Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
11310 hope nebulizer 1208
HOSPITAL: Respiratory Care Services Policy and Procedure Manual
Policy and Procedure Title: HOPE™ Continuous Nebulizer Protocol Area: Respiratory Care Services Performed by: Respiratory Care Practitioners Policy Number: Approved by: Current Effective Date Approved by: Review Date Approved by: Revised Date Approved by:
POLICY This policy assures the standardized use of the HOPE Continuous Medication Nebulizer for use in the delivery of aerosolized medications and diagnostic formulations with a 230 ml reservoir. PURPOSE The purpose is to provide for an easily implemented protocol to be used by the Respiratory Care Practitioner with effective guidelines and consistent instruction for use in the delivery of continuous nebulization to patients that are in a closely monitored area in the hospital. DEFINITION The HOPE Nebulizer is a high output nebulizer to be used to deliver aerosolized medication and diagnostic formulas. It provides additional hydration to help loosen secretions for patients whom therapy is indicated. Heliox, air or oxygen may be added via the multi gas inlet.
SETTINGS To ensure patient safety the device is intended to be used under medical supervision in the hospital, emergency department, extended care and inpatient and outpatient clinics. INDICATIONS 1.
Provide Long term bronchodilation for patients with serious Asthma, Exacerbation of COPD,
B&B HOPE™ Continuous Medication Nebulizer Policy and Procedure ● 2008 B&B Medical Technologies
EQUIPMENT B&B HOPETM Nebulizer (P/N 11310), Oxygen and/or medical grade air at 50 psi, Blender, Oxygen Analyzer with Alarm, Aerosol Tubing, Mask or other delivery device, Cardiac monitor (if indicated) and Pulse Oximeter (if indicated). The B&B Heliox regulator (P/N 11370) can be used for the delivery of 80/20 Helium-Oxygen Gas Mixture.
PROCEDURE A: Application/Preparation Steps 1.
Therapy should be initiated in the ER, Critical Care Unit, and Pediatric Critical Unit or in an
area in which the patient's EKG may be monitored continuously.
After an order has been received, the therapist is to verify the order in the patient's chart.
The treatment must be reordered every 24 hours by a physician.
After checking the patient's ID, the therapist is to explain the procedure to the patient and
answer any questions the patient may have.
Wash hands and assess patient's heart rate, breath sounds, respiratory rate, peak flow,
color, use of accessory muscles, patient's oxygen needs (current ABG) or Sa02.
Set up a continuous pulse oximeter to establish baseline saturation and monitor the patient.
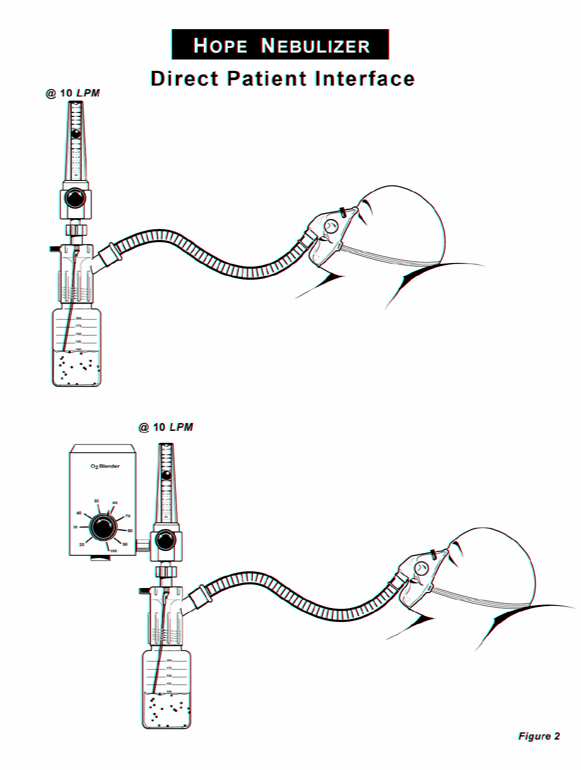
Attach the HOPE Nebulizer to the flowmeter or blender (Figure 2).
Attach the corrugated tubing to the HOPE nebulizer output and to the aerosol mask or other
B: Application/Action Steps 1.
PREPARE MEDICATION per protocol of this policy (Section E).
Pour medication into the HOPE nebulizer reservoir using aseptic technique.
Set flow meter to 10 liters per minute and adjust Fi02 per chart or Blender to meet patient
needs after attaching appropriate size mask to the patient.
Monitor the patient for adverse reactions and check the HOPE nebulizer every 30 minutes x
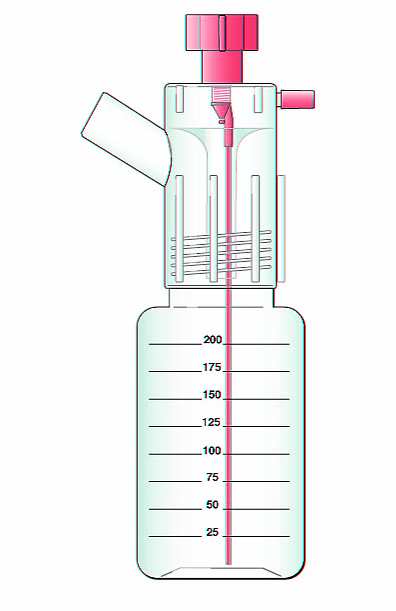
To determine approximate use of medication, look at the marks on the side of the nebulizer
(marks on nebulizer are in 25 ml increments). Adjust the flowmeter by small increments to
achieve desired output of 25 ml/hour, without auxiliary flow.
When using auxiliary flow output increases. Mix one more hour of medication to
C: Application/ Patient Assessment 1.
Monitor the patient’s Pulse before, during treatment, every 30 minutes x 2 hours, then
Assess Breath sounds before, during and post treatment.
Assess patient with Pulse oximeter before, during and post treatment.
In pediatrics, a TCM may be used to monitor patient pre, during and post treatment to
Measure Peak Flow rates before treatment, during treatment every hour x2, then every 2
Document Subjective statements by patient.
Monitor and document patient position, color and level of cooperation.
Monitor and document complications or problems noted during therapy.
B&B HOPE™ Continuous Medication Nebulizer Policy and Procedure ● 2008 B&B Medical Technologies
Measure and monitor Electrolyte levels at physician discretion, if patient is receiving agonist
Reevaluate the patient after initial 2 hours of therapy for possible decrease in drug
D: Documentation/Charting 1.
Check the patient and document the following information every 30 minutes for the first 2
hours, then every 2 hours on the Patient Flow Sheet
E: Prepare Medication Protocol This protocol is a guide to the preparation of medication. Physician orders as to medication content and strength must be on the chart prior to start of Continuous Bronchodilator Nebulization Therapy (CBNT). It is inherent to this therapy that the patient may need to have the dosages changed several times after the initiation of this procedure. The therapist must be aware of the signs that indicate the need for dosage change and alert the physician to any change in the patient's status. Guidelines based upon the dosing chart included with the HOPE Nebulizer: 1.
Initial Gas flow consideration is 10 lpm of 100% source gas driving the nebulizer
The medication delivery is based on physician prescription for mg/hr or ml/hr of
Mg/hr of medication ordered x 0.2 = ml of medication used per hour.
Output of nebulizer - ml of medication = ml of diluent (normal saline)
Multiply diluent and medication times hours you want to deliver; up to 8 hours @ 10 lpm
(maximum volume of nebulizer is 220 ml).
SAMPLE MEDICATION CALCULATION: SEE Dosing Chart on back of HOPE Nebulizer Instruction Sheet. This is a sample calculation. Ideally, when setting up CBNT, the initial fill and dosage should be for 3 hours.
MEDICATION + DILUENT = OUTPUT OF NEBULIZER (25 ml/hr. @ 10 lpm)
Albuterol 0.5% (5 mg = 1 ml, 10 mg=2 ml, 15 mg=3 ml, 20 mg=4 ml)
Dosage recommendations
B&B HOPE™ Continuous Medication Nebulizer Policy and Procedure ● 2008 B&B Medical Technologies
The use of other than the above bronchodilators for the CBNT for severe bronchospasm should be reviewed by the physician in regards to the following criteria. The ideal drug for this form of therapy has high efficacy with side effects which are both infrequent and benign. The drug may not have metabolites, which are bronchoconstrictors. The pulmonary deposition of drug is dependent upon the following: A.
The drug concentration in the aerosol mist.
The patient's minute volume and respiratory rate.
Other physical factors such as the inspiratory flow rate, airway diameter and route of
Initially, patients with severe bronchospasm may have reduced tidal and minute volumes, as well as decreased airway diameters. The reduced volumes in combination with high inspiratory flow rates and narrow airways can lead to a marked reduction in the amount of drug deposited in the lungs. In this situation, a stronger dose is needed to achieve bronchodilation. High doses may lead to side effects as the patient "opens up". When the patient improves, their minute volume and airway diameters may increase and their inspiratory flow rates decrease. The resulting increase in the amount of drug being deposited in the lungs may lead to side effects such as nausea, vomiting, tachycardia and a decreased electrolyte levels (K+ in particular). To avoid this, the patient should be reassessed often and the dose reduced as improvement is noted. F: Contraindications: 1.
Increased heart rate of >25 beats or as defined by the physician.
G: Treatment Complications: A complete reassessment is indicated any time the patient vomits. Failure may include, but is not limited to the following: 1.
Failure to significantly respond in 4 hours.
Decreasing aeration over time or increased wheezing without a simultaneous increase in
Decreasing pulse oximeter readings or an increasing need for higher Fi02’s to maintain the
Anything that leads you to believe, through your patient assessment, that the patient is
When treatment failure is suspected, re-evaluate the patient and contact the physician
H: Precautions and Adverse Events 1.
Exhaled aerosol or patient coughing may spread active pulmonary infections.
The HOPE Nebulizer is intended for single patient use.
B&B HOPE™ Continuous Medication Nebulizer Policy and Procedure ● 2008 B&B Medical Technologies
PROCEDURE A. Fi02 CHART IMPORTANT: Use oxygen analyzer to verify Fi02 IMPORTANT: Auxiliary flowincreases nebulizer output, mix one more hour of medication.
PROCEDURE A. Heliox Therapy Using 80/20 Heliox: 50% Fi02 50% Helium 1.
Set the Primary gas delivery at 10 lpm oxygen. Auxiliary gas 80/20 Heliox at 17 lpm or
15 lpm on the B&B Medical preset Heliox regulator
For every hour of medication delivery, mix 2 hours of solution.
Use alarmed oxygen analyzer to titrate nebulizer output to 50% Fi02.
IMPORTANT: Use oxygen analyzer to verify Fi02 IMPORTANT: Auxiliary flowincreases nebulizer output, mix one more hour of medication. B. Guidelines for Auxiliary Flow and Nebulizer Output With the addition of auxiliary flow (lpm), the out put of the nebulizer increases. The Hope Output Chart provides guidelines with average output in ml per liter of gas delivered to the patient. This chart provides the approximation of change in time for delivery of the medication along with average output of the medication delivered to the patient.
B&B HOPE™ Continuous Medication Nebulizer Policy and Procedure ● 2008 B&B Medical Technologies
Source Gas Auxiliary Flow Hope Nebulizer
B&B HOPE™ Continuous Medication Nebulizer Policy and Procedure ● 2008 B&B Medical Technologies
Reference Articles: Continuous Medication Nebulization Therapy
1.
Moler FW, Hurwitz ME, Custer JR. Improvement in Clinical Asthma Score and PaCO2 in `
Children with Severe Asthma Treated with Continuously Nebulized Terbutaline.
J Allergy Clin Immunol 988; 81:1101-1109
Portnoy J, Aggarwal J. Continuous Terbutaline Nebulization for Treatment of Severe
Robertson CF, Smith F, Bech R, Levison H. Response to Frequent Low Doses of Nebulized
Schuh S, Parker P, Najon A, Carry G, et al. High versus Low Dose Frequency Administered
Nebulized Albuterol in Children with Severe Acute Asthma.
Thivierge BM, et al. Effects of continuous inhalation of Salbutamol in Acute Asthma.
Calacone A, et al. Continuous Nebulization of Albuterol in Acute Asthma.
Chipps BE et al. Vortran High Output Extended Aerosol Respiratory Therapy (HEART) for
delivery of Continuously Nebulized Terbutaline for the Treatment of Acute Bronchospasm.
Pediatric Asthma, Allergy & Immunology 1990; 4: 271-277
Standing C, McCoy K, Hoppe M. Continuous vs Intermittent Aerosolized Albuterol in the
Pediatric Emergency Care 1989; 5 (4): 289 (abstract)
Bodenhamer J et al. Frequently Nebulized Beta Agonists for Asthma: Effects on Serum
Rudnitsky G, Spivey WH et al Comparison of Intermittent and Continuously Nebulized
Albuterol for Treatment of Asthma in a Urban ED. (Abstract)
Colacone A, Wolkove N et al. Safety and Efficacy of Continuous Nebulization of Salbutamol
in Initial Emergency Treatment of Asthma.
Am Rev Respir Dis 1989; 139 (4): a-431 (abstract)
Lin, R.Y. et al. Continuous versus Intermittent Albuterol Nebulization in the treatment of
Papo MC MD, et al. A Prospective, Randomized Study of Continuous Versus Intermittent
Nebulized Albuterol for Severe Status Asthmaticus in Children.
Fink JB, Dhand R. Secondary flow of air and Heliox through a closed dilution nebulizer
improves bronchodilator delivery. Respiratory Care 1998; 11
Fink JB. Helium-Oxygen: An Old Therapy Creates New Interest.
Journal for Respiratory Care Practitioners 1999; April/May: P-71
Lu TS et al. Helium-oxygen in upper airway obstruction. Anesthesiology 1976; 45:678-680
B&B HOPE™ Continuous Medication Nebulizer Policy and Procedure ● 2008 B&B Medical Technologies
Do You Know. Alcohol Street names: booze, sauce, drink What is it? Alcohol is a ―depressant‖ drug. That means it slows down the parts of your brain that affect your thinking and behaviour, as well as your breathing and heart rate. The use of alcohol has been traced as far back as 800 BC, and is common in many cultures today. Where does alcohol come from? Alcohol is produced
Kraut der Unsterblichkeit (Gynostemma pentaphylum) Andere Namen: Xiancao in China, Amachazuru in Japan. Über diese Pflanze wurde schon 1400 n. Christus berichtet. Sie gehört zu den Pflanzen in der traditionellen chinesischen Medizin. In Südchina wird dieses Kraut täglich als Tee getrunken und die Anzahl der Menschen in der Region Guizhou, die dort über 100 Jahre alt werden, ist überdurc
 Source Gas
Source Gas