Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Criticalcarenutrition.com
5.2 Strategies to Optimize Delivery and Minimize risks of EN: Motility agents January 31st 2009
Recommendation: Based on 1 level 1 study and 5 level 2 studies, in critically ill patients who experience feed intolerance (high gastric residuals, emesis), we recommend the use of a promotility agent. Given the safety concerns associated with erythromycin, the recommendation is made for metoclopramide. There are insufficient data to make a recommendation about the use of combined use of metoclopramide and erythromycin. Discussion: Subsequent to an earlier systematic review that looked primarily at the effects of motility agents on gastric emptying and feed intolerance (1), additional randomized
trials that report on clinical outcomes have been published. We have focused on those studies that report clinical outcomes (mortality, infection, length of stay) as well as evaluate
the impact of motility agents on measures of nutritional adequacy. Recent data from a non-randomized observational study showed that ICU patients with high gastric residual
volumes have delayed gastric emptying and that by initiating prokinetic therapy, this accelerates gastric emptying to resemble that of patients tolerating EN (2). The committee noted the lack of treatment effect on clinical outcomes from these trials, however the beneficial effects of motility agents on feed intolerance and nutritional adequacy were
recognized and thought to be important. In five out of the six trials, motility agents were associated with a significant improvement in nutritional intake. Due to the concerns re:
bacterial resistance, the potential for cardiac toxicity and tachyphylaxis with the use of erythromycin and the uncertainty around the safety and efficacy of naloxone as a motility
agent, it was agreed that the recommendation be made for metoclopramide. Given the low probability of harm, the favourable feasibility and cost considerations and the benefits of motility agents in improving nutrient intake, particularly when initiating early EN, the committee decided that motility agents be considered as a strategy to optimize nutrient
(1) Booth CM, Heyland DK, Paterson WG. Gastrointestinal promotility drugs in the critical care setting: a systematic review of the evidence. Crit Care Med. 2002 Jul;30(7):1429-35 (2) Landzinski James et al .Gastric motility function in critically ill patients tolerant vs. intolerant to gastric nutrition. JPEN 2008;32:45-50,2008.
Definition 0, 1, 2 or 3 Effect size
Magnitude of the absolute risk reduction attributable to the intervention listed—a higher score indicates a larger effect size
2 (nutrition adequacy) Confidence interval
95% confidence interval around the point estimate of the absolute risk reduction, or the pooled estimate (if more than one trial)—a
higher score indicates a smaller confidence interval
Validity
Refers to internal validity of the study (or studies) as measured by the presence of concealed randomization, blinded outcome
adjudication, an intention to treat analysis, and an explicit definition of outcomes—a higher score indicates presence of more of these
Homogeneity or
Similar direction of findings among trials—a higher score indicates greater similarity of direction of findings among trials
Reproducibility Adequacy of control
Extent to which the control group represented standard of care (large dissimilarities = 1, minor dissimilarities=2, usual care=3)
group Biological plausibility Consistent with understanding of mechanistic and previous clinical work (large inconsistencies =1, minimal inconsistencies =2, very Generalizability
Likelihood of trial findings being replicated in other settings (low likelihood i.e. single centre =1, moderate likelihood i.e.
multicentre with limited patient population or practice setting =2, high likelihood i.e. multicentre, heterogenous patients,
Estimated cost of implementing the intervention listed—a higher score indicates a lower cost to implement the intervention
Feasible
Ease of implementing the intervention listed—a higher score indicates greater ease of implementing the intervention in an
Estimated probability of avoiding any significant harm that may be associated with the intervention listed—a higher score
5.2 Strategies to Optimize Delivery and Minimize risks of EN: Motility agents January 31st 2009 Question: Compared to standard practice (placebo), does the routine use of motility agents improve clinical outcomes in critically ill patients? Summary of Evidence: There was one systematic review that reported on surrogate outcomes such as gastric emptying and feed intolerance (Booth et al 2002) and 4 level 2 studies and 1 level 1 study that reported on clinical outcomes. In addition, there were 1 level 1 and 3 level 2 studies
that reported on nutritional endpoints. Of the total of 9 studies included, 6 studies looked at the use of a single motility agent compared to placebo. Of these, 3 studies compared erythromycin to placebo (Chapman 2000, Berne 2002, Reigner 2002), 2 compared metoclopramide to placebo (Yavagal
2000 and Nursal 2007) and an earlier study compared the use of enteral naloxone to placebo (Meissner 2003). The data from three additional studies was not included in the meta-analysis as the interventions varied (MacLaren 2008 erythromycin vs. metoclopramide; Nguyen 2007
erthryomycin plus metoclopramide vs. erythromycin alone; Biovin 2001 erythromycin vs. small bowel feeding) (Nguyen 2007). Given the uncertainty around the safety and efficacy of naloxone as a motility agent, the data from the Meissner 2003 study was not included.
Mortality: When the data from the five studies of metoclopramide and erythromycin alone were aggregated, the use of motility agents had no effect
on mortality (RR = 1.03, 95% CI 0.85, 1.26, p =0.75, no heterogeneity present) (figure 1). Infections: In the one study using naloxone, there was a significant reduction in pneumonia (Meissner 2003) and in the other study, metoclopramide had no effect on the incidence of pneumonia (Yavagal 2000). One study reported on the number of infections per group rather than
the number of patients with infections and again there were no differences between the two groups (Berne 2002). LOS, Ventilator days: There were no differences between the groups in the 3 studies that reported on these outcomes (Meissner 2003, Nursal 2007 and Nguyen 2007). Other: The time to development of pneumonia was statistically different in the one study (Yavagal) (5.95 days versus 4.46 days, p=0.006), however,
the clinical significance of this difference is negligible. All studies demonstrated positive effects on nutrition indices i.e. lower gastric residual volumes, fewer interruptions in feeds, higher % feeds tolerated, fewer days to target calories, with the exception of 2 studies (Boivin 2001, Nursal
2007) in which there were no significant differences seen. The combined approach of erythromycin plus metoclopramide resulted in a significant higher calorie intake, lower gastric residual volumes and lower need for post pyloric feeds (Nursal 2007).
Conclusion:
1) Motility agents have no effect on mortality or infectious complications in critically ill patients.
2) Motility agents may be associated with an increase in gastric emptying, a reduction in feeding intolerance and a greater caloric intake in critically
ill patients. Level 1 study: if all of the following are fulfilled: concealed randomization, blinded outcome adjudication and an intention to treat analysis. Level 2 study: If any one of the above characteristics are unfulfilled. Table 1. Randomized Studies Motility Agents In Critically Ill Patients Population Intervention Mortality # (%)† Infections # (%)‡ Nutritional Indices Experimental Control Experimental Control Experimental Control Placebo-controlled trials 1) Chapman Mixed ICU patient C.Random: Yes Erythro 200 mg IV vs Successful feeding defined as GRV <250 mo and continuing with feeds. 2) Yavagal Feeds tolerated at 48 hrs Feeds tolerated for the study 4) Reignier EN discontinued if GRV>250 or vomited: Feeding volumes after day 3 Meissner** Amount of Reflux (mls) 6) Nursal Hospital Hospital Patients with high GRV Days to target calories Calorie intake/total calories Head to Head Comparisons 7) MacLaren Mixed ICU patient Both agents resulted in significant reduction in GRV and increase in feeding rate Combo vs Mono Failure of feeding (days) 8) Nguyen Hospital Hospital Caloric intake % prescribed 7 days Gastric residual volumes Need for post-pyloric feeds Motility agent vs Small bowel tubes 9) Boivin No difference in time to goal rate or overall adequacy.
* infections reported as per group, not # patients with infections
**data from this study not included in the meta-analysis due to the uncertainty around the safety and efficacy of naloxone as a motility agent.
Figure 1. TOPIC: 5.2. Motility Agents Article inclusion log Criteria for study selection Type of study: RCT or Meta-analysis Population: Critically ill, ventilated patients (no elective surgery patients) Intervention: Motility agents (exclude Cisapride) Outcomes: Mortality, LOS, QOL, functional recovery, complications, and measures of nutritional adequacy. Exclude if just report measures of gastric emptying.
Rejected References
Dive A, Miesse C, Galanti L, Jamart J, Evrard P, Gonzalez M, Installe E. Effect of erythromycin on
gastric motility in mechanically ventilated critically ill patients : A double-blind, randomized, placebo-controlled study. Crit Care Med 1995;23(8):1356-1362.
Spapen HD, Duinslaeger L, Diltoer M, Gillet R, Bossuyt A, Huyghens L. Gastric emptying in
critically ill patients is accelerated by adding cisapride to a standard enteral feeding protocol: Results of a prospective, randomized, controlled trial. Crit Care Med 1995;23(3):481-485.
Heyland DK, Tougas G, Cook DJ, Guyatt GH. Cisapride improves gastric emptying in mechanically
ventilated, critically ill patients. Am J Respir Crit Care Med 1996;154:1678-1683.
Williams A. The effect of cisapride on gastric stasis in intensive care patients. Br J Intensive Care 1996;6:186-193.
Altomare DF, Rubini D, Pilot MA, Farese S, Rubini G, Rinaldi M, Memeo V, D’Addabbo A. Oral
erythromycin improves gastrointestinal motility and transit after subtotal but not total gastrectomy for cancer. Br J Surg 1997;84:1017-1021.
Goldhill DR, Toner CC, Tarling MM, Baxter K, Withington PS, Whelpton R. Double-blind,
randomized study of the effect of cisapride on gastric emptying in critically ill patients. Crit Care Med. 1997 Mar;25(3):447-51. Comment in: Crit Care Med. 1998 Jan;26(1):188-9.
Jooste CA, Mustoe J, Collee G. Metoclopramide improves gastric motility in critically ill patients.
Chapman MJ, Fraser RJ, Kluger MT, Buist MD, De Nichilo DJ. Erythromycin improves gastric emptying in critically ill patients intolerant of nasogastric feeding. Crit Care Med. 2000
Jul;28(7):2334-7. Comment in: Crit Care Med. 2000 Jul;28(7):2657-9.
MacLaren R, Kuhl DA, Gervasio JM, Brown RO, Dickerson RN, Livingston TN, Swift K, Headley S, Kudsk KA, Lima JJ. Sequential single doses of cisapride, erythromycin, and metoclopramide in
critically ill patients intolerant to enteral nutrition: A randomized, placebo-controlled, crossover study. Crit Care Med 2000;28(2):438-444.
Yavagal DR, Karnad DR, Oak JL: Metoclopramide for preventing pneumonia in critically ill patients receiving enteral tube feeding: A randomized controlled trial. Crit Care Med 2000;May;28(5):1408-11.
Boivin MA, Levy H. Gastric feeding with erythromycin is equivalent to transpyloric feeding in the critically ill. Crit Care Med. 2001 Oct;29(10):1916-9.
van der Spoel JI, Oudemans-van Straaten HM, Stoutenbeek CP, Bosman RJ, Zandstra DF. Neostigmine resolves critical illness-related colonic ileus in intensive care patients with multiple organ failure--a prospective, double-blind, placebo-controlled trial. Intensive Care Med. 2001
Berne JD, Norwood SH, McAuley CE, Vallina VL, Villareal D, Weston J, McClarty J. Erythromycin reduces delayed gastric emptying in critically ill trauma patients: a randomized, controlled trial. J
Booth CM, Heyland DK, Paterson WG. Gastrointestinal promotility drugs in the critical care setting: A systematic review of the evidence. Crit Care Med 2002;Jul;30(7):1429-35.
Reignier J, Bensaid S, Perrin-Gachadoat D, Burdin M, Boiteau R, Tenaillon A.Erythromycin and
early enteral nutrition in mechanically ventilated patients. Crit Care Med 2002;Jun; 30(6): 1237-41.
Chapman M, Fraser R, de Beaux I, Creed S, Finnis M, Butler R, Cmielewski P, Zacharkis B, Davidson G. Cefazolin does not accelerate gastric emptying in the critically ill. Intensive Care Med
Griffith DP, McNally AT, Battey CH, Forte SS, Cacciatore AM, Szeszycki EE,Bergman GF, Furr CE, Murphy FB, Galloway JR, Ziegler TR. Intravenous erythromycin facilitates bedside placement
of postpyloric feeding tubes in critically ill adults: a double-blind, randomized, placebo-controlled study. Crit Care Med 2003 Jan; 31(1):39-44.
Marino LV, Kiratu EM, French S, Nathoo N. To determine the effect of metoclopramide on gastric
emptying in severe head injuries: a prospective, randomized, controlled clinical trial. Br J Neurosurg 2003 Feb;17(1):24-8.
Meissner W, Dohrn B, Reinhart K. Enteral naloxone reduces gastric tube reflux and frequency of
pneumonia in critical care patients during opioid analgesia. Crit Care Med 2003 Mar; 31(3):776-80.
Ritz MA, Chapman MJ, Fraser RJ, Finnis ME, Butler RN, Cmielewski P, Davidson GP, Rea D. Erythromycin dose of 70 mg accelerates gastric emptying as effectively as 200 mg in the critically
ill. Intensive Care Med. 2005 Jul;31(7):949-54. Epub 2005 Jun 7.
Sustić A, Zelić M, Protić A, Zupan Z, Simić O, Desa K. Metoclopramide improves gastric but not gallbladder emptying in cardiac surgery patients with early intragastric enteral feeding: randomized
controlled trial. Croat Med J. 2005 Apr;46(2):239-44.
Nguyen NQ, Chapman M, Fraser RJ, Bryant LK, Burgstad C, Holloway RH. Prokinetic therapy for feed intolerance in critical illness: One drug or two? Crit Care Med 2007;35(11):2561-2567.
Nursal TZ, Erdogan B, Noyan T, Cekinmez M, Atalay B, Bilgin. The effect of metoclopramide on
gastric emptying in traumatic brain injury. J Clin Neurosurg 2007;14:344-348.
MacLaren R, Kiser TH, Fish DN, Wischmeyer PE. Erythromycin vs metoclopramide for facilitating gastric emptying and tolerance to intragastric nutrition in critically ill patients. JPEN J Parenter
Accord national médico-mutualiste 2009–2010 ACCORD NATIONAL MEDICO-MUTUALISTE 2009–2010 En vertu des articles 26, 50 et 51 de la loi relative à l’assurance obligatoire soins de santé et indemnités, coordonnée le 14 juillet 1994, la Commission nationale médico-mutualiste (dénommée ci-après CNMM), sous la Présidence de M. Johan DE COCK, a conclu le 17 décembre 2008, l’accord
Promising Phase II Data For New Parkinson's Disease Drug Presented 22 Mar 2013 A new levodopa product (ODM-101) developed by Orion Corporation could improve the treatment of advanced Parkinson's disease patients. According to a Phase II study, presented yesterday at American Academy of Neurology's Annual Meeting in San Diego, ODM-101 significantly decreased daily OFF-time without increasing
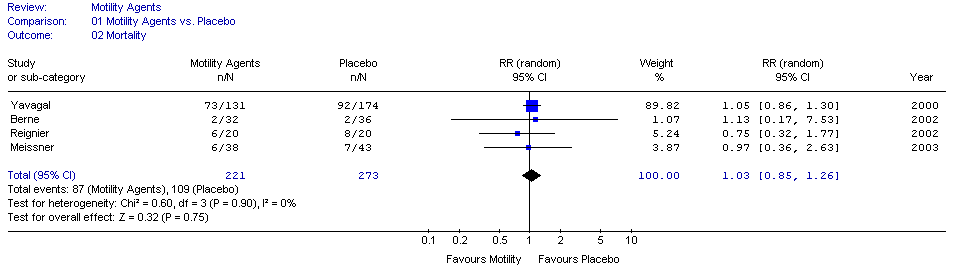 Figure 1.
Figure 1.