Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Pii: s1471-0153(01)00045-9
Cue reactivity and regulation of food intake
Department of Experimental Psychology, Maastricht University, PO Box 616,
A robust finding in eating research is the so-called counterregulation in restrained eaters. This
means that while normal subjects eat less during a taste test, after they consumed a preload, restrainedeaters consume more. An explanation is that food exposure causes stronger physiological preparatoryreactivity in the restrained eaters. This reactivity is experienced as craving and leads to an increasedfood intake. To test this theory, 46 high and low restrained eaters were exposed to food or soap, whilephysiological measurements were made. Afterwards, the subjects performed a taste test, during whichfood intake was secretly measured. Unrestrained eaters showed an increase in heart rate, gastricactivity, and saliva during food exposure; however, restrained eaters did not. Gastric activitysignificantly correlated with food intake. Group or exposure type did not influence food intake. It canbe concluded that unrestrained eaters prepared for food intake, whereas the restrained eaters did not. Apossible explanation is that restrained eaters used cognitive suppression to block physiologicalresponding, thereby controlling their food intake. D 2001 Elsevier Science Ltd. All rights reserved.
Keywords: Binge eating; Restrained eating; Conditioning; Cue reactivity
A large group of people is struggling with their food intake, trying to restrict it, but often fail
to do so. Herman and Mack (1975) performed an elegant experiment, using the so-calledpreload paradigm, in which this phenomenon is shown. In that experiment, unrestrained eatersshowed normal regulation of their eating behavior; after they ate a preload (milkshake), they ateless ice cream during a subsequent taste test than when they ate no preload. Restrained eaters,
* Corresponding author. Tel.: +31-43-388-1925/1908; fax: +31-43-361-5735. E-mail address: [email protected] (C. Nederkoorn).
1471-0153/02/$ – see front matter D 2001 Elsevier Science Ltd. All rights reserved. PII: S 1 4 7 1 - 0 1 5 3 ( 0 1 ) 0 0 0 4 5 - 9
C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
however, defined as subjects who want to restrict their food intake, consumed less during a tastetest when they did not eat a preload, but they consumed more during the taste test when they dideat a preload. This illogical behavior is called counterregulation and Herman and Mack’sexperiment initiated a large body of research. Restrained eaters repeatedly showed abnormalregulation of food intake (for an overview, see Boon, 1998). How can this eating pattern ofrestrained eaters be explained? A widespread cognitive explanation stems from the boundarymodel (Herman & Polivy, 1984). In this model, biological boundaries determine when a personfeels hungry or satiated and thereby when a person starts and stops eating. Restrained eatershave another self-imposed boundary, marking their maximum desired consumption, the so-called diet boundary. As long as this boundary is not broken, the restrained eater succeeds inrestricting food intake. When this diet boundary is broken, for example, after eating the preload,restrained eaters have disinhibitory thoughts, like ‘‘I’ve already blown my diet, I might as wellcontinue to eat,’’ and start overeating. However, restrained eaters also showed abnormalregulation after exposure to the sight, smell, or thought of food, without actually eating it(Fedoroff, Polivy, & Herman, 1997; Jansen & Van den Hout, 1991). These findings cannot beexplained with the disinhibitive thoughts of the boundary model; the ‘‘preload’’ was notconsumed, and, thus, no diet rule was broken. Furthermore, no evidence of disinhibitivethoughts was found when restrained eaters were instructed to think aloud during the preloadcondition (Jansen, Merckelbach, Oosterlaan, Tuiten, & van den Hout, 1988).
An alternative explanation for the counterregulation phenomenon stems from the cue
reactivity theory. This theory states that when a person regularly has eating binges, and thesebinges are reliable preceded by certain cues (e.g., the sight, smell and taste of the food,environment, cognitions, and emotions), these cues become predictors of the start of a binge. Exposure to these cues induces conditioned physiological reactivity, which can prepare theperson for the intake of food. In normal subjects, physiological responses to food cues arewidely documented and called cephalic phase responses (Mattes, 1997; Nederkoorn,Smulders, & Jansen, 2000). Binge eaters are expected to show even larger cephalic phaseresponses because the enormous amount of food intake during a binge threatens thehomeostatic balances of the body, and anticipation is more important compared to normalfood intake. In addition, more intense unconditioned stimulus, in this case the food intake,strengthens the conditioning. The cue reactivity is experienced as craving for the food andtriggers an eating binge (Jansen, 1994, 1998; Wardle, 1990). The theory originates in theaddiction field, where increased psychophysiological reactivity and craving are found whenthe substance abuser is exposed to drug/alcohol cues (Glautier & Remington, 1995;Robbins, Ehrman, Childress, & O’Brien, 1997), and studies suggest that craving for asubstance is a classical conditioned response (Drummond, Tiffany, Glautier, & Remington,1995). At least a part of the restrained eaters shows an eating pattern of dieting andovereating, which resembles the eating pattern of subjects with eating binges. Applied to thepreload paradigm, the cue reactivity model of binge eating states that exposure to a preload,either by seeing and smelling or actually eating it, will elicit conditioned physiologicalresponses and craving in the restrained eater. This, in turn, leads to increased food intake andcounterregulation. From the model, it also follows that, when not exposed to the preload orother binge cues, the restrained eater is able to control food intake and eats less.
C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
In sum, the cue reactivity model predicts that: (1) restrained eaters show more
physiological reactivity when exposed to binge cues than unrestrained eaters. (2) Cuereactivity is experienced as craving and (3) the increased reactivity and craving during theexposure lead to increases in the food intake of the restrained eaters during the taste testafterwards. Furthermore, the cognitive theory on overeating predicts that (4) a preload (orexposure to ‘‘forbidden’’ food) elicits disinhibitive thoughts in restrained eaters, whichlead to an increased food intake during the taste test.
The present experiment was designed to test these four hypotheses. Restrained and
unrestrained women participated in an adjusted ‘‘preload’’ experiment, in which half ofthem was exposed to the sight and smell of food, without consuming it, and the other halfwas exposed to control stimuli. During the exposure, physiological reactivity wasmeasured. Before and after the exposure, the subjects rated several subjective states, likecraving for food. Afterwards, the participants performed a taste test and food intake wasmeasured. At the end, the subjects rated retrospectively the frequency of disinhibitorythoughts during the exposure period.
As part of another study, first year students of psychology and health sciences of
Maastricht University were invited to complete a set of questionnaires, among which is aDutch translation of the White Bear Suppression Inventory (WBSI; Wegner & Zanakos,1994) and the Restraint Scale (RS; Herman & Polivy, 1980). A total of 173 participantsreturned the questionnaires. Women with scores higher than 15 and lower than 10(1/2 standard deviation of the mean in earlier studies of the authors) on the RS wereinvited by telephone to participate in a smell and taste experiment. Forty-six womenparticipated. The data of two participants were excluded from the analyses, one participantbecause of use of medication (Prozac) and one participant because she saw through theexperimental manipulations and purpose of the study. All participants filled in the RSagain directly after the experiment to obtain scores directly related to the time of theexperiment. Based on the mean RS score during the experiment (11.9), 20 participantswith higher scores were classified as restrained eaters and 24 participants with lowerscores were classified as unrestrained eaters (mean scores are revealed in Table 1).
Table 1Mean and standard error of age, BMI, RS, and EDE-Q for both groups
C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
Subjective states (relaxation, hunger, anger, craving for food, anxiety, and nausea) were
scored on visual analogue scales (VAS), ranging from 0 (e.g., not at all angry) to 100(e.g., very angry).
The subjects rated the frequencies of stereotypical disinhibitory thoughts during the
taste test retrospectively, ranging from 0 (not thought this at all) to 100 (thought it all thetime). The disinhibitory thoughts were: ‘‘ My day is ruined now, I might as well continueto eat,’’ ‘‘I cannot control myself,’’ ‘‘Everything must be eaten,’’ ‘‘Stay away from thefood,’’ ‘‘I don’t have myself in hand,’’ and ‘‘I have already eaten too much now, let’s takeanother bite.’’ The scores were summed up to obtain an overall score.
A Dutch translation of the RS (Herman & Polivy, 1980) was used to measure the intention
to restrain food intake. Subjects scoring high on the RS are characterized by an eating patternalternating between dieting episodes and periodic overeating (Herman & Polivy, 1980). ADutch translation of the EDE-Q (Fairburn & Beglin, 1994) was used to measure to existenceof specific eating psychopathology. The EDE-Q informs about restraintness, as well aseating, weight, and shape concern, and contains seven items that are not included in the sumscore. One of these items asks the number of eating binges during the last 28 days. TheWBSI (Wegner & Zanakos, 1994) exists with 15 items and measures the habituationaltendency to suppress unwanted thoughts. The participants also completed a questionnairethat checked compliance with the instructions and use of medication. Furthermore, thewomen had to describe the aim of the experiment to check whether they were conscious ofthe fact that the taste test was a pretext and that actually food intake measured.
Physiological measurements were all sampled with 250 Hz. Heart rate, blood pressure,
electrogastrography, salivation, skin conductance, and skin temperature were measured. Physiological measurements were made during the baseline (4 min) and during theexposure period (8 min).
Heart rate was measured by three Ag–AgCl electrodes, two attached over the heart
region and a reference electrode was placed on the left elbow. R-waves were detected off-line with a template matching procedure, and beats per minute were calculated.
Blood pressure was transduced using a Finapress Monitor (Ohmeda); the Finapress cuff
was attached around the middle phalanx of the middle finger of the nondominant hand. The hand was placed on a box on the table, the height of which was the same as theheart region.
Electrogastrography was measured by three Ag–AgCl electrodes, one placed on the
participant’s left side approximately 6 cm from the midline and just below the lowest rib,another just above the umbilicus and a reference electrode placed on the participant’s leftelbow. The signal was off-line resampled at 25 Hz, mean and linear trends were removed, thesignal was filtered with a high pass filter (at 0.0184 Hz, À 3 dB), and windowed with a cosinebell window (10%). After the preprocessing, the 4-min epochs were Fourier-transformed andpower was calculated in the frequency band between 2.5 and 3.5 cpm. To diminish largeindividual differences in scores caused by, among others, the thickness of the fat layer on thestomach, ratio scores with the baseline (exposure/ baseline) were calculated.
C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
As a measure of salivation, swallows were recorded (Nederkoorn, Smulder, & Jansen,
1999; Nederkoorn et al., 2000; Pomerleau, Fertig, Baker, & Cooney, 1983). The accompany-ing EMG signal was recorded with three Ag– AgCl electrodes — two electrodes were attachedunder the left jaw, in the length of the anterior part of the musculus digastricus, and a referenceelectrode was placed on the left mastoid process. Before digitization, a band pass filter was setbetween 10 and 300 Hz, and the signal was rectified and integrated. The digitized epochs werelow pass filtered (at 0.4 Hz, À 3 dB) to smooth the signal. Artifacts like coughing or talkingwere removed, and by visual inspection of the data, the definition of a swallowing responsewas determined as a response of the integrated signal above a 5-mV threshold, with a minimumof 1.5 s between responses.
Skin conductance was measured with three Ag–AgCl electrodes placed on the thenar and
hypothenar eminences of the palm of the nondominant hand; the reference electrode wasplaced on the back of this hand.
Temperature was measured by a thermistor, placed on the skin in the proximity of the liver.
This was thought to be the most sensitive place for measuring changes in surface temperaturecaused by metabolic processes (Westerterp-Plantenga, Wouters, & ten Hoor, 1990).
The participants were instructed not to eat for 3 h before the experiment. After entering
the laboratory, electrodes were attached and signals were checked. The subject was toldthat physiological reactivity to several odors would be measured. In front of theparticipant, a round table was turning, and paused for a few seconds every quarter ofthe plateau. The participant was instructed to sit quietly and relaxed. First, a baselinemeasurement of 4 min was made. Then the participant rated its subjective states on theVAS scales. Thereafter, four bowls were placed on the turning table, just under the nose ofthe participant. In the food condition, the bowls contained chocolate raisins, a kind of spicenuts (typical Dutch one-bite cookies, called ‘‘pepernoten’’), cocktail nuts, and small piecesof liquorice (called ‘‘kokindjes’’), respectively. In the control condition, the bowlscontained four different kinds of small pieces of bath soap. All bowls were filled withlarge amounts of the stimuli. The participant was instructed to concentrate on the smell ofthe stimuli and to sit quiet and relaxed again. The exposure continued for 8 min, duringwhich physiological measurements were made. Then the participant rated its subjectivestates again on the VAS scales. The turning table was removed, and the bowls were placedon the desk, in front of the participant. The participant had to fill in a questionnaire aboutthe smell of the four stimuli. Once the questionnaire was filled in, the taste test began. Thewomen in both conditions received four bowls with food stimuli and a questionnaire aboutthe taste of the food items. Subjects in the experimental group tasted the food they hadsmelled; subjects in the control group also tasted the food in bowls that were exactlycomparable to the bowls of the experimental group. The participant was told that she couldeat as much as she wanted or needed to make a proper judgement over the taste. Then theparticipant was left alone. Fifteen minutes later, the experimenter came back and removed
C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
Fig. 1. Mean and standard error of heart rate (a), salivation (b), and gastric activity (c) during control and foodexposure, compared to the baseline, of restrained and unrestrained eaters.
C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
the bowls. The participant filled in the remaining questionnaires (RS, EDE-Q, andcompliance, in that order), her weight and height were measured, and she received asmall grant for participation.
Mean physiological responses were calculated. Baseline scores, BMI, and time of
measurement were included as covariates. All variables were analyzed using 2 (restrained /unrestrained) Â 2 (food/soap exposure) between-subjects analyses of variance (ANOVA).
Unrestrained and restrained eaters did not differ in age. Restrained eaters, however, had
significantly higher BMI and scored higher on the RS and the EDE-Q. Mean age, BMI,and scores on the RS and EDE-Q are revealed in Table 1.
The first hypothesis of the cue reactivity theory was that:
Hypothesis 1: Restrained eaters show more reactivity to food exposure, compared tocontrol exposure, than unrestrained eaters.
Several physiological effects were found. A significant main effect of group on heart
rate emerged. The unrestrained eaters showed a higher heart rate than restrained eaters[ F(1,43) = 15.9, P < .001]. A marginal significant effect of condition was found; overall,the subjects showed a higher heart rate during food exposure than during control exposure[ F(1,43) = 4.0, P =.052]. There was also a significant interaction effect [ F(1,43) = 4.1,P < .05]; the heart rate of the unrestrained eaters was higher during food exposure, whereasthere was no effect on the heart rate of the restrained subjects (see Fig. 1a). Gastricactivity also showed a significant interaction [ F(1,43) = 8.4, P < .01]. Restrained eaters hada larger increase in gastric power during control exposure than during food exposure,whereas unrestrained eaters showed the opposite pattern (see Fig. 1b).
The same pattern was found for swallowing, restrained eaters swallowed more often
during the control exposure than during food exposure; unrestrained eaters swallowed moreduring food exposure [ F(1,43) = 5.0, P < .05] (see Fig. 1c).
Restrained eaters had a higher skin temperature than unrestrained eaters, irrespective of
exposure type [ F(1,43) = 5.9, P < .05]. No effects were found on blood pressure (systolic,diastolic, or mean blood pressure) and skin conductance level.
The second hypothesis of the cue reactivity theory states that:
Hypothesis 2: The physiological reactivity was experienced as craving.
Both groups reported an increase in craving after food exposure compared to exposure
to the control stimuli [ F(1,43) = 12.3, P < .001]. However, there was no significantcorrelation between any physiological measurement and craving (Fig. 2).
C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
Fig. 2. Mean and standard error of the increase in reported craving after food and control exposure of restrainedand unrestrained eaters.
The third hypothesis from the cue reactivity theory states that:
Hypothesis 3: An increase in cue reactivity and craving during the exposure is relatedto an increase in food intake during the taste test.
However, the type of exposure (control or food) did not influence food intake, in
neither group. No significant difference in food intake between the groups was found. There was also no correlation between craving and food intake. Yet, there was asignificant correlation between gastric activity during exposure and food intake duringthe taste test (r =.39, P < .01). No other correlation between a physiological measurementand food intake was found. Mean kilocalories consumed during the taste test are revealedin Table 2.
The fourth hypothesis, derived from the cognitive theory, states that:
Hypothesis 4: During food exposure, restrained eaters have more disinhibitivecognitions, leading to an increased food intake during the taste test.
Retrospectively, restrained eaters indeed reported more disinhibitive cognitions than
unrestrained eaters [ F(1,43) = 10.2, P < .005]; however, the cognitions were reported asfrequently in the food, as well as in the control condition. No significant interaction effect
Table 2Mean and standard error of kilocalories consumed during the taste test, by the restrained and unrestrained eaters,after control or food exposure
C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
was found, and there were no significant correlations between the reported cognitions andcraving for food, as well as food intake.
Exploratively, the subjective ratings of emotion (anger, fear, and relaxation) before and
after the exposure were analyzed. There was a significant interaction effect on anger[ F(1,43) = 4.4, P < .05]; restrained eaters reported more anger after control exposure andless after food exposure. Unrestrained eaters reported less anger after control exposurethan after food exposure. There were no significant effects of group or exposure onratings of other subjective states (hunger and nausea). There were also no significantcorrelations between physiological measurements and subjective ratings.
The aim of the present experiment was to test if the cue reactivity model explains the
abnormal regulation of food intake, which is often found in restrained eaters. The theorystates that restrained eaters show more reactivity when exposed to food cues(Hypothesis 1), experience this reactivity as craving (Hypothesis 2), and consequentlyeat more after the exposure (Hypothesis 3). Finally, the widespread cognitive model wastested, which predicts that restrained eaters have more disinhibitive thoughts duringexposure to the preload and this leads to an increase in food intake (Hypothesis 4).
In respect to the first hypothesis, unrestrained eaters showed a relative larger increase in
food cue reactivity than restrained eaters. Secondly, both groups reported an increase incraving after food exposure, and there was no correlation between craving, on one hand, andreactivity or food intake, on the other hand. The groups also did not differ in food intake. There was, however, a significant correlation between gastric activity and food intake.
The fourth hypothesis states that restrained eaters have more disinhibitive cognitions
during food exposure, leading to counterregulation. However, the restrained eaters did reportmore disinhibitive cognitions than unrestrained eaters after food and control exposure. Thesecognitions did not lead to counterregulation and were not directly related to craving or foodintake. Thus, although the restrained eaters did, in general, have more disinhibitivecognitions, they were not influenced by food exposure and unrelated to food intake.
It was thus found that unrestrained eaters showed a larger increase in cue reactivity than
restrained eating subjects. How can we explain this unexpected finding? The increase inheart rate, gastric activity, and salivation in normal subjects was also found in an earlier studyon cue reactivity of unrestrained eaters during food exposure (Nederkoorn et al., 2000). Now,it appears that gastric activity is indeed related to food intake. Therefore, gastric activitymight be considered to reflect a preparation response for food, and interestingly, theunrestrained subjects did prepare for food intake. It was expected to find restrained eatersto show exaggerated responses. However, they showed no or decreased responses during thefood exposure, compared to the control exposure. Opposite responses have also beenreported by others. Karhunen, Lappalainen, Tammela, Turpeinen, and Uusitupa (1997)found a decrease in salivation in obese binge eaters during food exposure; Bulik, Lawson,and Carter (1996) found a decrease in salivation in bulimic patients during exposure to binge
C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
food; and Rogers, Anderson, Finch, Jas, and Gatenby (1994) found a smaller salivaryincrease in ‘‘chocoholics’’ than in controls, after exposure to chocolate. In the addiction field,it is suggested that opposite physiological reactions serve a compensatory role, therebydiminishing the effect of the drug intake (Siegel, 1989). However, normal subjects who arealso conditioned on food intake prepare for food intake by increasing heart rate, gastricactivity, and salivation, instead of a compensatory decrease (Mattes, 1997; Nederkoorn et al.,2000). It therefore seems unlikely that restrained eaters would show preparations responsesin the opposite way.
Rogers et al. (1994) suggest that the food exposure might have caused anxiety, which
could have inhibited the salivary reaction, whereas Bulik et al. (1996) found a negativerelation between salivation and depression. That exposure to forbidden food can causedefense reactions is also found by Mauler, Tuschen, and Hamm (1997), who found largerstartle responses in bulimic patients during food exposure. However, in our experiment, therestrained subjects did not report an increase in anxiety or anger during food exposure, nordid these emotions correlate with the physiological responses. Depression was notmeasured; therefore, the role of emotions cannot completely be ruled out as a determinantof physiological reactivity.
Cognitions might also have played a role of importance. Although disinhibitive
cognitions were not related to physiological reactivity or food intake, cognitive strategiesare able to influence physiological reactivity. Dawson and Reardon (1969) and Harveyand Wickens (1973) showed that inhibitory instructions (‘‘It is not smart to reactphysiologically’’) can diminish the skin conductance orienting response, whereas facili-tatory instructions (‘‘It is very smart to react physiologically’’) enhance this response. Piacentini, Schell, and Vanderweele (1993) found that restrained eaters showed smallerorienting responses during food exposure than unrestrained eaters did. It thus might besuspected that unrestrained subjects showed physiological reactivity because they, beingnormal eaters, did not suppress any thought about food intake. Restrained eaters, on theother hand, are supposed to suppress eating-related cognitions. They always try torestrain their intake; in other words, it might be hypothesized that they use cognitivestrategies to suppress or block their physiological reactivity. This suggestion would extantthe cue reactivity theory: Food cues can elicit physiological reactivity, which leads to anincreased food intake (supported by the correlation found between gastric activity andfood intake), but subjects are able to inhibit these reactions by cognitive suppression. Incase the suppression fails, the restrained eaters are expected to overeat. In the presentexperiment, the restrained eaters might have been successful in suppressing theirphysiological reactivity, and thereby in restraining their food intake. Indeed, we found,post hoc, a significant positive correlation between scores on the WBSI and the RS(r =.48, P < .001, n = 43), suggesting that restraintness in eating and cognitive suppression,in general, are closely related. However, we did not measure suppression directly, leavingthis explanation hypothetically.
Another finding in contrast to predictions of the cue reactivity model was that
physiological reactivity was not related to subjective craving, and craving was not relatedto the amount of food intake. Of course, being in a laboratory and attached to
C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
physiological apparatus can have disturbed feelings of craving and inhibited food intake. Itmight still be possible that in natural settings, a relation will be found between craving, onone hand, and physiological reactivity and food intake, on the other hand. So far, however,we must conclude that no evidence is found that subjective craving plays a role ofimportance in counterregulation.
In sum, unrestrained eaters showed physiological reactivity during food exposure, and over
all subjects, the gastric activity was related to the amount of food intake afterwards. There was,however, no relationship between subjective craving and food intake. Restrained eatersshowed opposite physiological responses, which might result from intervening emotions orthe use of cognitive strategies to suppress unwanted reactivity. Because the cognitivesuppression hypothesis is post hoc and not tested in the present experiment, it might be afruitful enterprise for further research to manipulate suppression directly during food exposureand to measure its effects on psychophysiological reactivity, as well as on food intake.
The authors acknowledge with gratitude the support of Eric Rassin with the WBSI data.
Boon, B. J. F. (1998). Why dieters overeat: on the cognitive regulation of eating behavior (pp. 11 – 43). Unpub-
lished doctoral dissertation, University of Utrecht, the Netherlands.
Bulik, C. M., Lawson, R. H., & Carter, F. A. (1996). Salivary reactivity in restrained and unrestrained eaters and
women with bulimia nervosa. Appetite, 27, 15 – 24.
Dawson, M. E., & Reardon, P. (1969). Effects of facilitatory and inhibitory sets on GSR conditioning and
extinction. Journal of Experimental Psychology, 82, 462 – 466.
Drummond, D. C., Tiffany, S. T., Glautier, S., Remington, B. (1995). Addictive behaviour: cue exposure theory
Fairburn, C. G., & Beglin, S. J. (1994). The assessment of eating disorders: interview or self-report questionnaire?
International Journal of Eating Disorders, 16, 363 – 370.
Fedoroff, I. C., Polivy, J., & Herman, C. P. (1997). The effect of pre exposure to food cues on the eating behavior
of restrained and unrestrained eaters. Appetite, 28, 33 – 47.
Glautier, S., & Remington, B. (1995). The form of responses to drug cues. In: D. C. Drummond, S. T. Tiffany,
S. Glautier, & B. Remington (Eds.), Addictive behaviour, cue exposure, theory and practice ( pp. 21 – 46). Chichester: Wiley.
Harvey, C. B., & Wickens, D. D. (1973). Effects of cognitive control processes on the classically conditioned
galvanic skin response: a within-subjects design. Journal of Experimental Psychology, 101, 278 – 282.
Herman, C. P., & Mack, D. (1975). Restrained and unrestrained eating. Journal of Personality, 43, 647 – 660. Herman, C. P., & Polivy, J. (1980). Restrained eating. In: A. B. Stunkard (Ed.), Obesity ( pp. 208 – 255). Phila-
Herman, C. P., & Polivy, J. (1984). A boundary model for the regulation of eating. In: A. J. Stunkard, & E. Stellar
(Eds.), Eating and its disorders ( pp. 141 – 156). New York: Raven Press.
Jansen, A. (1994). The learned nature of binge eating. In: C. R. Legg, & D. A. Booth (Eds.), Appetite, (8,
pp. 193 – 211). Oxford: Oxford University Press.
C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
Jansen, A. (1998). A learning model of binge eating: cue reactivity and cue exposure. Behaviour Research and
Jansen, A., Merckelbach, H., Oosterlaan, J., Tuiten, A., & van den Hout, M. A. (1988). Cognitions and self-talk
during food intake of restrained and unrestrained eaters. Behaviour Research and Therapy, 26, 393 – 398.
Jansen, A., & Van den Hout, M. (1991). On being led into temptation: ‘‘counterregulation’’ of dieters after
smelling a ‘‘preload’’. Addictive Behaviors, 16, 247 – 253.
Karhunen, L. J., Lappalainen, R. I., Tammela, L., Turpeinen, A. K., & Uusitupa, M. I. J. A. D. (1997). Subjective
and physiological cephalic phase responses to food in obese binge eating women. International Journal ofEating Disorders, 21, 321 – 328.
Mattes, R. D. (1997). Physiological responses to sensory stimulation by food: nutritional implications. Journal of
the American Dietetic Association, 97, 406 – 410.
Mauler, B., Tuschen, B., & Hamm, A. (1997). Fear or craving: startle reflex modulation during viewing of food
cues in deprived and nondeprived bulimics. Psychophysiology, 34, S1, S62.
Nederkoorn, C., Smulder, F. T. Y., & Jansen, A. (1999). Recording of swallowing events using electromyography
as a non-invasive measurement of salivation. Appetite, 33, 361 – 369.
Nederkoorn, C., Smulders, F. T. Y., & Jansen, A. (2000). Cephalic phase responses, craving and food intake in
normal subjects. Appetite, 35, 45 – 55.
Piacentini, A., Schell, A. M., & Vanderweele, D. A. (1993). Restrained and nonrestrained eaters’ orienting
responses to food and nonfood odors. Physiology & Behavior, 53, 133 – 138.
Pomerleau, O. F., Fertig, J. B., Baker, L., & Cooney, N. (1983). Reactivity to alcohol cues in alcoholics and non-
alcoholics: implications for a stimulus control analysis of drinking. Addictive Behaviors, 8 (1), 1 – 10.
Robbins, S. J., Ehrman, R. N., Childress, A. R., & O’Brien, C. P. (1997). Relationships among physiological and
self-report responses produced by cocaine-related cues. Addictive Behaviors, 22, 157 – 167.
Rogers, P., Anderson, A., Finch, G., Jas, P., & Gatenby, S. (1994, August). Relationship between food craving
and anticipatory salivation, eating patterns, mood and body weight in women and men. Poster sessionpresented at the Society for the Study of Ingestive Behaviour, Second Independent Meeting, MacMasterUniversity, Hamilton, Canada.
Siegel, S. (1989). Pharmacological conditioning and drug effects. In: A. J. Goudie, & M. W. Emmett-Oglesby
(Eds.), Psychoactive drugs: tolerance and sensitization ( pp. 115 – 180). Clifton, NJ: Humana Press.
Wardle, J. (1990). Conditioning processes and cue exposure in the modification of excessive eating. Addictive
Wegner, D. M., & Zanakos, S. (1994). Chronic thought suppression. Journal of Personality, 62, 615 – 640. Westerterp Plantenga, M. S., Wouters, L., & ten Hoor, F. (1990). Deceleration in cumulative food intake curves,
changes in body temperature and diet-induced thermogenesis. Physiology & Behavior, 48 (6), 831 – 836.
CLINICIAN’S CORNER Management of Fibromyalgia Syndrome Don L. Goldenberg, MD Context The optimal management of fibromyalgia syndrome (FMS) is unclear and comprehensive evidence-based guidelines have not been reported. Objective To provide up-to-date evidence-based guidelines for the optimal treat- ment of FMS. ATANYONETIME,10%TO12% DataSources,Selection,andExtraction Asearchofallhu
GASTROENTEROLOGY AND HEPATOLOGY Faculty Publications July 1, 2008 – June 30, 2009 PEER-REVIEWED MANUSCRIPTS Agrawal A , Roberts J, Sharma N, Tutuian R, Vela M, Castell DO . Symptoms with acid and nonacid reflux may be produced by different mechanisms. Dis Esophagus. 2009;22(5):467-70. Epub 2009 Feb 13. PubMed PMID: 19222535. Kraichely RE, Farrugia G, Pittock SJ, Cas
 Cue reactivity and regulation of food intake
Department of Experimental Psychology, Maastricht University, PO Box 616,
A robust finding in eating research is the so-called counterregulation in restrained eaters. This
means that while normal subjects eat less during a taste test, after they consumed a preload, restrainedeaters consume more. An explanation is that food exposure causes stronger physiological preparatoryreactivity in the restrained eaters. This reactivity is experienced as craving and leads to an increasedfood intake. To test this theory, 46 high and low restrained eaters were exposed to food or soap, whilephysiological measurements were made. Afterwards, the subjects performed a taste test, during whichfood intake was secretly measured. Unrestrained eaters showed an increase in heart rate, gastricactivity, and saliva during food exposure; however, restrained eaters did not. Gastric activitysignificantly correlated with food intake. Group or exposure type did not influence food intake. It canbe concluded that unrestrained eaters prepared for food intake, whereas the restrained eaters did not. Apossible explanation is that restrained eaters used cognitive suppression to block physiologicalresponding, thereby controlling their food intake. D 2001 Elsevier Science Ltd. All rights reserved.
Cue reactivity and regulation of food intake
Department of Experimental Psychology, Maastricht University, PO Box 616,
A robust finding in eating research is the so-called counterregulation in restrained eaters. This
means that while normal subjects eat less during a taste test, after they consumed a preload, restrainedeaters consume more. An explanation is that food exposure causes stronger physiological preparatoryreactivity in the restrained eaters. This reactivity is experienced as craving and leads to an increasedfood intake. To test this theory, 46 high and low restrained eaters were exposed to food or soap, whilephysiological measurements were made. Afterwards, the subjects performed a taste test, during whichfood intake was secretly measured. Unrestrained eaters showed an increase in heart rate, gastricactivity, and saliva during food exposure; however, restrained eaters did not. Gastric activitysignificantly correlated with food intake. Group or exposure type did not influence food intake. It canbe concluded that unrestrained eaters prepared for food intake, whereas the restrained eaters did not. Apossible explanation is that restrained eaters used cognitive suppression to block physiologicalresponding, thereby controlling their food intake. D 2001 Elsevier Science Ltd. All rights reserved.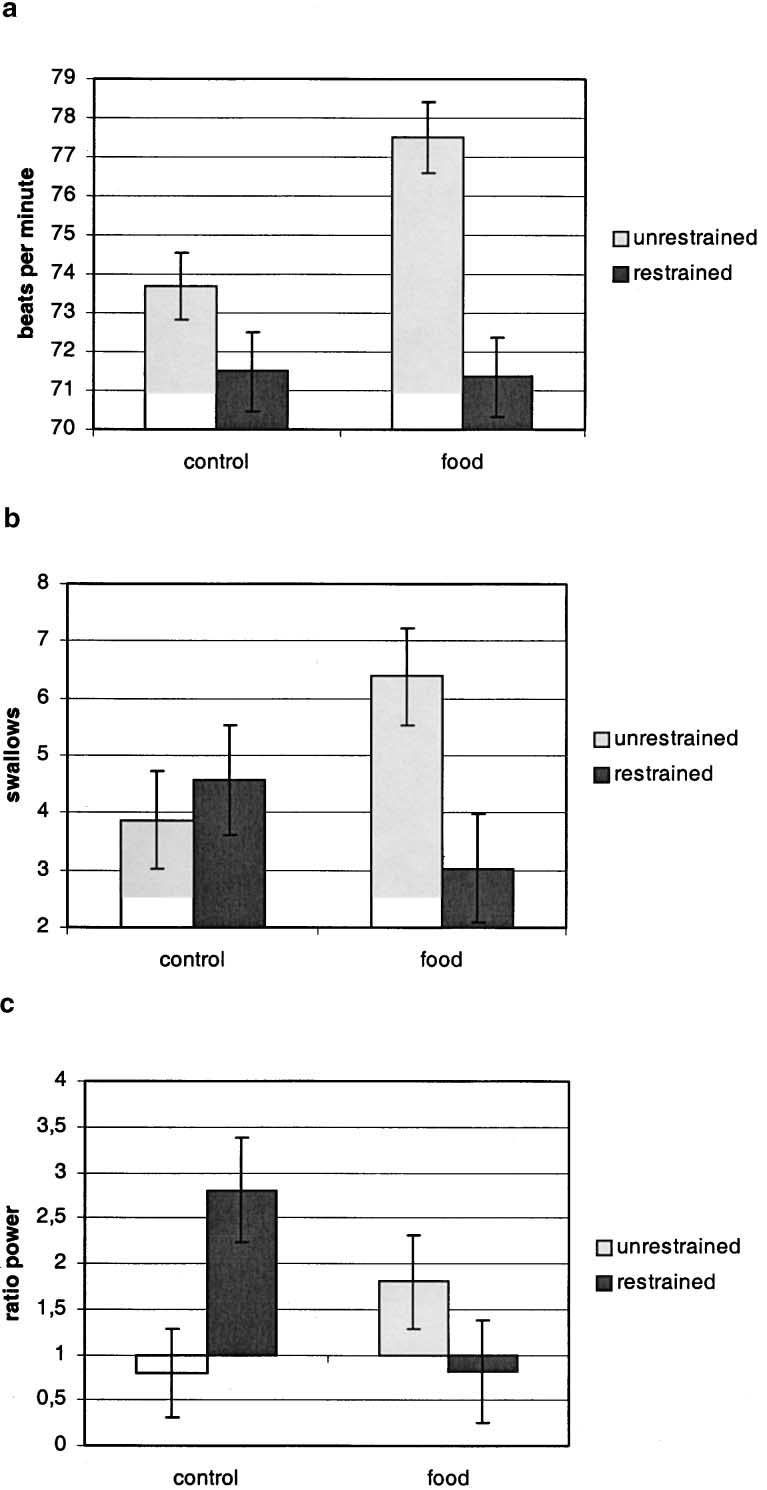 C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
Fig. 1. Mean and standard error of heart rate (a), salivation (b), and gastric activity (c) during control and foodexposure, compared to the baseline, of restrained and unrestrained eaters.
C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
Fig. 1. Mean and standard error of heart rate (a), salivation (b), and gastric activity (c) during control and foodexposure, compared to the baseline, of restrained and unrestrained eaters.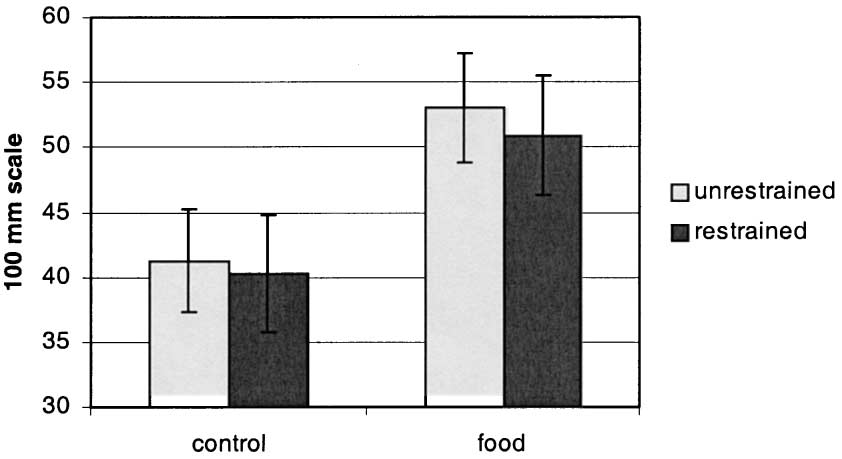 C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
Fig. 2. Mean and standard error of the increase in reported craving after food and control exposure of restrainedand unrestrained eaters.
C. Nederkoorn, A. Jansen / Eating Behaviors 3 (2002) 61–72
Fig. 2. Mean and standard error of the increase in reported craving after food and control exposure of restrainedand unrestrained eaters.