Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Dlin.web.unc.edu
Cyclosporine or Cyclosporine Plus Methylprednisolone for Prophylaxis of Graft-Versus-Host Disease: A Prospective, Randomized Trial
By H. Joachim Deeg, Danyu Lin, Wendy Leisenring, Michael Boeckh, Claudio Anasetti, Frederick R. Appelbaum,
Thomas R. Chauncey, Kristine Doney, Mary Flowers, Paul Martin, Richard Nash, Gary Schoch, Keith M. Sullivan,
Patients with a lymphohematopoietic malignancy consid- difference was seen for grades III-IV GVHD. However, chronic ered to be at high risk for posttransplant relapse were en- GVHD occurred somewhat more frequently in patients re- rolled in a study to compare the use of cyclosporine (CSP) ceiving CSP plus MP (44%) than in patients receiving only as a single agent with a combination of methylprednisolone CSP (21%; P ! .02). The incidence of de novo chronic GVHD (MP) and CSP for graft-versus-host disease (GVHD) prophy- was marginally higher in patients receiving CSP plus MP (P ! laxis after marrow transplantation from an HLA-identical sib- .08). No significant differences in the risk of infections ling donor. Sixty patients were randomized to receive CSP were observed. There was a suggestion that the risk of re- only and 62 were randomized to receive CSP plus MP. Daily lapse was lower in patients receiving CSP plus MP (P ! .10) CSP was started on day Ï1 (5 mg/kg/d intravenously) and and, although the overall survival in the two groups was not administered at gradually reduced doses until day 180. MP different (P ! .44), there was a slight advantage in favor of was started on day 7 at 0.5 mg/kg/d, increased to 1.0 mg/ CSP plus MP-treated patients for relapse-free survival (P ! kg/d on day 15, started on a taper schedule on day 29, and .07). These results suggest that prophylactic MP, when com- discontinued on day 72. All 104 evaluable patients (surviving bined with CSP, has only limited efficacy in acute GVHD
ı28 days) had sustained engraftment. The incidence rates prevention and may increase the probability of chronic of grades II-IV acute GVHD were 73% and 60% for patients receiving CSP and CSP plus MP, respectively (P ! .01). No
᭧ 1997 by The American Society of Hematology. CYCLOSPORINE (CSP) HAS been used clinically for infection,10 although this was not the case in an earlier
almost 2 decades. Although introduced with high ex-
study.11 The combination of CSP plus prednisone has never
pectations into the practice of marrow transplantation, the
been compared in a prospective randomized study to single-
efficacy of CSP as a single agent for the prevention of graft-
agent CSP. Such a study is of interest for several reasons.
versus-host disease (GVHD) was not superior to that of a
(1) Although the addition of methylprednisolone (MP) to
then standard regimen of intermittent methotrexate (MTX).1-3
CSP may decrease the incidence of GVHD, it may add to
However, second generation studies showed a significant
toxicity and, as a result, fail to improve overall outcome.12
reduction in the incidence of acute GVHD and improved
(2) Earlier noncontrolled studies suggested that the use of
survival when CSP was administered in combination with
MP increased the probability of developing chronic
MTX.4-6 One disadvantage of the combined regimen was that
GVHD.12,13 (3) At least one study comparing CSP plus MTX
the myelosuppressive effect of MTX delayed hematopoietic
to CSP combined with MTX plus MP showed a decreased
recovery as compared with results with CSP alone.4,5 In addi-
incidence of relapse with the incorporation of MP.12 There-
tion, it has been suggested that prevention of acute GVHD
fore, we performed a prospective randomized study compar-
may be associated with an increased probability of leukemic
ing a combination of CSP plus MP with single-agent CSP
relapse.7 Other investigators combined CSP plus predni-
for GVHD prophylaxis in patients considered at high risk
sone.8,9 This combination allowed for more rapid hematopoi-
of recurrent malignancy posttransplant.
etic recovery compared with MTX-containing regimens, al-
beit at the price of a higher incidence of GVHD than seenwith MTX plus CSP.5,6 Also, evidence has been presented
that the addition of prednisone may increase the risk of
From September 1991 through July 1994, 123 patients considered
at high risk for posttransplant relapse were registered on this proto-col. This included patients with lymphoid and myeloid malignancies
From the Fred Hutchinson Cancer Research Center, Seattle, WA;
who were not in remission (relapse or resistant disease) and with
the Veterans Administration Medical Center, Seattle, WA; and the
lymphoid malignancies in third or subsequent remission or with
Departments of Medicine and Biostatistics, University of Washing-
myeloid leukemia in second or subsequent remission. One patient
(unique patient number 7559) declined a transplant after randomiza-
Submitted September 30, 1996; accepted January 8, 1997.
tion. Characteristics of the remaining 122 patients (followed for 17.5
Supported by Public Health Service Grants No. CA15704,
to 59 [median, 41] months) are shown in Table 1. Seven stratification
CA18029, CA18221, and HL36444 from the National Institutes of
variables were considered: diagnosis (myeloid v lymphoid), disease
Health, Department of Health and Human Services, Bethesda, MD.
stage (remission v relapse or accelerated phase), age (õ25 years vAddress reprint requests to H. Joachim Deeg, MD, Fred Hutchin-
¢25 years), donor/patient gender, high risk v low risk for posttrans-
son Cancer Research Center, 1124 Columbia St, M318, Seattle, WA
plant relapse,14 conditioning regimen (1,200 cGy total body irradia-
tion [TBI] or none v ú1,200 cGy TBI), receiving intravenous (IV)
The publication costs of this article were defrayed in part by page
Ig (yes v no), and treatment in laminar air flow room (yes v no). As
charge payment. This article must therefore be hereby marked
shown in Table 1, the study arms were balanced with respect to
‘‘advertisement’’ in accordance with 18 U.S.C. section 1734 solely to
these risk factors. Protocol and consent forms were approved by the
Institutional Review Board of the Fred Hutchinson Cancer Research
᭧ 1997 by The American Society of Hematology.
Center (Seattle, WA). Risks and benefits of treatment regimens were
explained to each patient in detail before hospital admission.
Blood, Vol 89, No 10 (May 15), 1997: pp 3880-3887
Table 1. Patient and Transplant Characteristics
patients who were discharged to the Outpatient Department receivedoral CSP at a dose of 5 mg/kg twice daily. This dose was continued
through day 83 if no toxicity developed; it was tapered to 4 mg/kg
on day 84, to 3 mg/kg on day 98, to 2 mg/kg twice a day on day120, and continued through day 180. Downward dose adjustments
were made if renal toxicity developed. MP was started on day 7 and
administered through day 14 at a dose of 0.25 mg/kg IV twice daily.
On day 15, the MP dose was increased to 0.5 mg/kg twice daily
and then decreased again to 0.25 mg/kg orally on day 29, to 0.15
mg/kg on day 43, and to 0.1 mg/kg on day 57 through day 72, when
Assessment, grading, and treatment of acute GVHD have been
reported previously.16-19 Acute GVHD was treated by increasing the
dose of MP to 2 mg/kg in patients who had been randomized to
CSP plus MP or by instituting MP in patients randomized to receive
CSP only. The plan was to treat patients for 14 days at the full dose
and then begin to taper steroids. Patients who did not respond to
MP as primary therapy were generally treated with antithymocyte
Patients were evaluated for the presence of chronic GVHD before
discharge from the center as described.17,20,21 Studies included hema-
topoietic and chemical parameters, skin and lip biopsies, Schirmer’s
test, pulmonary function tests, and other examinations as indicated.
Patients with clinical extensive chronic GVHD were treated with
Abbreviations: LAF, laminar air flow room; ALL, acute lymphoblas-
continued immunosuppression. Patients with subclinical disease or
tic leukemia; ANC, acute nonlymphoblastic leukemia; CML, chronic
without evidence of GVHD were observed at regular intervals, and
myelogenous leukemia; NHL, non-Hodgkin lymphoma; MDS, myelo-
therapy was instituted if clinical disease developed.
dysplastic syndrome; CY, cyclophosphamide; BU, busulfan.
* Patients were stratified by disease status.
† Numbers of patients in remission are in parenthesis.
‡ Refractory anemia with excess blasts (RAEB) or RAEB in transfor-
All patients received prophylactic systemic antiviral and antibacte-
rial antibiotics and trimethroprim-sulfamethoxazole for Pneumo-cystis carinii prophylaxis as described.5 Twelve patients were placed
in a laminar air flow room for protective isolation. Ten patients
received intermittent IVIg as part of a concurrent study. In the re-
maining patients, IVIg was administered only when serum IgG levels
The infection data for this analysis were collected prospectively
All donors were HLA-genotypically identical relatives. Serologi-
on coded data sheets for the time interval from day 0 through day
cal (class I) and molecular typing (class II) were performed according
100 and categorized in a blinded fashion (M.B.) as described.10,22
Briefly, bacteremia was defined as one or more positive blood cul-tures with any bacterial organism regardless of associated symptoms. Conditioning Regimens and Transplantation
Any culture record for a given organism within 21 days of an initial
Conditioning regimens are summarized in Table 1. Fractionated
positive blood culture for that organism was considered to represent
irradiation was delivered from two opposing 60Co sources at an
the same infection and was not considered to indicate a new bacter-
exposure rate of 7 cGy/min. Within 4 hours of the last TBI exposure
emia. Blood culture records for a different organism occurring any
or 36 hours after the last dose of chemotherapy, donor marrow was
time after a positive culture for another organism was considered to
infused IV. The marrow cell dose ranged from 0.5 to 6.1 (median,
be a separate bacteremia. Blood culture records for multiple organ-
1.8) 1 108 cells/kg. The day of marrow infusion was designated day
isms on the same day were considered to be a single polymicrobial
0. Engraftment was defined as the first of at least 3 consecutive
bacteremia. Culture records for a micrococcus or non-JK corynebac-
days on which the neutrophil count surpassed 0.5 1 109/L after the
terium species or aerobic diphtheroids were not included in the pres-
ent analysis because they were considered to be contaminants. Organsite infections were identified as positive bacterial cultures from
GVHD Prophylaxis, Assessment, and Treatment
normally sterile sites (eg, sinuses). Fungemia was defined as occur-
All patients received CSP and, in addition, were randomized to
rence of one or more positive blood cultures with any fungal organ-
receive or not to receive MP in a nonblinded fashion; regimens for
ism regardless of associated symptoms. Invasive mold infections
both drugs were identical to those previously described by others.8,15
were defined as biopsy-proven tissue invasion or positive cultures
CSP was administered at doses of 5 mg/kg/d as a continuous IV
as described.22 Analyses were performed considering all infections,
infusion on days 01 through 3 and at 3 mg/kg/d on days 4 through
bacterial infections, fungal infections, and combined invasive fungal,
14. On days 15 through 35, 3.75 mg/kg/d was administered IV;
gram-negative, and polymicrobial infections. Table 2. Incidence of Acute GVHD
The primary response variable in the study design was
the incidence of grades II-IV acute GVHD. Secondary responses tobe analyzed included the development of chronic GVHD, incidence
of infections, relapse, and survival. The CSP arm was expected to
show a 50% incidence of grades II-IV GVHD. For purposes of
this study, reduction to 25% would have been considered clinically
significant. For a test with .05 statistical significance and with power
90% a maximum sample size of 92 patients per arm would be
required.23 An interim analysis was performed as planned upon en-rollment of 71 patients. The estimated incidence rates of acute
GVHD for patients receiving CSP or CSP plus MP were 60% and
44%, respectively, yielding a one-sided P value of .092. These in-
terim results suggested a beneficial effect of the drug combination
but were not strong enough to terminate the study early. Patient
enrollment was therefore continued, but the goal of accruing 92
patients had to be abandoned as a consequence of competing clinical
Log-rank test statistics and Cox models were used in
an analysis by intent to treat for time to event data including acute
and chronic GVHD, survival, relapse, nonrelapse mortality, relapse-
free survival, and infection. A second analysis was performed by
actual treatment, excluding 8 patients in the CSP arm and 7 patients
in the CSP plus MP arm who failed to receive the prescribed treat-
ment based on decisions by the attending physician. For additional
* Log-rank test for overall grading; x2 test for grading by organ.
analysis of the infection data, the Anderson-Gill counting processmodel24 was used, which is an extension of the Cox model thataccommodates multiple events (infection episodes) in the same indi-vidual. Cumulative incidence and conditional probability esti-
risk of developing acute GVHD among patients on CSP was
mates25,26 were used in the analysis of acute and chronic GVHD.
significantly higher than for patients on CSP plus MP for
Kaplan-Meier estimates are presented for disease-free survival. Soft-
any grade (P Å .001) and for grades II-IV (P Å .01) but not
ware package S-plus 3.3 (Mathsoft Inc, Seattle, WA) was used for
for severity grades III-IV (P Å .28). As shown in Table 3,
the Anderson-Gill model, and SAS (SAS Institute Inc, Cary, NC),
results were basically the same in the analysis by actual
Stata (Stata Statistical Software: Release 5.0; Stata Corporation, Col-
treatment. The decision not to administer the GVHD prophy-
lege Station, TX), or Gauss (version 3.2.6; Aptech Systems Inc,
laxis prescribed by randomization was made by the attending
Maple Valley, WA) were used for all other analyses. Results wereanalyzed as of January 1, 1996.
physician. Reasons included mainly concern about steroidadministration to patients who were infected or suboptimal
prophylaxis with CSP as the only drug.
Chronic GVHD developed in 12 of the patients receiving
CSP at 75 to 305 (median, 127) days posttransplant and in
All 104 patients surviving more than 28 days had sus-
25 of the patients receiving CSP plus MP at 75 to 492
tained engraftment; 18 patients who died before day 28 (12
(median, 182) days posttransplant. Thus, the cumulative inci-
and 6 patients on CSP and CSP plus MP, respectively) were
dences were 21% and 44% for patients receiving CSP and
considered unevaluable for engraftment.
CSP plus MP, respectively (Fig 2A). The relative risk ofdeveloping chronic GVHD for patients receiving CSP plus
MP was 2.33 (confidence interval [CI], 1.16, 4.71; P Å .02). The conditional probabilities (conditional on surviving) of
Results are summarized in Tables 2 and 3 and Figs 1 and
developing chronic GVHD for the two groups were 51%
2. The cumulative incidence of grades I-IV acute GVHD
and 94%, respectively (P Å .03; Fig 2B). De novo chronic
was 82% and 66% for patients on CSP and CSP plus MP,
GVHD developed in 1 of 8 patients at risk on CSP (these
respectively (P Å .001, log-rank test). Grades II-IV acute
were the only 8 patients who never received any MP) and
GVHD, the primary endpoint of the study, developed in 44
in 12 of 19 patients at risk on CSP plus MP, respectively;
patients (73%) on the CSP arm at 3 to 67 (median, 10) days
the relative risk was 6.28 (CI, 0.81, 48.4; P Å .08). The
after transplantation, compared with 37 patients (60%) on
pattern was the same in the analysis by actual treatment,
the CSP plus MP arm at 4 to 78 (median, 12) days after
although the differences did not reach significance.
transplantation. Acute GVHD, grades III-IV, developed in24 patients (40%) receiving CSP and 21 patients (34%) re-
ceiving CSP plus MP (Table 2A). Although the incidenceof acute GVHD in patients receiving only CSP was higher
The incidence of clinically relevant infections is summa-
in all target organs, the difference was most striking in the
rized in Table 3. Whereas the numbers of infectious events,
skin (Table 2B). In Cox regression analysis (Table 3), the
particularly fungal infections, appeared to be slightly higher
Table 3. Cox Regression Analysis of Time to Event Data
* Includes gram-negative, fungal, and polymicrobial infections.
in the group of patients receiving CSP plus MP, none of the
patients on the CSP arm and 20 patients the CSP plus MP
differences was statistically significant. This was true for
arm had developed an infection; this difference was not sig-
both the number of patients experiencing infections (first
nificant (relative risk, 0.99; CI, 0.49, 2.0; P Å .98). Similarly,
infection) and the number of episodes (all infections). Be-
in the analysis by actual treatment no significant difference
cause treatment of GVHD involved the use of MP, it was
possible that the therapeutic use of MP in patients originally
randomized to receive CSP only would obscure differencesbetween the two prophylactic groups. Therefore, an addi-
Among CSP-treated patients, 17 had a recurrence of their
tional analysis was performed with censoring of patients at
underlying disease compared with 13 receiving CSP plus
the time of treatment for acute GVHD. By that time, 14
MP prophylaxis (not significant). Relapse tended to occur
Probability of acute GVHD in patients receiving GVHD prophylaxis with CSP alone or CSP plus MP. (A) Acute GVHD grades I-IV (P
! .001); (B) acute GVHD grades II-IV (P ! .01). Chronic GVHD in patients receiving GVHD prophylaxis with CSP alone or CSP plus MP. (A) Probability (P ! .02); (B) conditional probability (P ! .03).
later in patients receiving CSP plus MP, but this difference
versial.8,9,15,31-33 A recent study suggested that the use of MP
was not significant (P Å .10).
concurrently with MTX and CSP increased — rather thandecreased — the incidence of GVHD, leading to the specula-
tion that MP interfered with the antimetabolite MTX, therebyreducing or neutralizing its immunosuppressive effect.12
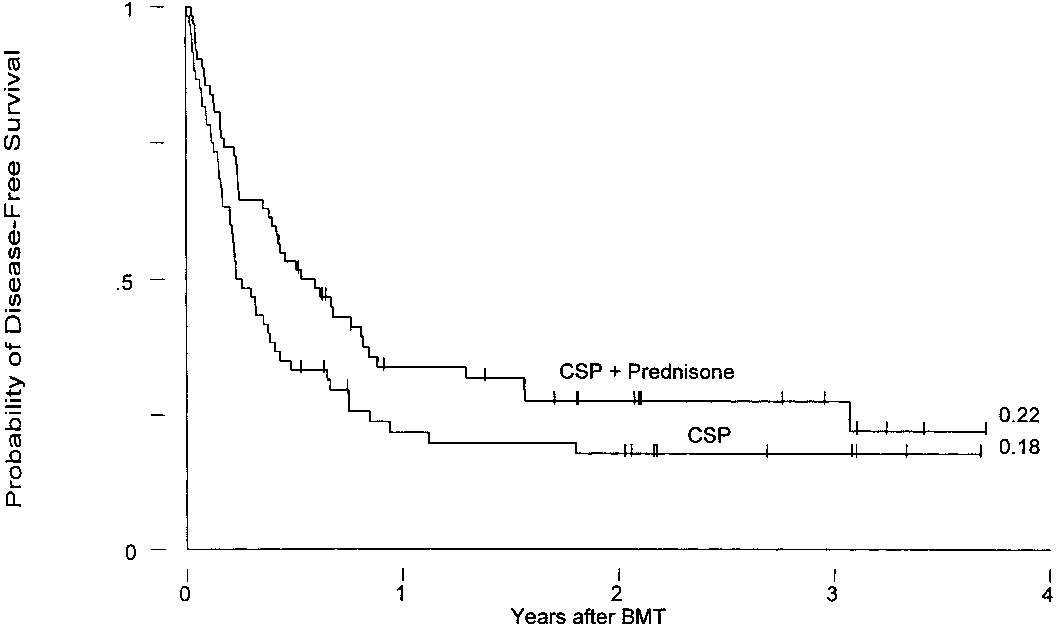
Currently, 36 patients are surviving, 17 who had received
However, it is interesting that, in the same study, patients
CSP and 19 CSP plus MP prophylaxis, for Kaplan-Meier
who had received MP were somewhat less likely to suffer
survival estimates at 3 years of 26% and 23%, respectively
a posttransplant relapse than patients not receiving MP.12 The
(P Å .45). Three-year relapse-free survival estimates for the
objective of the present trial was to compare in a prospective,
two groups are 18% and 22%, respectively (P Å .07; Fig
randomized study single-agent CSP and CSP plus MP in
regard to GVHD prevention and incidence of infection. As
Causes of death are listed in Table 4. There was no differ-
the study population, we chose patients with myeloid or
ence in overall mortality between the two groups and there
lymphoid malignancies who were considered to be at high
was no obvious difference in regard to any particular cause
risk of disease recurrence after transplantation. Because
these patients would be expected to potentially benefit from
a graft-versus-leukemia effect,34-37 not using the standardregimen of CSP plus MTX and accepting a possibly higher
MP has been used extensively in patients undergoing mar-
incidence of GVHD was felt to be acceptable.
row or solid organ transplantation and is considered standardtherapy for treatment of established acute and chronicGVHD.27-30 Several studies have also incorporated MP for
Table 4. Causes of Death
GVHD prophylaxis, but its role for this indication is contro-
Leukemia-free survival in patients receiving GVHD prophy-
Abbreviation: MOS, multiorgan system. laxis with CSP alone or CSP plus MP (P ! .07).
* Disease present at autopsy or within 6 weeks of death.
As suggested by earlier noncontrolled studies,15 the inci-
that patients receiving CSP plus MP had a lower incidence
dence of acute GVHD of all severity grades in the present
of leukemic relapse (P Å .10) and that relapse-free survival
study, although high overall, was lower in patients receiving
was better in the CSP plus MP group than among patients
a combination of CSP plus MP. However, this difference in
receiving CSP only (P Å .07). These results are consistent
overall grading was significant only for mild to moderate
with findings of an earlier trial showing that the addition of
but not for severe (grades III-IV) manifestations of GVHD.
MP to CSP plus MTX resulted in fewer relapses.11 In that
The difference was most striking in the skin, consistent with
study we speculated that MP interfered with the efficacy of
earlier observations that skin manifestations are particularly
MTX and that the resulting increase in GVHD was associ-
responsive to steroids.30 Of note was the rather early onset
ated with a more potent graft-versus-leukemia effect. How-
of skin exanthemas thought to represent GVHD in some
ever, in the present study, the incidence of acute GVHD was
patients. Although it is not possible to exclude the possibility
actually lower in the CSP plus MP group; the incidence of
of nonspecific rashes, the fact that they occurred in both
chronic GVHD was nevertheless increased as compared with
treatment arms suggests that the omission of MTX, currently
patients receiving CSP alone. These data are consistent with
used in most standard regimens,5,6 contributed to this phe-
either a direct antileukemic effect of MP or a graft-versus-
nomenon. This notion is supported by observations in earlier
leukemia effect associated with chronic GVHD.36,37
randomized studies comparing MTX and CSP.1,2
In conclusion, this randomized prospective study shows
GVHD prophylaxis also influenced the development of
that a combination of CSP plus MP is more effective in
chronic GVHD, albeit in a direction opposite to that observed
preventing acute GVHD than CSP alone. The incidence of
with acute GVHD: the incidence of chronic GVHD was
chronic GVHD, on the other hand, was higher in the CSP
higher in CSP plus MP-treated patients than among patients
plus MP group, a finding in support of the notion that MP
receiving CSP only. A difference was still present if patients
is not an effective agent for the prevention of chronic GVHD.
who developed acute GVHD and, therefore, received thera-
However, only very few patients were able to avoid the use
peutic MP even if originally randomized to receive CSP only
of MP completely. There was a suggestion that the prophy-
were censored. The occurrence of de novo chronic GVHD
lactic use of MP resulted in a slight improvement of relapse-
was marginally more likely in patients on CSP plus MP
prophylaxis (P Å .08). The reason for such an effect of MPis not clear. Conceivably, MP, although suppressing an acute
GVHD reaction, interfered with signals required for T-cell
We thank all of the nurses and physicians on the Transplant
selection and the establishment of tolerance.38 As a result,
Wards, the Outpatient Department, and the Long-term Follow-up
host-reactive T cells would initiate GVHD once immunosup-
Office for their contributions and Bonnie Larson and Harriet Childs
pression was tapered or discontinued. Although it is known
for typing the manuscript. Special thanks to Russ Schwartz and the
that acute GVHD represents a major risk factor for the subse-
staff of the Microbiology Laboratory for compiling the bacterial and
quent development of chronic GVHD,39,40 the present results
suggest that the prophylactic use of MP, even though effec-tive in reducing the incidence of acute GVHD, does not
provide prophylaxis for chronic GVHD.
1. Deeg HJ, Storb R, Thomas ED, Flournoy N, Kennedy MS,
A previous prospective trial in patients receiving MTX
Banaji M, Appelbaum FR, Bensinger WI, Buckner CD, Clift RA,
plus CSP and randomized to receive or not to receive MP
Doney K, Fefer A, McGuffin R, Sanders JE, Singer J, Stewart P,
as GVHD prophylaxis had shown a significantly higher prob-
Sullivan KM, Witherspoon RP: Cyclosporine as prophylaxis for
ability of infection in patients on MP.10 In the present study,
graft-versus-host disease: A randomized study in patients undergoing
the probabilities of fungal and bacterial infections were simi-
marrow transplantation for acute nonlymphoblastic leukemia. Blood65:1325, 1985
lar in the two groups. There may be several reasons for the
2. Storb R, Deeg HJ, Thomas ED, Appelbaum FR, Buckner CD,
discrepancy between previous and present results. For one,
Cheever MA, Clift RA, Doney KC, Flournoy N, Kennedy MS, Loug-
the MP dose in the present study was lower (0.5 mg/kg/d v
hran TP, McGuffin RW, Sale GE, Sanders JE, Singer JW, Stewart
1 mg/kg/d) in the early posttransplant period. Secondly, the
PS, Sullivan KM, Witherspoon RP: Marrow transplantation for
use of MTX in the previous (but not in the current) study
chronic myelocytic leukemia: A controlled trial of cyclosporine ver-
might impair mucosal integrity, thereby facilitating the de-
sus methotrexate for prophylaxis of graft-versus-host disease. Blood
velopment of invasive infections, an effect that may have
been amplified by the addition of MP. The lack of a signifi-
3. Deeg HJ: Chemoprevention of graft-vs-host disease: Effects
cant difference between CSP and CSP plus MP-treated pa-
on donor marrow and host environment, in Gale RP, Champlin RE(eds): Bone Marrow Transplantation: Current Controversies. New
tients in the present study was not explained by the therapeu-
tic use of MP: results were indistinguishable (P Å .98) when
4. Deeg HJ, Storb R, Weiden PL, Raff RF, Sale GE, Atkinson
patients receiving therapeutic MP were censored.
K, Graham TC, Thomas ED: Cyclosporin A and methotrexate in
The probability of relapse of the underlying disease is
canine marrow transplantation: Engraftment, graft-versus-host dis-
influenced not only by disease stage, but also by other fac-
ease, and induction of tolerance. Transplantation 34:30, 1982
tors, including the type and intensity of the GVHD prophy-
5. Storb R, Deeg HJ, Whitehead J, Appelbaum F, Beatty P, Ben-
lactic regimen and the development of acute or chronic
singer W, Buckner CD, Clift R, Doney K, Farewell V, Hansen J,
GVHD.34-36 There was a suggestion in the present analysis
Hill R, Lum L, Martin P, McGuffin R, Sanders J, Stewart P, Sullivan
K, Witherspoon R, Yee G, Thomas ED: Methotrexate and
19. Przepiorka D, Weisdorf D, Martin P, Klingemann HG, Beatty
cyclosporine compared with cyclosporine alone for prophylaxis of
P, Hows J, Thomas ED: 1994 Consensus conference on acute GVHD
acute graft versus host disease after marrow transplantation for leu-
grading. Bone Marrow Transplant 15:825, 1995
20. Sullivan KM, Shulman HM, Storb R, Weiden PL, With-
6. Ringden O, Klaesson S, Sundberg B, Ljungman P, Lonnqvist
erspoon RP, McDonald GB, Schubert MM, Atkinson K, Thomas
B, Persson U: Decreased incidence of graft-versus-host disease and
ED: Chronic graft-versus-host disease in 52 patients: Adverse natural
improved survival with methotrexate combined with cyclosporin
course and successful treatment with combination immunosuppres-
compared with monotherapy in recipients of bone marrow from
donors other than HLA identical siblings. Bone Marrow Transplant
21. Loughran TP Jr, Sullivan K, Morton T, Beckham C, Schubert
M, Witherspoon R, Sale G, Sanders J, Fisher L, Shulman H, Thomas
7. Butturini A, Bortin MM, Gale RP: Graft-versus-leukemia fol-
ED, Storb R: Value of day 100 screening studies for predicting the
lowing bone marrow transplantation. Bone Marrow Transplant
development of chronic graft-versus-host disease after allogeneic
bone marrow transplantation. Blood 76:228, 1990
8. Forman SJ, Blume KG, Krance RA, Miner PJ, Metter GE, Hill
22. Bowden RA, Cays M, Gooley T, Mamelok R, van Burik J:
LR, O’Donnell MR, Nademanee AP, Snyder DS: A prospective
Phase I study of amphotericin B colloidal dispersion (ABCD) for
randomized study of acute graft-v-host disease in 107 patients with
the treatment of invasive fungal infections after marrow transplant.
leukemia: Methotrexate/prednisone v cyclosporine A/prednisone.
23. Pepe MS, Anderson GL: Two-stage experimental designs:
9. Santos GW, Tutschka PJ, Brookmeyer R, Saral R, Beschorner
Early stopping with a negative result. Appl Stat 41:181, 1992
WE, Bias WB, Braine HG, Burns WH, Farmer ER, Hess AD, Kaizer
24. Andersen PK, Gill RD: Cox’s regression model for counting
H, Mellits D, Sensenbrenner LL, Stuart R, Yeager AM: Cyclosporine
processes: A large sample study. Ann Stat 10:1100, 1982
plus methylprednisolone versus cyclophosphamide plus methylpred-
25. Pepe MS, Longton G, Pettinger M, Mori M, Fisher LD, Storb
nisolone as prophylaxis for graft-versus-host disease: A randomized
R: Summarizing data on survival, relapse, and chronic graft-versus-
double-blind study in patients undergoing allogeneic marrow trans-
host disease after bone marrow transplantation: Motivation for and
description of new methods. Br J Haematol 83:602, 1993
10. Sayer HG, Longton G, Bowden R, Pepe M, Storb R: Increased
26. Pepe MS, Mori M: Kaplan-Meier, marginal or conditional
risk of infection in marrow transplant patients receiving methylpred-
probability curves in summarizing competing risks failure time data?
nisolone for graft-versus-host disease prevention. Blood 84:1328,
27. Hings IM, Filipovich AH, Miller WJ, Blazar BL, McGlave
11. Verfaillie C, Weisdorf D, Haake R, Hostetter M, Ramsay
PB, Ramsay NK, Kersey JH, Weisdorf DJ: Prednisone therapy for
NKC, McGlave P: Candida infections in bone marrow transplant
acute graft-versus-host disease: Short-versus long-term treatment. A
recipients. Bone Marrow Transplant 8:177, 1991
prospective randomized trial. Transplantation 56:577, 1993
12. Storb R, Pepe M, Anasetti C, Appelbaum FR, Beatty P, Doney
28. Bacigalupo A, Van Lint MT, Frassoni F, Podesta M, Venezi-
K, Martin P, Stewart P, Sullivan KM, Witherspoon R, Bensinger
ano G, Avanzi G, Vitale V, Marmont AM: High dose bolus methyl-
W, Buckner CD, Clift R, Hansen J, Longton G, Loughran T, Petersen
prednisolone for the treatment of acute graft versus host disease.
FB, Singer J, Sanders J, Thomas ED: What role for prednisone in
prevention of acute graft-versus-host disease in patients undergoing
29. Sullivan KM, Witherspoon RP, Storb R, Deeg HJ, Dahlberg
S, Sanders JE, Appelbaum FR, Doney KC, Weiden P, Anasetti C,
13. Ringde´n O, Persson U, Gunnar S, Johansson O, Gahrton G,
Loughran TP, Hill R, Shields A, Yee G, Shulman H, Nims J, Strom
Groth C-G, Lundgren G, Lo¨nnqvist B: Early diagnosis and treatment
S, Thomas ED: Alternating-day cyclosporine and prednisone for
of acute human graft-versus-host disease. Transplant Proc 15:1490,
treatment of high-risk chronic graft-versus-host disease. Blood
14. Nash RA, Pepe MS, Storb R, Longton G, Pettinger M, Ana-
30. Kennedy MS, Deeg HJ, Storb R, Doney K, Sullivan KM,
setti C, Appelbaum FR, Bowden RA, Deeg HJ, Doney K, Martin
Witherspoon RP, Appelbaum FR, Stewart P, Sanders J, Buckner
PJ, Sullivan KM, Sanders J, Witherspoon RP: Acute graft-versus-
CD, Martin P, Weiden P, Thomas ED: Treatment of acute graft-
host disease: Analysis of risk factors after allogeneic marrow trans-
versus-host disease after allogeneic marrow transplantation: Ran-
plantation and prophylaxis with cyclosporine and methotrexate.
domized study comparing corticosteroids and cyclosporine. Am J
15. Tutschka PJ, Copelan EA, Klein JP: Bone marrow trans-
31. Ramsay NKC, Kersey JH, Robison LL, McGlave PB, Woods
plantation for leukemia following a new busulfan and cyclophospha-
WG, Krivit W, Kim TH, Goldman AI, Nesbit ME Jr: A randomized
study of the prevention of acute graft-versus-host disease. N Engl J
16. Deeg HJ, Cottler-Fox M: Clinical spectrum and pathophysiol-
ogy of acute graft-vs.-host disease, in Burakoff SJ, Deeg HJ, Ferrara
32. Yau JC, LeMaistre CF, Zagars GK, Williams LA, Meneghetti
J, Atkinson K (eds): Graft-vs.-Host Disease: Immunology, Patho-
CM, Luke DR, Dunphy FR, Spinolo JA, Jagannath S, Spitzer G,
physiology, and Treatment. New York, NY, Marcel Dekker, 1990,
Zander AR, Dicke KA: Methylprednisone, cyclosporine and metho-
trexate for prophylaxis of acute graft-versus-host disease. Bone Mar-
17. Thomas ED, Storb R, Clift RA, Fefer A, Johnson FL, Neiman
PE, Lerner KG, Glucksberg H, Buckner CD: Bone-marrow trans-
33. Chao NJ, Schmidt GM, Niland JC, Amylon MD, Dagis AC,
Long GD, Nadamanee AP, Negrin RS, O’Donnell MR, Parker PM,
18. Martin PJ, Schoch G, Fisher L, Byers V, Anasetti C, Appel-
Smith EP, Snyder DS, Stein AS, Wong RM, Blume KG, Forman
baum FR, Beatty PG, Doney K, McDonald GB, Sanders JE, Sullivan
SJ: Cyclosporine, methotrexate, and prednisone compared with
KM, Storb R, Thomas ED, Witherspoon RP, Lomen P, Hannigan
cyclosporine and prednisone for prophylaxis of acute graft-versus-
J, Hansen JA: A retrospective analysis of therapy for acute graft-
host disease. N Engl J Med 329:1225, 1993
versus-host disease: Initial treatment. Blood 76:1464, 1990
34. Weiden PL, Sullivan KM, Flournoy N, Storb R, Thomas ED,
and the Seattle Marrow Transplant Team: Antileukemic effect of
J, Kolb H, Rimm AA, Ringden O, Rozman C, Speck B, Truitt RL,
chronic graft-versus-host disease. Contribution to improved survival
Zwaan FE, Bortin MM: Graft-versus-leukemia reactions after bone
after allogeneic marrow transplantation. N Engl J Med 304:1529, 1981
marrow transplantation. Blood 75:555, 1990
35. Sullivan KM, Storb R, Buckner CD, Fefer A, Fisher L,
38. Sprent J, Kosaka H, Gao EK: T cell tolerance after bone
Weiden PL, Witherspoon RP, Appelbaum FR, Banaji M, Hansen J,
marrow transplantation in mice. Bone Marrow Transplant 10:5, 1992
Martin P, Sanders JE, Singer J, Thomas ED: Graft-versus-host dis-
ease as adoptive immunotherapy in patients with advanced hemato-
39. Ochs LA, Miller WJ, Filipovich AH, Haake RJ, McGlave
logic neoplasms. N Engl J Med 320:828, 1989
PB, Blazar BR, Ramsay NK, Kersey JH, Weisdorf DJ: Predictive
36. Weisdorf DJ, Woods WG, Nesbit ME Jr, Uckun F, Dusenbery
factors for chronic graft-versus-host disease after histocompatible
K, Kim T, Haake R, Thomas W, Kersey JH, Ramsay NK: Allogeneic
sibling donor bone marrow transplantation. Bone Marrow Transplant
bone marrow transplantation for acute lymphoblastic leukaemia:
Risk factors and clinical outcome. Br J Haematol 86:62, 1994
40. Vogelsang GB: Acute and chronic graft-versus-host disease.
37. Horowitz MM, Gale RP, Sondel PM, Goldman JM, Kersey
Solide Hirnmetastasen Was gibt es Neues? Die Kombination aus Ganzhirnbestrahlung und Radiochirurgie verlängert gegenüber alleiniger Radiochirurgie nicht die Überlebenszeit, reduziert aber die lokale Rezidivrate im Gehirn (Aoyama et al. 2006). Die wichtigsten Empfehlungen auf einen Blick • Singuläre oder solitäre Hirnmetastasen solider Tumoren (mit Ausnahme kleinzel iger Bron
FICOSA participa en el desarrollo de un nuevo sistema de videovigilancia alimentado con energías renovables La tecnología del sistema de alimentación con energía eólica y solar permite el funcionamiento de instalaciones aisladas de la red eléctrica Viladecavalls (Barcelona), 13 de Noviembre de 2012.- La multinacional FICOSA ha participado en el desarrollo de un nuevo sistema de
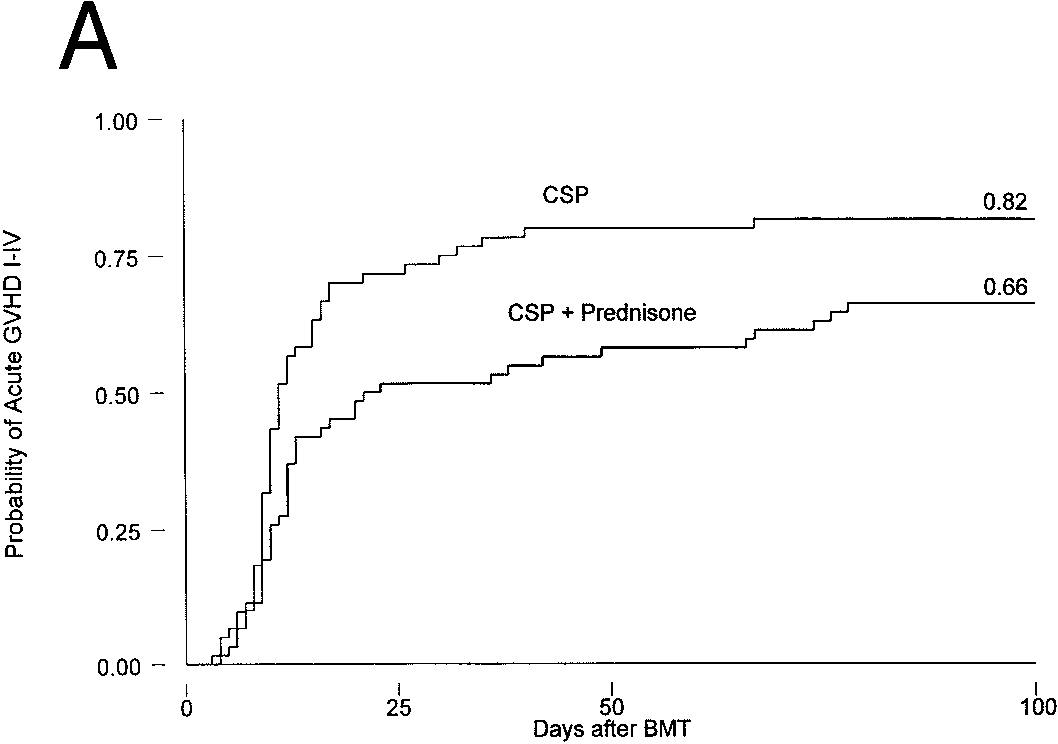
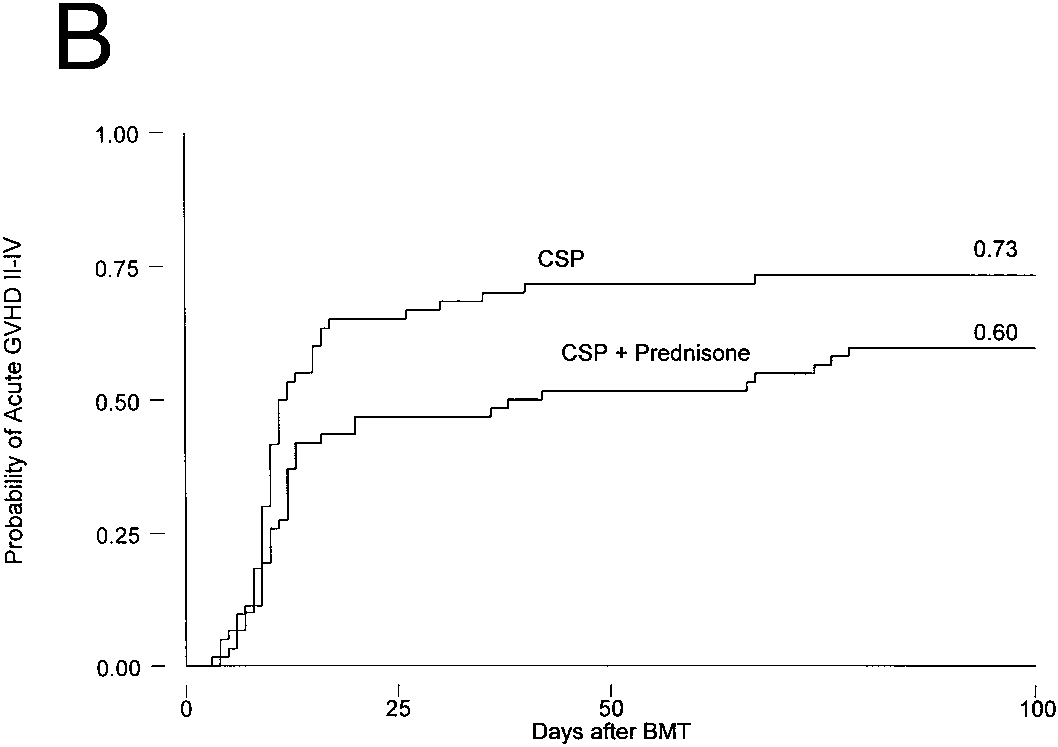 Table 3. Cox Regression Analysis of Time to Event Data
Table 3. Cox Regression Analysis of Time to Event Data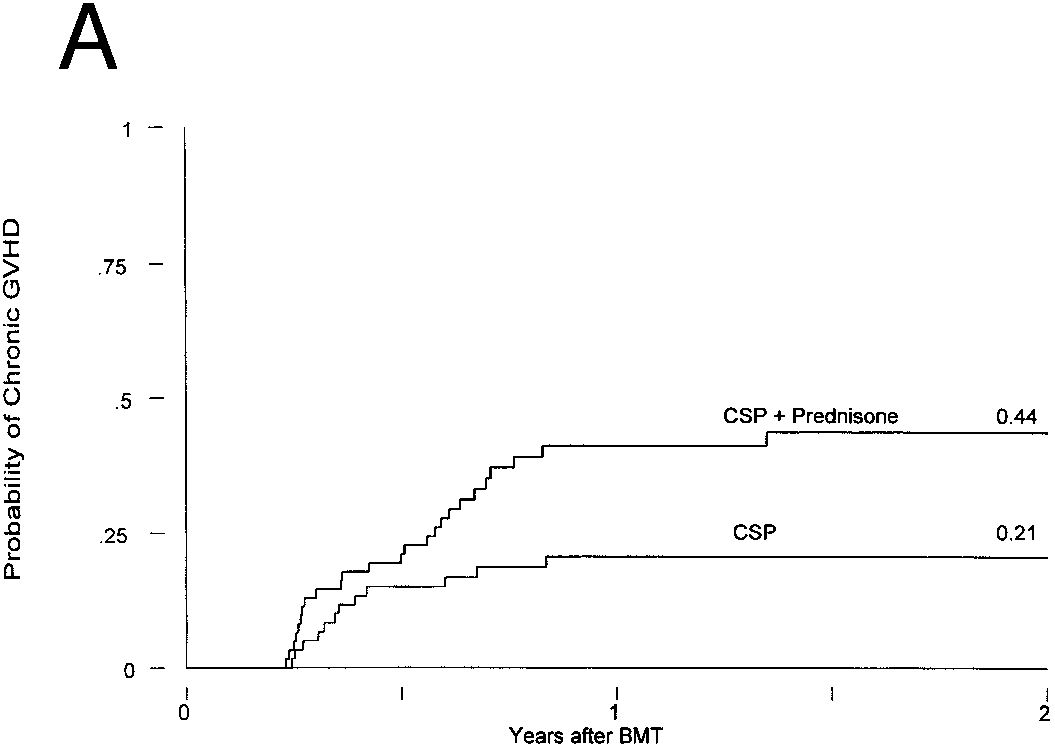
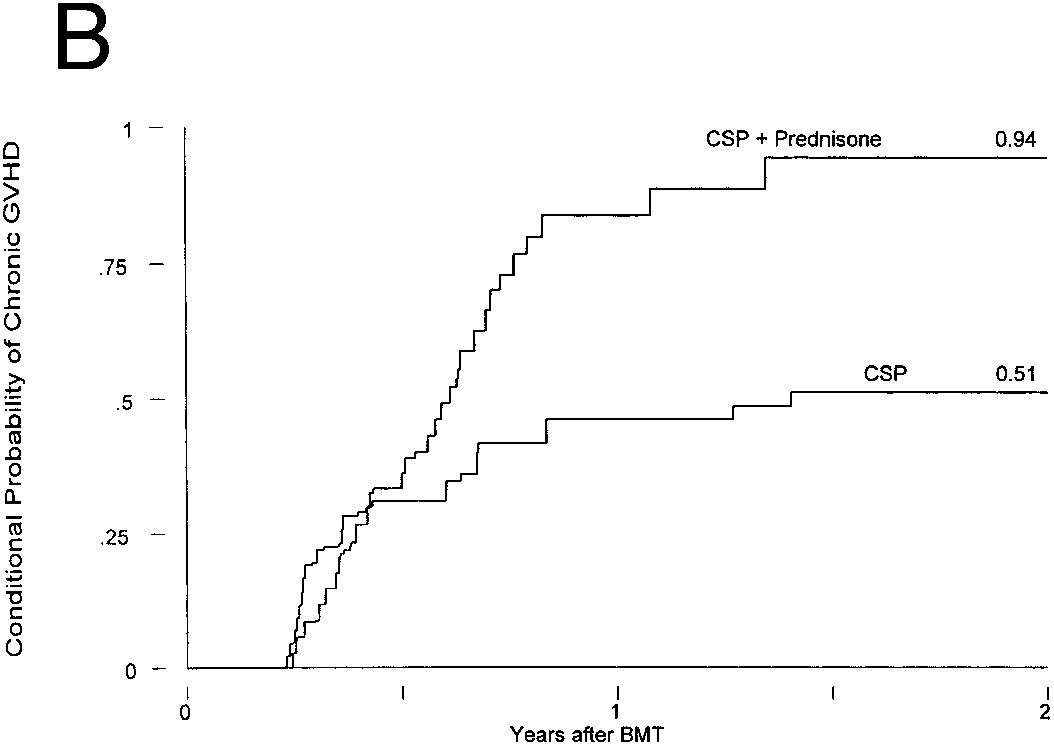
 Chronic GVHD in patients receiving GVHD prophylaxis with CSP alone or CSP plus MP. (A) Probability (P ! .02); (B) conditional
Chronic GVHD in patients receiving GVHD prophylaxis with CSP alone or CSP plus MP. (A) Probability (P ! .02); (B) conditional