Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Dx.stanford.edu
Stanford Hospital & Clinics Antibiotic Dosing Reference Guide 2011
This document is also located on the SHC Intranet (http://portal.stanfordmed.org/depts/pharmacy) P&T Approved April 15, 2011
Formulas for dosing weights: Ideal body weight IBW (male) = 50 kg + (2.3 x height in inches > 60 inches)· IBW (female) = 45 kg + (2.3 x height inches > 60 inches)
Adjusted BW (kg) = IBW + 0.4 (TBW – IBW)
Intermittent CrCl >50 mL/min CrCl 10–50 mL/min CrCl <10 mL/min Hemodialysis (IHD) Acyclovir (IV)1,4,5, 6,7,8 (Use ideal BW for Acyclovir (PO)1,5 Ambisome1(Ampho BLiposomal) Amikacin1,2,3, 7 (Use ideal or adjusted BW for obese) Timing of levels: Draw trough 30 min prior to 4th dose. Draw peak 30 min after infusion ends See appendix for Once daily dosing: goal peak 35–60; goal trough <4. Consult Hartford Nomogram complete guidelines Conventional dosing: goal peak 25–35 for serious infections, 15–20 for UTI Ampicillin (IV)1,3,4,6 Ampicillin/sulbactam1,2,4 (SHC Restriction) Azithromycin (IV/PO)1 Aztreonam1,2, 6 Severe: pseudomonas, Caspofungin1
Consider 70 mg x 1, then 35mg q24h if severe hepatic dysfunction (Child–Pugh score >7);
(Hepatic adjustment)
70 mg q24h if on phenytoin, rifampin, other strong enzyme inducers
Cefazolin1,2, 5, 6,7, 8 Cefepime1,4, 5, 6, 7 (SHC Interchange) Severe: endocarditis/CF Ceftriaxone1, 5, 9
Meningitis, E. faecalis endocarditis: 2 gm q12h
Ciprofloxacin(IV/PO)1,2, 5, Clindamycin1,2(caution in Colistin1,5,6 (Use ideal BW in obese) Daptomycin1, 10, 11, 21(Use adjusted BW in obese) (SHC Restriction) Doxycycline (IV/PO)1 Ertapenem1 Ethambutol (PO)1,7 Fluconazole(IV/PO)1,5,6, 8
Load 800 mg for Foscarnet1 Please see Lexi-comp or Micromedex for renal dosing table. Note that dosing is by CrCl per kg (ml/min/kg)
CrCl/kg > 1.4: CMV Induction treatment: 60 mg/kg q8h or 90 mg/kg q12h x 14-21 days Ganciclovir1, 6 5mg/kg for all patients
*Manufacturer’s CrCl cutoffs. Please refer to BMT protocols if applicable Gentamicin6 (SHC interchange to Gram positive tobramycin. Exception: gram positive synergy) Timing of levels: Draw trough 30 min prior to 4th dose. Draw peak 30 min after infusion ends (4th dose). (For CrCl <60, check levels sooner than 4th dose)
In HD, check trough before each HD session, and peak 30 minutes after each dose.
See appendix for Goal levels:
For synergy,goal peak 3–5mg/L (3-4 if using IDSA endocarditis guidelines). Goal trough <1 mg/L
complete guidelines
* Streptococci, Streptococcus bovis, Strep. viridans endocarditis: optional dosing 3mg/kg q24h for CrCl > 60
Imipenem/Cilastatin1,2, 6 (Nonformulary) Isoniazid1 Intermittent CrCl >50 mL/min CrCl 10–50 mL/min CrCl <10 mL/min Hemodialysis (IHD) Levofloxacin(IV/PO)1,2, 5, Linezolid(IV/PO)1,4 (SHC Restriction) Meropenem1,2, 6, 8, 18 (SHC Restriction) Consider extended infusion (3 hours) or more frequent dosing intervals for pseudomonas or resistant pathogens Moxifloxacin1 Metronidazole(IV/PO)1 Nafcillin1 Oseltamivir (PO)1,2, 15,16,17
Give after every other HD Penicillin G (IV)1, 5, 6 Piperacillin/tazobactam 1,2,4, 5, 6, 8
Extended infusion for CrCl > 20: 3.375
Posaconazole (PO)1,2, 22
No change. Posaconazole levels shown to have great degree of interpatient variability. Many clinicians would recommend
(SHC Restriction)
blood levels to assess efficacy. Consider drawing a trough 4 - 7 days after initiating dose
Pyrazinamide (PO)1, 5, 12 (Use ideal BW) Rifampin(IV/PO)1, 13, 14 Tobramycin20 (Use ideal or adjusted BW for obese) Goal levels: Goal peak (4–8mg/L), and trough (<1-2mg/L) for treatment. *certain qualifications for once–daily dosing See appendix for Timing of levels:
Draw trough 30 min prior to 4th dose. Draw peak 30 minutes after infusion ends (4th dose). (For CrCL <20, may check levels sooner than 4th dose)
complete guidelines
For once-daily dosing, draw a single random level 8 to 12 hours after dose given adjustments are made based on a published Hartford nomogram. For HD, draw trough pre-HD, and peak 30 min after end of each infusion Trimethoprim (TMP)/ Sulfamethoxazole1, 5, 6(Dose by ideal or
2.5 – 5 mg/kg/day TMP divided q8 – 12h
adjusted BW in obese)
PCP/Stenotrophomonas: 7.5 – 10 mg/kg/day TMP divided
Valganciclovir(PO)1 Please refer to transplant protocols if applicable Vancomycin6, 19, 21 (Use actual body Goal levels: Goal trough 10–15 mcg/ml (cellulitis, skin/soft tissue infections) Consider loading dose Goal trough 15–20 mcg/ml (pneumonia, bacteremia, endocarditis, osteomyelitis) of 20–25mg/kg (max Timing of levels: Draw trough< 30 minutes before 4th dose of new regimen. When SCr acutely 2gm) for severe
rises, hold dose, restart when level <15 - 20
See appendix for complete guidelines
Caution with IV: accumulation of IV vehicle cyclodextran occurs. Consider PO unless benefits justify risks of IV use.
Voriconazole (IV/PO)1,22
Levels shown to have great degree of interpatient variability. Many clinicians would recommend blood levels to assess
(SHC Restriction)
efficacy. Consider drawing a trough 4 - 7 days after new dose
Abbreviations: SCr = serum creatinine LD = loading dose; MU= million units; PNA = pneumonia; HD = hemodialysis; CAP = community acquired pneumonia; CRRT = continuous renal replacement therapy; TMP = trimethoprim; PCP: pneumocystis jiroveci pneumonia TB = tuberculosis; UF = ultrafiltration CRRT dosing: doses listed are for CVVHDFand CVVHD modalities, which are the most common modes at SHC. Note that these are generally higher than doses used in CVVH. All SHC formulary Restrictions/Interchange program descriptions can be accessed using Lexi-Comp and the intranet under pharmacy policies (intranet > Departments > Pharmacy) References: 1.
Lexi–Drug, Lexi–Comp® [Internet database]. Hudson, OH: Lexi–Comp, Inc. Available at http://www.crlonline.com. Accessed March, 2011
The Sanford Guide to Antimicrobial Therapy, 39th ed. Sperryville, VA: Antimicrobial Therapy. 2009
Drug Prescribing in Renal Failure, 5th ed. Philadelphia, PA: Dosing Guidelines for Adults and Children, 2007
McEvoy G (Ed). American Hospital Formulary Service Drug Information. Bethesda, MD: American Society of Health–System Pharmacists; 2008
Micromedex® Healthcare Series [Internet database]. Greenwood Village, CO: Thomson Reuters (Healthcare), Inc. Available at http://www.thomsonhc.com/hcs/librarian. Accessed March, 2011
Heinz et al., Antimicrobial Dosing Concepts and Recommendations forCritically Ill Adult Patients Receiving Continuous Renal Replacement Therapy or Intermittent Hemodialysis, Pharmacotherapy 2009
Aranoff GR et al., Drug Prescribing in Renal Failure, 5th edition, American College of Physicians, Philadephia, 2007
Trotman RL et al, Antibiotic Dosing in Critically Ill Adult Patients Receiving Continuous Renal Replacement Therapy, CID 2005
Guglielmo BJ et al., Ceftriaxone Therapy for Staphylococcal Osteomyelitis, CID 2000
Pai MP et al, Influence of Morbid Obesity on the Single–Dose Pharmacokinetics of Daptomycin,AAC 2007
Dvorchik BH and Damphousse,D,The Pharmacokinetics of Daptomycin in Moderately Obese, Morbidly Obese, and Matched Nonobese Subjects, Journal of Clinical Pharmacology, 2005
ATS Guidelines for Treatment of Tuberculosis, Am J RespirCrit Care Med Vol 167. pp 603–662, 2003
Baddour et al , Infective Endocarditis: Diagnosis and Management, Circulation. 2005
Zimmerli W et al., Role of Rifampin for Treatment of Orthopedic Implant–Related Staphylococcal Infections, JAMA 1998
15. http://www.cdc.gov/H1N1flu/recommendations.htm
Robson R, et al. The pharmacokinetics and tolerability of oseltamivir suspension in patients on hemodialysis and continuous ambulatory peritoneal dialysis Nephrol Dial Transplant 2006;21:2556–62.
Taylor RJ et al. Oseltamivir is adequately absorbed following nasogastric administration to adult patients with severe H5N1 influenza. PLoS ONE 2008;3:e3410.
Kuti et al., Use of Monte Carlo Simulation to Design an Optimized Pharmacodynamic Dosing Strategy for Meropenem, J ClinPharmacol2003 43: 1116
Rybak M, Lomaestro B, Rotschafer JC et al. Therapeutic monitoring of vancomycin in adult patients: A consensus review of the American Society of Health–System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Am J Health–Syst Pharm. 2009; 66:82–98
Nicolau DP et al, Experience with a Once–Daily Aminoglycoside Program Administered to 2,184 Adult Patients, AAC 1995; 39(3): 650–65
Liu et al, Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of Methicillin–Resistant Staphylococcus Aureus Infections in Adults and Children, Clinical Infectious Diseases 2011;1–38
Andes D, Pascual A, and Marchetti O. Antifungal therapeutic drug monitoring: established and emerging indications. Antimicrob Agents Chemother 2009; 53:24-34
Stanford Hospital & Clinics Vancomycin Dosing Guidelines
Vancomycin is a tricyclic Glycopeptide antibiotic that exhibits bactericidal activity by preventing the synthesis and assembly of a growing bacterial cell wall, altering the permeability of the bacterial cytoplasmic membrane, and selectively inhibiting bacterial RNA synthesis. Vancomycin is considered to be a concentration-independent or time-dependent killer of bacteria. A. Determine creatinine clearance and dose
a) Determine the dose with total body weight (TBW) b) Calculate creatinine clearance with the Cockcroft-Gault equation using an ideal body weight (IBW) or an adjusted body
weight (ABW) if the patient is obese (TBW >20% over IBW)
CrCL (mL/min) = (140 – age) x IBW ( x 0.85 for females )
IBW (male) = 50 kg + (2.3 x height in inches > 60 inches) IBW (female) = 45 kg + (2.3 x height inches > 60 inches) ABW (kg) = IBW + 0.4 (TBW – IBW)
B. Initial Empiric Dosing
Loading Dose: Consider a loading dose of 20-25mg/kg (max 2gm) for severe infections and ICU patients Creatinine Clearance Interval (mL/min) Total body weight (TBW) Hemodialysis
Post-dialysis when levels <15mg/L or <20 mg/L
in severe infections (i.e. meningitis, pneumonia)
C. Administration Vancomycin Dose Infusion Rate
Red man syndrome may occur if the infusion is too rapid. It is not an allergic reaction, but may be characterized by hypotension and/or a maculopapular rash appearing on the face, neck, trunk, and/or upper extremities. If this should occur, slow the infusion rate to over 11/2 to 2 hours and increase the dilution volume. Reactions are often treated with antihistamines
D. Therapeutic Drug Monitoring 1. Clinical situations to obtain serum trough concentrations
Patients with rapidly changing renal function
Concomitant administration of nephrotoxic medication (i.e. aminoglycosides, amphotericin B)
Patients on intermittent or continuous dialysis
Patients requiring higher than usual doses of vancomycin (>20 mg/kg/dose)
Altered volume of distribution (i.e. Morbidly obese patients)
Patients receiving prolonged course of therapy
Trough levels should be obtained within 30 minutes before the 4th dose of a new regimen
For q24h and q48h regimens, consider drawing levels prior to 3rd or 2nd dose respectively
Recommend trough levels >10 mcg/mL to avoid microbial resistance
When SCr acutely rises, hold dose and draw level. Restart therapy when level <15 - 20
CRRT: obtain level within 30 minutes prior to 3rd or 4th dose
Intermittent hemodialysis (IHD): obtain levels daily before dialysis or consider waiting >4 hours after dialysis to avoid rebound effect
Dosing assumes that HD is high flux and removes ~20% of vancomycin per 3 hour session
10–15 mcg/ml (cellulitis, skin/soft tissue infections)
15–20 mcg/ml (pneumonia, bacteremia, endocarditis, osteomyelitis)
Stanford Hospital & Clinics Aminoglycoside Dosing Guidelines
Aminoglycosides are concentration dependent antibiotics, meaning that as aminoglycoside concentration increases, the rate and extent of bacterial killing increases. Optimum bactericidal activity for the aminoglycosides is achieved when the exposure concentration is approximately 8 to 10 times the MIC. Determining dose and creatinine clearance a) Use of ideal body weight (IBW) for determining the mg/kg/dose appears to be more accurate than dosing on the basis of total
body weight (TBW). In morbid obesity, dosage requirement may best be estimated using an adjusted body weight (ABW) of: IBW + 0.4 (TBW - IBW)
Obese patients: Obese is defined as a Total body weight (TBW) > 20% over Ideal body weight (IBW)
IBW (male) = 50 kg + (2.3 x height in inches > 60 inches) IBW (female) = 45 kg + (2.3 x height inches > 60 inches)
b) Calculate creatinine clearance with the Cockcroft-Gault equation using an ideal body weight (IBW) or an adjusted body weight
CrCL (mL/min) = (140 – age) x IBW ( x 0.85 for females )
Extended-Interval Therapy (Once daily dosing)
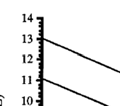
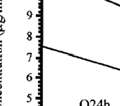
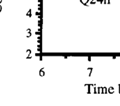
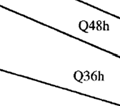
Hartford Nomogram The method of once-daily dosing intends to optimize the peak/MIC ratio in the majority of clinical situations by administering a dose of 7mg/kg of either gentamicin or tobramycin. Similar to that of conventional regimens, once-daily protocols also require modification for patients with renal dysfunction in order to minimize drug accumulation. Due to high peak concentrations obtained and the drug-free period at the end of the dosing interval, it is usually not necessary to draw standard peak and trough samples, rather a single random blood sample is obtained between 6 to 14 hours after the start of the aminoglycoside infusion. This concentration is used to determine the dosing interval based on a nomogram for once-daily dosing. Non-Hartford Nomogram The second method of extended-interval therapy utilizes a 5mg/kg gentamicin or tobramycin dose in patients without renal dysfunction. If dosage adjustment is required to compensate for impaired renal function, the dose and/or dosing interval may be modified to optimize therapy and minimize drug accumulation. Exclusion Criteria for Extended Interval Therapy:
Renal insufficiency (CrCL <30 mL/min or rapidly declining renal function)
Traditional Dosing Tradition dosing includes reduced doses and frequent administration of aminoglycosides using pharmacokinetic parameters to determine dose and frequency to achieve target peak and trough values. Gram positive-synergy Dosing Synergy dosing is a low dose of aminoglycoside in conjunction with an antimicrobial agent that exhibits activity against the cell wall of gram-positive bacteria (i.e. beta-lactams, glycopeptides) for the treatment of gram-positive infections Gentamicin & Tobramycin Initial Empiric Dosing CrCL (mL/min) Once daily dosing* Traditional Synergy** Hemodialysis
*See Hartford nomogram for monitoring of once-daily dosing regimens **Alternative for synergy: 3mg/kg Q24H for Streptococci and Streptococcus bovis endocarditis
Amikacin Initial Empiric Dosing CrCL (mL/min) Once daily dosing* Traditional Hemodialysis
* See Hartford nomogram for monitoring of once-daily dosing regimens- divide level by half then plot on graph Monitoring High Dose Extended Interval (Hartford Nomogram- for once-daily dosing) A. Initial
level testing: Single level drawn 8-12 hours after the first dose
Gentamicin/tobramycin: Plot level on graph
Amikacin: Divide level in half, then plot on graph
trough level testing- for traditional and synergy dosing regimens
Trough monitoring (30-60 minutes prior to next dose) should be considered in patients demonstrating acute
changes in renal function or suspicion of extended interval failure
Maintenance trough levels should be monitored at least once weekly
Traditional Regimens
▪ Cp< 1mg/L (mild UTI and synergy) ▪ Cp< 2-3mg/L (moderate-severe UTI) ▪ Cp< 3-5mg/L (severe GNR infection)
Gram-Positive Synergy
*Peaks are drawn 30 minutes after the end of the infusion; Cp = concentration in plasma Target Levels based on Dosing Regimen
Gentamicin and Tobramycin Amikacin Interval Peak
*7mg/kg once daily dosing does not require routine monitoring of target peaks and troughs unless the patient is having flluctuations in renal function or has failed extended interval dosing. Please follow the Hartford nomoggram and check an 8-12 hour post-dose level, this can be done after the first dose **This dose is generally used for cystic fibrosis patients
*** Extended interval dosing can be Q24H, Q36H, or Q48H References: 1.
Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America. Circulation. Jun 14 2005;111(23):e394-434.
Bates RD, Nahata MC, Jones JW, et al. Pharmacokinetics and safety of tobramycin after once-daily administration in patients with cystic fibrosis. Chest. Nov 5 1997;112(5):1208-1213.
BH. H. Vancomycin Dosing & Monitoring Guidelines. UC Davis Medical Center. 2010.
Freeman CD, Nicolau DP, Belliveau PP, Nightingale CH. Once-daily dosing of aminoglycosides: review and recommendations for clinical practice. J Antimicrob Chemother. Jun 1997;39(6):677-686.
Nicolau DP, Freeman CD, Belliveau PP, Nightingale CH, Ross JW, Quintiliani R. Experience with a once-daily aminoglycoside program administered to 2,184 adult patients. Antimicrob Agents Chemother. Mar 1995;39(3):650-655.
Nightingale CH, Ambrose PG, Drusano GL, Murakawa T. Antimicrobial Pharmacodynamics in Theory and Clinical Practice. Vol Second Edition: Informa Healthcare; 2007.
Rybak MJ, Lomaestro BM, Rotschafer JC, et al. Therapeutic monitoring of vancomycin in adults summary of consensus recommendations from the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Pharmacotherapy. Nov 2009;29(11):1275-1279.
Smyth A, Tan KH, Hyman-Taylor P, et al. Once versus three-times daily regimens of tobramycin treatment for pulmonary exacerbations of cystic fibrosis--the TOPIC study: a randomised controlled trial. Lancet. Feb 12-18 2005;365(9459):573-578.
Vic P, Ategbo S, Turck D, et al. Efficacy, tolerance, and pharmacokinetics of once daily tobramycin for pseudomonas exacerbations in cystic fibrosis. Arch Dis Child. Jun 1998;78(6):536-539.
Vic P, Ategbo S, Turck D, et al. Tolerance, pharmacokinetics and efficacy of once daily amikacin for treatment of Pseudomonas aeruginosa pulmonary exacerbations in cystic fibrosis patients. Eur J Pediatr. Nov 1996;155(11):948-953.
Whitehead A, Conway SP, Etherington C, Caldwell NA, Setchfield N, Bogle S. Once-daily tobramycin in the treatment of adult patients with cystic fibrosis. Eur Respir J. Feb 2002;19(2):303-309.
SFHRenAT15 Care for and support the patient before transplant surgery Overview This standard is about preparing the patient medically, therapeutically and psychologically for the transplant operation, and combining these different aspects of preparation with sensitivity. Users of this standard will need to ensure that practice reflects up to date information and policies. SFHRenAT15
Division of Community and Family Health Services NAME OF AGREEMENT : Interagency Coordination - Title V, Title XIX AGREEING PARTIES : This agreement is between the Utah Department of Health, Division of Community and Family Health Services (DCFHS) as the designated Title V (Maternal and Child Health) agency and the Utah Department of Health, Division of Health Care Financing (DHCF) as the desig