Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Untitled
Preventive Effects of Rosiglitazone on Restenosis after Coronary Stenting in Patients with Type 2 Diabetes Donghoon Choi, MD, PhD Cardiology Division Yonsei University College of Medicine, Background
1. Cardiovascular disease is one of the important leading
cause of deaths in Type 2 diabetic patients.
2. As a result of dramatic increase in implantation
numbers, in-stent restenosis has been significant clinical and socio-economic problems.
3. The in-stent restenosis rate after coronary stenting has
reached up to 45-50 % in type 2 DM patients comparing to 15-25% in non-diabetic patients.
4. The most effective treatment modality for in-stent
Pathogenesis of Restenosis Growth factors & cytokines Receptor activation Smooth muscle cell Cell proliferation Extracellular matrix Migration Synthesis & secretion Approaches for Restenosis Prevention Inflammation Migration Proliferation Reduce injury 1. Enhance biocompatibility 2. Anti-inflammatory Antimigratory Antiproliferative Promote healing & reendotheliali- Atherogenic Effects of PPARγ Ligands in the Vasculature Monocytes Endothelial Cells
↓ Atherosclerosis Male OLETF rat, Balloon injury at 16 weeks and pioglitazone for 3weeks Intima area Intima/media ratio Pioglitazone Pioglitazone
TZDs: effects on carotid arterial intimal and medial co
Troglitazone 400 mg/day IMT (mm) ∆
Japanese subjects with type 2 diabetes*P < 0.001 vs. control
Minamikawa J, et al. J Clin Endocrinol Metab 1998; 83:1818–1820. Study Purpose
• To investigate the preventive effect of PPAR-
γ agonist, rosiglitazone on restenosis after coronary stenting in type II DM patients.
=> 6 month follow-up angiographic binary
Subjects (I)
- Type II DM patients undergoing coronary
stenting at YUMC (Nov. 2001 ~ Dec. 2002)
- LVEF < 40% or evidence of CHF- GOT/GPT > 2 x upper limit of normal range- Cr > 2.0 mg/DL - Previous CABG- Primary PTCA
Subjects (II) Study design and Method
• Anthropometry, Serologic lab : initial and 6 month
• Rosiglotazone : at least 8mg before angiography,
• Control Blood Sugar : continue individual
conventional therapy (sulfonylurea, biguanide,
Baseline Characteristics Rosiglitazone No. (male/female) 45 (34/11) 38 (24/14) Age (years) 59.9±9.3 60.9±9.3 DM duration (years) 7.2±3.8 7.5±4.9 BMI (kg/cm2) 24.8±3.35 24.9±2.96 Fasting glucose (mg/dL) 150.3±28.4 160.3±34.4 HbA1c (%) 7.72±1.13 7.79±1.30 Fasting insulin (µU/mL) 4.97±2.51 5.60±2.70 Total cholesterol (mg/dL) 191.1±48.9 190.5±37.6 HDL-cholesterol (mg/dL) 41.1±10.9 38.9±11.0 Triglyceride (mg/dL) 159.5±55.1 167.7±60.8 Free fatty acid (µmol/L) 580.3±101.7 669.2±127.4 hsCRP (mg/L) 2.01±1.33 2.92±1.98 Medications Rosiglitazone Treatments: No. (%) HMG-CoA reductase 37 (88.1) 31 (81.6) inhibitor ACE inhibitors 30 (71.4) 28 (73.7) Antiplatelet agents 38 (90.5) 34 (89.5) Sulfonylureas 26 (61.9) 25 (65.8) Biguanides 22 (52.3) 21 (55.3)
α-glucosidase inhibitor 15 (35.7) 10 (26.3) Baseline Angiographic Characteristics Rosiglitazone Stented coronary vessels Left main Reference diameter (mm) 3.15±0.49 3.16±0.49 Minimum lumen diameter 0.65±0.41 0.83±0.57 Diameter stenosis (%) 79.4±12.8 74.4±15.8 Lesion length (mm) 16.48±5.16 19.02±6.09 <0.05 Post-stenting Angiographic Data Rosiglitazone Stent diameter (mm) 3.24±0.42 3.29±0.41 Stent length (mm) 18.40±4.75 20.28±5.73 Post-stenting 3.10±0.43 3.13±0.48 Diameter stenosis (%) 2.49±4.26 2.25±4.44 Acute gain (mm) 2.45±0.57 2.30±0.53 Follow-up Biochemical Characteristics Rosiglitazone Baseline FU Baseline FU Fasting glucose (mmol/l) 8.34±1.58 6.87±1.52 8.90±1.91 7.35±1.89 HbA1c (%) 7.72±1.13 7.23±0.93 7.79±1.30 7.17±0.98 Fasting insulin (pmol/l) 35.7±18.0 34.2±18.9 40.2±19.4 34.5±19.7 HDL-cholesterol (mmol/l) 1.06±0.28 1.14±0.27 1.01±0.28 1.12±0.21 Triglyceride (mmol/l) 1.80±0.62 1.43±0.69 1.89±0.69 1.34±0.44 Free fatty acid (µmol/L) 580.3±101.7 548±95.6 669.2±127.4 492.0±101.4 hsCRP (mg/L) 2.01±1.33 1.79±1.22 2.92±1.98 0.62±0.44 Follow-Up Angiographic Data Rosiglitazone 1.91±1.05 2.49±0.88 Diameter Stenosis (%) 40.60±31.90 23.00±23.40 Lumen loss (mm) 1.20±0.97 0.65±0.73 Loss index 0.49±0.42 0.29±0.31 Restenosis rate (%) Clinical Follow-Up Data Target lesion revascularization MACE The Effects of Rosiglitazone on VSMC migration at 48 weeks (mm) Change in m Baseline 0.815 Progression rate (mm/48 weeks) = 0.031 – 0.012*
IMT = intima-media thicknessPatients with clinically stable coronary artery disease without diabetes
RSG dose 4 mg/day for initial 8 weeks; 8 mg/day for remaining 40 weeks*P = 0.03 vs. PBO
Sidhu JS, et al. Arterioscler Thromb Vasc Biol 2004; 24:930–934. Conclusion
• In this study, rosiglitazone has dramatically
reduced restenosis rate of CAOD pateintswith coronary stenting in Type 2 diabetes.
• In type 2 diabetes patients with CAOD, using
PPAR-γ agonist, not only for glucose lowering and insulin sensitizing effect, but also for anti-inflammatory effect, has to be strongly considered.
MATERIAL SAFETY DATA SHEET TRIETHYLENE GLYCOL (ALL GRADES) _______________________________________________________________________________________________ 1. CHEMICAL PRODUCT AND COMPANY IDENTIFICATION _______________________________________________________________________________________________ Brenntag Canada Inc. WHMIS Number: 00060866 43 Jutland Road. Index: GCD1354/06A Toro
SatelLite50-TH/E Combined humidity and temperature logger Description Operation SatelLite50-TH/E is a compact two-channel datalogger The built-in electronics are powerd from a single for connection of an external combined termperature standard 1.5V battery. This reduces the battery cost to and humidity sensor. SatelLite50-TH/E is characterised one-tenth of the special 3.6V Lithiu
 Preventive Effects of
Preventive Effects of  Background
Background
 Pathogenesis of Restenosis
Pathogenesis of Restenosis Approaches for Restenosis
Approaches for Restenosis  Atherogenic Effects of PPARγ Ligands
Atherogenic Effects of PPARγ Ligands
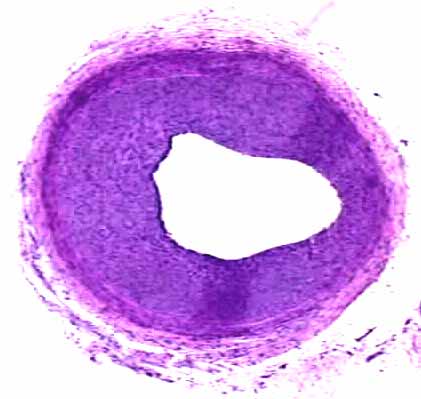
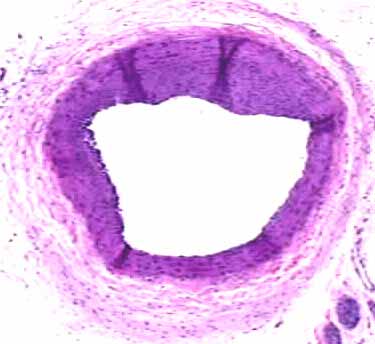 Male OLETF rat, Balloon injury at 16 weeks
Male OLETF rat, Balloon injury at 16 weeks  TZDs: effects on carotid arterial intimal and medial co
Troglitazone 400 mg/day
TZDs: effects on carotid arterial intimal and medial co
Troglitazone 400 mg/day Study Purpose
Study Purpose Subjects (I)
Subjects (I) Subjects (II)
Subjects (II) Study design and Method
Study design and Method Baseline Characteristics
Baseline Characteristics Medications
Medications Baseline Angiographic
Baseline Angiographic  Post-stenting Angiographic Data
Post-stenting Angiographic Data Follow-up Biochemical
Follow-up Biochemical  Follow-Up Angiographic Data
Follow-Up Angiographic Data Clinical Follow-Up Data
Clinical Follow-Up Data The Effects of Rosiglitazone
The Effects of Rosiglitazone  at 48 weeks (mm)
at 48 weeks (mm) Conclusion
Conclusion