lateral epicondylitis. Clin J Sport Med, 15, 305– 312.
Dynamic Chiropractic – June 16, 2003, Vol. 21, Issue 13 The Drugging of Our Children, Part 1 (see part 2 below) Since the 60s, parents have told their children, "Just say ’no’ to drugs." TV commercials, parentingmagazines and "wellness " visits to pediatricians send a completely different message. In the past two decades, our society has accepted (and even embraced)
SHELL GADUS NAMING SYSTEM BEST PRACTICE The Shell Gadus grease names are designed to help you Shell recommends the following best practice approach:make the right choice. They include a let er that indicates 1. Check the thickener compatibility guide in this leaflet to the thickener type. Before changing greases, check the ensure you take a proper course of action. compatibility o
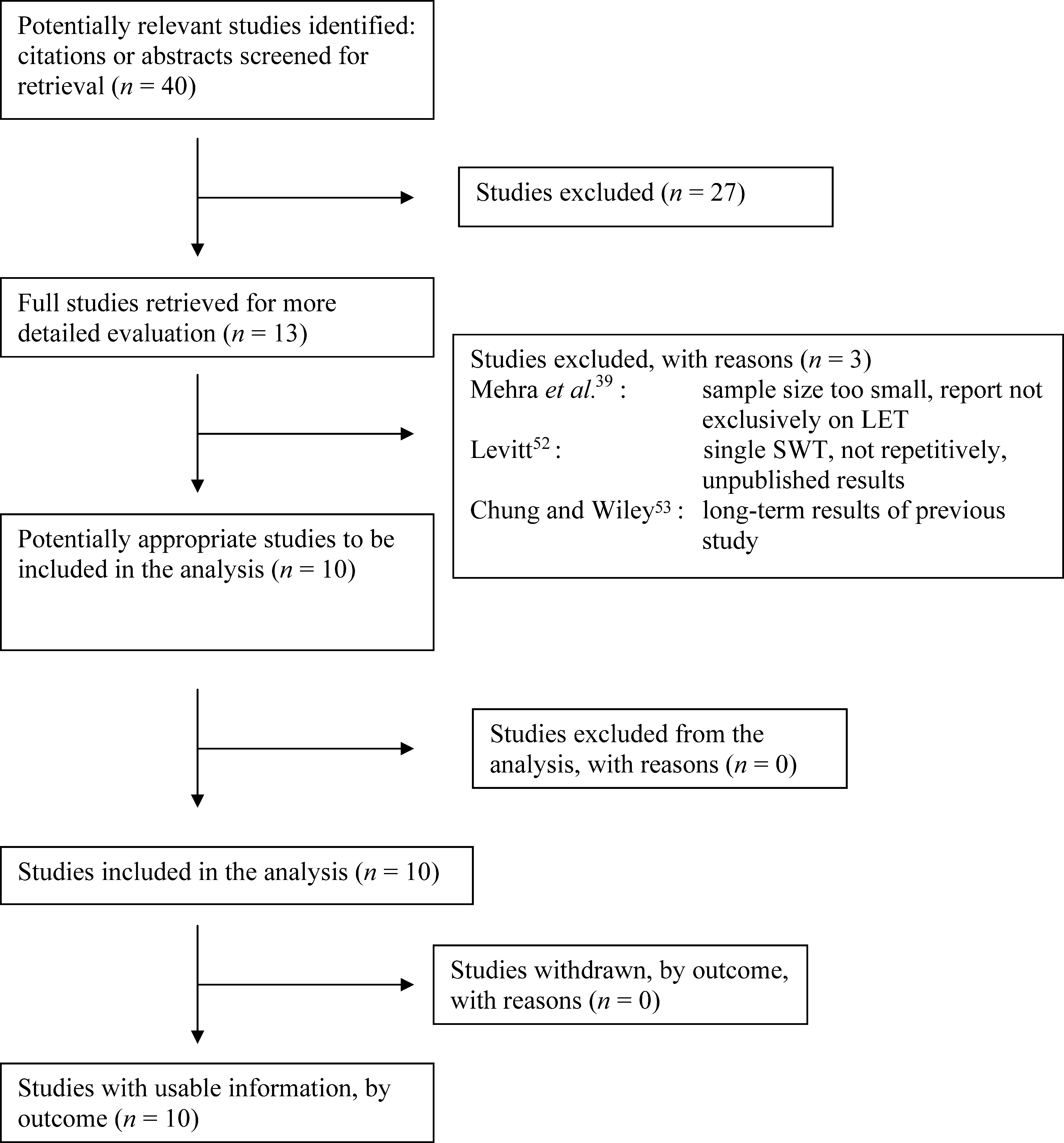 Fig. 1 QUOROM statement diagram flow.
Fig. 1 QUOROM statement diagram flow.