University of Michigan Guidelines for Health System Clinical Care Gastroesophageal Reflux Disease (GERD) Patient population: Adults Guideline Team Objective: To implement a cost-effective and evidence-based strategy for the diagnosis and Team Leader
treatment of gastroesophageal reflux disease (GERD).
Joel J Heidelbaugh, MD Family Medicine Key Points: Team Members
Diagnosis History. A well-taken history is essential in establishing a diagnosis of GERD. If the classic
symptoms of heartburn and acid regurgitation clearly dominate a patient’s history, they can help
establish the diagnosis of GERD with sufficiently high specificity, although sensitivity of clinical
history remains low compared to 24-hour pH monitoring. The presence of atypical symptoms
(Table 1), although common, cannot sufficiently support the clinical diagnosis of GERD. [B*]Testing. No gold standard exists for the diagnosis of GERD [A*]. Although pH probe is accepted
as the standard with a sensitivity of 85% and specificity of 95%, false positives and false negatives
still exist [B*]. Endoscopy lacks sensitivity in determining pathologic reflux. Barium radiology has
limited usefulness in the diagnosis of GERD and is not recommended [B*].
Therapeutic trial. An empiric trial of acid suppression therapy can identify patients with GERD
who do not have alarm symptoms [A*] and may be helpful in the evaluation of those with atypical
manifestations of GERD, specifically, non-cardiac chest pain (NCCP) [B*].
UMHS Guidelines
Treatment Oversight Team Lifestyle modifications. Lifestyle modifications should be recommended throughout the treatment
of GERD, but there is little evidence-based data to support their efficacy [D*].
William E Chavey, MD R Van Harrison, PhD
Pharmacologic treatment. H2-receptor antagonists (H2RAs), proton pump inhibitors (PPIs), and
prokinetics have proven efficacy in the treatment of GERD [A*]. Past prokinetics have been as
effective as H2RAs but are currently unavailable [A*]. Carafate and antacids are ineffective [A*],
but may be used as supplemental acid-neutralizing agents for certain patients with GERD [D*].
• Non-erosive reflux disease (NERD): Step-up (H2RAs followed by a PPI if no improvement) and
Literature search service
step-down (PPI followed by the lowest dose of acid suppression) therapy are equally effective for
both acute treatment and maintenance [C*]. Costs for step-down treatment are mainly
medications, while step-up treatment requires more frequent endoscopy. On demand (patient-
directed) therapy is the most cost-effective strategy.
• Documented erosive esophagitis: Initial PPI therapy is the treatment of choice for acute and
For more information call GUIDES: 734-936-9771
maintenance therapy for patients with documented erosive esophagitis [A*].
• PPI’s should be taken 30-60 minutes prior to a meal to optimize effectiveness [B*].
Surgery. Antireflux surgery is an alternative modality in the treatment of GERD in patients who
have documented chronic reflux with recalcitrant symptoms [A*]. Surgery has a significant
Regents of the
complication rate (10-20%). Resumption of pre-operative medication treatment (>50%) is common
University of Michigan Other endoscopic modalities. Some alternative endoscopic modalities are less invasive and have
fewer complications, but are also likely to have lower response rates than antireflux surgery [C*],
and have not been shown to reduce acid exposure.
Follow up Symptoms unchanged. If symptoms remain unchanged in a patient with a prior normal
endoscopy, repeating endoscopy has no benefit and is not recommended [C*].
construed as including all proper methods of care or
Warning signs. Patients with warning signs and symptoms suggesting complications from GERD
(Table 2) should be referred to a GERD specialist.
methods of care reasonably directed to obtaining the same
Risk for complications. Further diagnostic testing (e.g., EGD [esophagogastroduodenoscopy], pH
monitoring) should be considered in patients who do not respond to acid suppression therapy [C*]
regarding any specific clinical procedure or treatment must be
and in patients with a chronic history of GERD who are at risk for complications (e.g., Barrett’s
esophagus, adenocarcinoma, stricture). Chronic reflux has been suspected to play a major role in
of the circumstances presented by the patient.
the development of Barrett’s esophagus, yet it is unknown if outcomes can be improved through
surveillance and medical treatment [D*]. Costs of surveillance for Barrett’s Esophagus without
dysplasia are likely to be prohibitive [B*]. Anti-reflux therapy has been shown to reduce the need for recurrent dilation from esophageal stricture formation [A*].
* Levels of evidence reflect the best available literature in support of an intervention or test: A=randomized controlled trials; B=controlled trials, no randomization; C=observational trials; D=opinion of expert panel. Figure 1. Diagnosis and Treatment of GERD Table 1. Atypical Table 2. Warning Signs Table 3. Lifestyle Modifications [D*] Signs of GERD Suggesting Complicated GERD
Avoid recumbency for 3 hours postprandially
Avoid certain foods: chocolate, alcohol, peppermint,
coffee, onions, garlic, fatty foods, citrus, tomato
Avoid medications that can potentiate symptoms
Table 4. Medications for Acute Treatment and Maintenance Regimens Drug Dose Dosage $ Cost/Month Equivalents Brand Generic
20 mg daily/40 mg daily/40 mg BID 142/142/284
40 mg daily/80 mg daily/40 mg BID 114/228/228
30 mg daily/60 mg daily/30 mg BID 144/288/288
a For brand drugs, Average Wholesale Price minus 10%. AWP from Amerisource Bergen Wholesale Catalog 10/06. For generic drugs,
Maximum Allowable Cost plus $3 from BCBS of Michigan MAC List, 8/8/06. Clinical Background Clinical Problem Treatment Decision Problems Incidence
Although symptomatic relief generally occurs with empiric
treatment, the long-term effects of anti-reflux medications
Gastroesophageal reflux disease (GERD) is a common
are as yet unknown. Complications from GERD (e.g.,
chronic, relapsing condition that carries a risk of significant
Barrett’s esophagus, adenocarcinoma) are rare but do exist;
10-15% with GERD will develop Barrett’s esophagus, and
complications. While many patients self-diagnose, self-
5-10% of those with Barrett’s will develop adenocarcinoma
treat and do not seek medical attention for their symptoms,
over 10-20 years. Chronic reflux has been suspected to
others suffer from more severe disease with esophageal
play a major role in the development of Barrett’s esophagus
damage ranging from erosive to ulcerative esophagitis.
(specialized columnar epithelium/intestinal metaplasia), yet
it is unknown if outcomes can be improved through
More than 60 million adult Americans suffer from
surveillance and medical treatment. Anti-reflux therapy has
heartburn at least once a month and over 25 million
been shown to reduce the need for recurrent dilation from
experience heartburn daily. The National Ambulatory
Medical Care Survey (NAMCS) found that 38.53 million
annual adult outpatient visits were related to GERD. For
Previous cost-effectiveness models were flawed in that
patients presenting with GERD symptoms, 40-60% or more
certain studies examined only patients with erosive
have reflux esophagitis. Up to 10% of these patients will
esophagitis and excluded patients with non-erosive
have erosive esophagitis after investigation. GERD appears
esophagitis (NERD), while some studies included data on
to be more prevalent in pregnant women and a higher
anti-reflux surgery only for patients who failed medical
complication rate exists among the elderly. Patients with
therapy. These studies also viewed a short-term analysis of
GERD generally report decreases in productivity, quality of
therapeutic efficacy, rather than following patients over a
life and overall well-being. Many patients rate their quality
lifetime, and did not allow for the switching from one
of life to be lower than that reported by patients with
untreated angina pectoris or chronic heart failure. GERD is
a risk factor for the development of adenocarcinoma,
Rationale for Recommendations
further increasing the importance of its diagnosis and
Etiology
Extraesophageal manifestations associated with GERD
Most patients with GERD have normal baseline LES (lower
occur in up to 50% of patients with non-cardiac chest pain,
esophageal sphincter) tone. The most common mechanism
78% of patients with chronic hoarseness, and 82% of
for acid reflux is transient relaxation of the lower
patients with asthma. Over 50% of patients with GERD
esophageal sphincter (> 90% of reflux episodes in normal
have no endoscopic evidence of disease. Although
subjects and 75% of episodes in patients with symptomatic
diagnostic limitations occur less often when patients present
GERD). Other mechanisms include breaching the LES
with the classic symptoms of heartburn and acid
because of increased intra-abdominal pressure (strain
regurgitation, diagnosis may be difficult in patients with
induced reflux) and a baseline low LES pressure. The latter
recalcitrant courses and extraesophageal manifestations of
two mechanisms increase in frequency with greater reflux
severity. Other factors include delayed gastric emptying
(co-factor in 20% of GERD patients), medication use
Diagnostic Problems
(particularly calcium channel blockers), hiatal hernia
(increased strain induced reflux and poor acid clearance
The lack of a gold standard in the diagnosis of GERD
from hernia sac), and poor esophageal acid clearance
presents a clinical dilemma in treating patients with reflux
(esophageal dysmotility, scleroderma, decreased salivary
symptomatology. Many related syndromes including
atypical GERD, H. pylori-induced gastritis, gastroduodenal
ulcer and gastric cancer may present similarly, making
Natural History
accurate history taking important. Even in these cases the
pre-test sensitivity and specificity for accurate diagnosis
Most GERD patients do not seek medical attention (80-
remain low. Invasive testing is over-utilized and not always
90%) and self-medicate (50%). In patients seeing
cost-effective, given the relatively small risk of
physicians, most will have chronic symptoms that will
misdiagnosis based upon an accurate patient history.
occur off treatment. Patients with more severe esophagitis
Empiric pharmacotherapy is advantageous based on both
will have symptoms recur more quickly and almost all will
have recurrent symptoms and esophagitis if followed up for
> 1 year. Progression of disease can be seen in up to 25% of patients with esophagitis, but it is less likely to occur if
esophagitis is not present or is mild (LA class A, B).
Empiric therapy should be tried for two weeks for patients
Complications such as Barrett’s esophagus, esophageal
with typical GERD symptoms. Treatment can be initiated
ulcers, esophageal stricture or adenocarcinoma of the
with standard dosage of either an H2RA BID (on demand)
esophagus are very rare unless the initial endoscopy shows
or a PPI (30-60 minutes prior to first meal of the day), with
esophagitis or Barrett’s esophagus. A normal endoscopy
drug selection depending on clinical presentation and
with symptomatic GERD presents a good prognosis. Long
appropriate cost effectiveness and the end point of complete
term natural history studies are few and are urgently
symptom relief. (See Figure 1 and Table 4). If symptom
relief is not adequate and H2RA BID was initially used,
then PPI daily should be used. If PPI daily was initially
Diagnosis
used, then increase to maximum dose PPI daily or BID (30-
60 minutes prior to first and last meals).
Evidence-based limitations exist when trying to assess the
validity of the diagnostic modalities for GERD. Most
For those patients who initially present with more severe
studies are flawed methodologically because no gold
and more frequent symptoms of typical GERD, treatment
standard exists. However, the calculated numbers are
may be initiated with higher and more frequent dosages of
helpful in providing a framework to assess available
an H2RA or PPI. If symptom relief is not adequate from
options. Recent studies suggests that combining diagnostic
initial dose, then increase potency/frequency as needed to
modalities (omeprazole challenge test, pH monitoring, and
obtain complete symptom relief: high-dose H2RA to PPI
endoscopy) may increase the sensitivity for diagnosis of
daily, PPI daily or maximum dose PPI daily or BID. If
GERD (approaching 100%), but this approach is not
there is no response when using higher dosages, then
practical in the routine clinical setting.
diagnostic testing should be performed. If patient responds,
give 8-12 weeks of therapy, i.e. enough to heal undiagnosed
History. A well-taken history is essential in establishing
esophagitis. If patient has complete symptom relief at 8-12
the diagnosis of GERD. Symptoms of classic burning in
weeks, taper over 1 month to lowest effective dose of the
the chest, with sour or bitter taste, and acid regurgitation
medication that gives complete relief, e.g., H2RA on
have been shown to correctly identify GERD with a
demand, PPI QOD. If symptoms reoccur, put patient back
sensitivity of 89% and specificity of 94%. However,
on initial effective medication and dose, and consider
symptom frequency, duration and severity are equally
further testing depending on clinical presentation and
distributed among patients with varying grades of
esophagitis and Barrett’s esophagus and cannot be used
reliably to diagnose complications of GERD.
Patients who present with atypical or extraesophageal
manifestations take a longer time to respond to empiric
PPI diagnostic test. A response to a short course of
therapy. If there is no improvement at all in symptoms after
proton-pump inhibitors (PPIs) is commonly considered to
one month, further testing should be pursued.
support a diagnosis of GERD. PPIs have been studied and
tried more often than H2-receptor antagonists given their
Endoscopy. Endoscopy is the primary technique for
higher efficacy. A recent meta-analysis found that a
evaluating mucosal integrity, esophageal stricture
successful short-term trial of PPI therapy did not
formation, and Barrett's esophagus with a sensitivity of
confidently establish a diagnosis of GERD (sensitivity 78%,
50% and specificity of 95%. Endoscopic evidence of
specificity 54%) when 24 hour pH monitoring was used as
esophagitis occurs in less than 50% of people who have
the reference standard. This may be due to observed
experienced heartburn greater than twice a week over a six-
clinical benefit of PPIs in treating other acid-related
conditions (as seen in the heterogeneous dyspeptic
population), patients with enhanced esophageal sensitivity
Esophagitis is best defined by the LA classification system
to acid (without true GERD), or even due to a placebo
and identifies the degree to which mucosal breaks (erosions
effect. In those with NCCP (non-cardiac chest pain),
or ulcerations) occur, graded in severity from A to D, with
empiric trial with high-dose omeprazole (40 mg AM, 20 mg
D being the most severe. Specific definitions are:
PM) had a sensitivity of 78% and specificity of 85%.
A One or more mucosal breaks no longer than 5 mm,
Standard dosages may have lower sensitivity and
none of which extends between the tops of the
B One or more mucosal breaks more than 5 mm long,
Empiric/therapeutic trial. Diagnostic modalities cannot
none of which extends beyond the tops of two
reliably exclude GERD even if they are negative.
Therefore an empiric trial may be the most expeditious way
C Mucosal breaks that extend between the tops of two
in which to diagnose GERD in those with classic symptoms
or more mucosal folds, but which involves less than
and who do not have symptoms suggestive of complications
(e.g., carcinoma, stricture). (Also see the discussion of
D Mucosal breaks which involve at least 75% of the
"step-up" therapy and "step-down" therapy in treatment
(Dent, J et al. An evidence-based appraisal of reflux
symptoms with reflux events. Associations greater than
disease management-the Genval Workshop Report. Gut
The purpose for pH probe must be defined before
Although biopsy is indicated in defining Barrett's
proceeding: is it to diagnose GERD or to determine the
esophagus, histological assessment has not been clinically
adequacy of therapy. The test should be performed off
useful in the diagnosis of GERD if endoscopy is positive
therapy if the diagnosis is under question. The test should
for mucosal abnormalities. Descriptives such as erythema,
be performed on therapy if one is trying to determine the
edema, and friability also are not clear indications of
adequacy of treatment. The major indication for
performing 24 ambulatory pH monitoring is in
documenting treatment failures, either to antireflux surgery
Endoscopy should be considered in those who present with
warning symptoms (see Table 2) and who are suspected to
have complications from GERD. Further testing should
Other diagnostic modalities. Other diagnostic modalities
also occur for patients who do not respond to therapy, need
include manometry, Bernstein’s test and gastroesophageal
continuous chronic therapy and have risk factors for
scintigraphy. Due to their many limitations, these tests
should not be routinely ordered. Barium swallow should
not be used in the evaluation of GERD although it was
Repeating endoscopy is likely not to be worthwhile
commonly used in the past. It is useful in the evaluation of
following a normal result. In observational studies, patients
dysphagia but limited in its ability as a screening test for
with an initial normal endoscopy have not been found to
GERD, as are all the aforementioned modalities.
progress to severe esophagitis during a 10 year follow-up,
thus arguing against repeat endoscopy in a select group of
patients whose symptom complex has not changed during
Treatment
this time. However, some patients did progress to grade A
Lifestyle modifications. For a history typical for
uncomplicated GERD, expert opinion is to discuss and PH probe. Many patients do not have evidence of offer various lifestyle modifications throughout the course
esophagitis on endoscopy and yet they respond to acid
of GERD therapy (see Table 3). Neither the efficacy nor
suppression and have behaviors and concerns that parallel
the potential negative effects of lifestyle changes on a
those who have evidence of mucosal damage. Patients with
patient’s quality of life have been adequately examined for
endoscopic-negative GERD and who do not respond to
any of these modifications. With relatively little data
medications are best evaluated by ambulatory pH
available, it is reasonable to educate patients about factors
monitoring. On average, patients with endoscopic-negative
reflux have less acid exposure than those with esophagitis,
but more compared to people without reflux. However,
Head elevation. Numerous studies have indicated that
normal acid exposure has been found in up to 29% of
the elevation of the head of a patient’s bed by 4 to 8 inches,
patients with documented reflux esophagitis and in up to
as well as avoiding recumbency for 3 hours or greater after
33% of patients with endoscopic-negative GERD.
a large or fatty meal, may decrease distal esophageal acid
exposure. However, data reflecting the true efficacy of this
Ambulatory pH monitoring is based upon the amount of
maneuver in patients is almost completely lacking. It has
time the intraesophageal pH is less than 4, with normal
also been suggested that patients should avoid sleeping on
defined as less than 4% over a 24-hour period. Patients are
additional pillows, as this may increase abdominal pressure
expected to perform their usual activities with dietary and
lifestyle restrictions minimized in order to improve the
Avoid certain foods. Several foods are believed to be
direct esophageal irritants: citrus juices, carbonated
Recent advances in “wireless” pH radiotelemetry capsule
beverages, coffee and caffeine, chocolate, spicy foods, fatty
technology eliminates the need for the uncomfortable
foods, or late evening meals. However, no randomized
nasoesophageal tube, and increases diagnostic yield by
controlled trials to support recommendations to avoid or
allowing for longer monitoring (e.g., now 48-hour and soon
minimize these foods. Individualized dietary modification
96-hour). Also, intraluminal impedance monitoring can
detect “nonacid” (i.e. liquid/gas) reflux, which may be
important in medically refractory patients with regurgitation
Weight loss. An association among weight, reflux and
who are being considered for surgery or in patients with
reflux complications has been demonstrated. Weight loss
atypical symptoms. Correlating symptoms with reflux
has been shown to improve global symptom scores,
events is important in those with EGD-negative GERD and
particularly if weight gain occurred before the onset of
is helpful in the evaluation of those with extraesophageal or
sporadic symptoms. The symptom index associates
Smoking cessation and alcohol minimization.
maximal therapy, the disadvantages include cost, which
Smoking cessation and the elimination or minimization of
may exceed or equal the cost of a proton-pump inhibitor, as
alcohol are also encouraged for a variety of health reasons.
Both nicotine and alcohol have been shown to lower LES
pressure and lead to further esophageal irritation. A recent
No randomized controlled trials exist to examine the course
systematic review found that smoking was associated with
of incompletely treated GERD, nor are good data available
an increase in GERD symptoms (over 1-2 days), yet
on the natural history of inflammatory esophageal disease.
smoking cessation was not shown to decrease GERD
Little information is available on the level of gastric acid
symptoms in 3 low-quality studies. Alcohol use may or
suppression that is needed to ensure adequate esophageal
may not be associated with reflux symptoms.
Avoid medications that lower LES pressure.
Patients seem to develop some tolerance to the H2RAs,
Medications that lower LES pressure should be avoided in
with some decreased efficacy observed after 30 days of
patients with symptoms of GERD. These medications
include calcium channel blockers, β-agonists, α-adrenergic
agonists, theophylline, nitrates, and some sedatives.
In the short term, randomized controlled trials with patients
on placebo found similar rates of adverse effects as
Avoid tight clothing around waist. Another anecdotal
compared to the RCTs with patients on H2RAs. Most
suggestion is that patients refrain from wearing tight
evidence describing adverse effects is from case reports or
clothing around the waist to minimize strain-induced reflux.
uncontrolled trials. H2RAs have been associated with rare
cytopenias, gynecomastia, liver function test abnormalities,
Over-the-counter (OTC) remedies. Antacids and OTC
and hypersensitivity reactions. In the long-term, no
acid suppressants are appropriate, initial patient-directed
controlled trials with follow-up on the safety of chronic use
therapy for GERD. Antacids (Tums, Rolaids, Maalox) and
combined antacid/alginic acid (Gaviscon) have been shown
to be more effective than placebo in the relief of daytime
Proton Pump Inhibitors (PPIs). Solid evidence from
GERD symptoms. Two long-term studies suggest that
numerous randomized controlled trials has shown that PPIs
approximately 20% of patients experience some relief from
are more effective than both H2RAs and placebo in
controlling symptoms from erosive reflux disease (83%
compared to 60% and 27%, respectively) over a 4 to 8 week
All four of the histamine type-2 receptors antagonists
period. One systematic review compared the efficacy of
(H2RAs: cimetidine, famotidine, nizatidine, and ranitidine)
PPIs and H2RAs and found that a greater number of people
have been approved for use in the US as OTC preparations
improved symptomatically with PPIs, yet the difference
at a dose that is uniformly one-half of the standard lowest
was not significant for heartburn remission. One RCT
prescription dosage for each compound; ranitidine is now
showed that at 12 months, significantly more people were
available in an OTC formulation at standard dose. At these
still in remission with omeprazole compared to ranitidine.
dosages, the H2RAs decrease gastric acid production,
Another RCT found that treatment with omeprazole was
particularly in the postprandial state, without affecting
more likely than ranitidine to improve symptom and
esophagogastric barrier dysfunction. The four compounds
are virtually interchangeable at these dosages, with
similarities in the rapidity and duration of action. The OTC
In the treatment of erosive esophagitis, PPIs had faster
costs are equivalent (although the generic costs differ by
healing rates than either H2RAs or placebo (78% compared
dosage). Some patients may predict when they will suffer
to 50% and 24%, respectively) over a 4-8 week period. No
reflux symptomatology and may benefit from pre-
RCTs have examined therapy for a longer period of time.
medication with these OTC H2RAs. The OTC H2RAs are
believed to be superior in efficacy when compared to
One RCT found no evidence of a significant difference
among the PPIs, including omeprazole, lansoprazole,
rabeprazole and pantoprazole in the healing of erosive
H2 antagonists (H2RAs). Numerous randomized,
esophagitis. Efficacy in pH changes was not studied. The
controlled trials have demonstrated that standard
least expensive PPI is omeprazole, which is available
prescription dose H2RAs are more effective than placebo at
generically and OTC. A single study showed that
relieving heartburn in cases of GERD, with symptomatic
esomeprazole, the S-isomer of omeprazole, at doses of 20
relief reported in 60% of cases. A systematic review found
mg and 40 mg is more effective than omeprazole 20 mg in
that people in trials on H2RAs had faster healing rates than
healing and symptom resolution in GERD patients with
people in trials on placebo: over a 4-8 week period a healed
reflux esophagitis, with a tolerability profile comparable to
esophagitis rate of 50% on H2RA and 24% on placebo.
that of omeprazole. A recent randomized controlled trial
compared esomeprazole 40 mg to lansoprazole 30 mg.
Both higher doses and more frequent dosing of H2RAs
Esomeprazole was superior in healing and symptom
appear to be more effective in the treatment of reflux
control, with superiority highest in more severe degrees of
symptoms and healing of esophagitis. If the patient is on
Newer endoscopic treatments. Radiofrequency heating of
The potential benefit of chronic PPI therapy in patients with
the GE junction (Stretta) and endoscopic gastroplasty
chronic or complicated GERD generally outweighs any
(Bard, Wilson Cook), polymer injections to bolster the GE
theoretical risk of adverse events. Decreased cobalamin
junction, and full thickness gastroplication have all been
absorption has been found, although a clinically significant
shown to improve symptoms and quality of life scores in
decrease in serum vitamin B12 levels is not usually seen.
sham controlled trials. None of these techniques have
PPIs cause a profound decrease in gastric acid secretion,
consistently reduced acid exposure. Polymer injections
which leads to an increase in gastrin production from the
have been removed for safety concerns. Durability of
antral G-cells. No cases of gastric cancer/carcinoid linked
response for all of these modalities (30-50% at 3 years) may
to use of the PPIs have been reported since the advent of
limit long term usefulness. Complications are relatively
this class of medication over 20 years ago. PPIs have been
rare in experienced hands and are less than with standard
associated with rare community-acquired pneumonia,
Clostridium difficile colilis, and hip fracture.
Treatment Failure
Several studies have demonstrated that on-demand therapy
with PPIs is the most cost-effective method for NERD
Empiric trials should be limited if no response is seen.
Treatment response should be present in 2-4 weeks for
patients with typical symptoms. Patients with atypical
Surgical treatment. Anti-reflux surgery is an accepted
symptoms also have an initial response in one month, but
alternative treatment for symptomatic acid/bile reflux. The
may require 3-6 months for maximal response. Patients
basic tenets of surgery are reduction of the hiatal hernia,
with atypical symptoms may require higher PPI doses for
repair of the diaphragmatic hiatus, strengthening the
response. Empiric treatment in patients with atypical
gastroesophageal junction-posterior diaphragm attachment,
symptoms is appropriate if typical symptoms are also
and strengthening the anti-reflux barrier by adding a gastric
present. Esophageal pH monitoring off of anti-reflux
wrap around the gastroesophageal junction
medications might be the best approach initially in patients
(fundoplication). Open and laparoscopic surgical repairs
with atypical symptoms only since <30% of patients will
are available. Controlled trials comparing open and
have GERD associated symptoms. If patients with atypical
laparoscopic approaches have shown similar efficacy and
symptoms do not respond to treatment in 1-3 months, then
complications with lower morbidity and shorter hospital
GERD is not likely the cause and the other diagnoses
Post-surgical complications are common, but typically short
Maintenance Regimens
term and manageable in most instances. Short term solid
food dysphagia occurs in 10% of patients (2-3% have
The goal of maintenance therapy is to have a symptom free
permanent symptoms) and gas bloating occurs in 7-10% of
individual with no esophagitis. Multiple regimens are used
patients. Diarrhea, nausea and early satiety occur more
to accomplish this. Increasing severity of esophagitis is
rarely. While some complication occurs in up to 20% of
associated with increasing need for potent acid reduction
patients, major complications occur in only 3-4% of
patients. Patient satisfaction is high when GERD
Since most individuals with GERD do not undergo
endoscopy, chronic acid suppression is tailored to the
Controlled trials comparing anti-reflux surgery to antacids,
individual. Options include: step-up therapy (starting less
H2 receptor antagonists and proton pump inhibitors have
potent agents and moving up for treatment response), step-
shown marginal superiority to surgery. Recent studies
down therapy (using potent acid suppression initially with
comparing surgery with proton pump inhibitors have shown
decreasing dose or less potent agents to tailor to the
similar efficacy if PPI could be titrated to response. Long-
individuals response), on demand (patient-directed)
term follow-up trials have shown that 52% of patients are
therapy, or surgery, All options have the goal of complete
back on anti-reflux medications 3-5 years after surgery,
most likely secondary to a combination of poor patient
Step-up therapy. When beginning step-up therapy, no
more than 2 weeks is needed to determine if a dosage of
The choice to consider anti-reflux surgery must be
medication will be effective. If a patient does not respond
individualized. Patients should have documented acid
to an H2 receptor antagonist within 2 weeks, the patient
reflux, a defective anti-reflux barrier in the absence of poor
should be switched to a proton pump inhibitor, again
gastric emptying, normal esophagus motility and at least a
emphasizing it be used 30 minutes to 1 hour prior to meals
partial response to acid reduction therapy. Surgery appears
so that the PPI has time to interact with an activated pump.
to be most effective for heartburn and regurgitation (75-
90%) and less effective for extraesophageal symptoms (50-
If the patient does not respond to this program, a double-
dose program (BID; 30 minutes before breakfast and 30
minutes before dinner) may be effective in reducing
symptoms. If the patient does not respond to this program,
bronchospasm/asthma). Laryngeal neuropathy has been
the patient is likely not to have reflux as a source of their
implicated recently as a cause for laryngitis symptoms and
symptoms and diagnostic testing would be appropriate.
Approximately 40% of patients requiring PPI therapy will
Pulmonary. Asthma and GERD are common conditions
need increasing dosage over time. Tolerance to H2 receptor
that often coexist with 50-80% of asthmatics having GERD
antagonists occurs over time. The main goal is to use the
and up to 75% having abnormal pH testing. However, only
lowest dose and least potent medication to obtain a
30% of patients who have both GERD and asthma will have
complete and sustained symptomatic response.
GERD as the cause for their asthma. The causal
relationship between asthma and GERD is difficult to
Break through symptoms are common and the patients can
establish because either condition can induce the other
use antacids and/or nocturnal H2 receptor antagonists.
(GERD causing asthma as above, and asthma causing
These should be limited to individuals who are not getting
increased reflux by creating negative intrathoracic pressure
symptomatic response, yet have defined reflux as their
and overcoming LES barrier). Furthermore, medications
source of symptoms. This would be a very small number of
used for asthma, such as bronchodilators, are associated
patients. H2 receptor antagonists should not be
with increased reflux symptomatology. Historical clues to
GERD-related asthma may include asthma symptoms that
worsen with big meals, alcohol, and supine position, or
Step-down therapy. Once symptoms are controlled after
adult-onset and medically refractory asthma. Diagnostic
step-up therapy, step-down therapy commences with the
testing with pH probe and EGD have limited utility in
patient taking a PPI for 8 weeks, followed by an H2RA if
establishing causality in this population.
GERD symptoms were adequately controlled with a PPI,
then stepping down further to on-demand use of antacids if
Ear, nose, and throat. In patients presenting with ENT
the patient was asymptomatic while taking an H2RA. The
symptoms, 10% of hoarseness, up to 60% of chronic
majority of patients who take more than a single daily dose
laryngitis and refractory sore throat, and 25-50% of globus
of a PPI and who experience relief of symptoms can be
sensation may be due to reflux. EGD and pH testing are
successfully stepped down to single-dose therapy without a
frequently normal in this population. Reflux laryngitis is
recurrence of reflux symptoms. However, a small
usually diagnosed based on the laryngoscopic findings of
percentage of patients with refractory GERD will need
laryngeal erythema and edema, posterior pharyngeal
long-term therapy with higher doses of a PPI to control
coblestoning, contact ulcers, granulomas, and interarytenoid
changes. However, a recent study found these signs to be
nonspecific for GERD, noting at least 1 sign in 91 of 105
On demand therapy. Treatment can be initiated with
(87%) healthy people without reflux or laryngeal
standard dosage of either a PPI daily or an H2RA twice
complaints. Many of these signs may be due to other
daily on demand (patient directed therapy). Drug selection
laryngeal irritants such as alcohol, smoking, postnasal drip,
depends on clinical presentation, cost-effectiveness, and
viral illness, voice overuse, or environmental allergens,
end point of appropriate symptom relief.
suggesting their use may contribute to overdiagnosis of
GERD. This also may explain why many patients (up to
Special Circumstances
40-50%) with laryngeal signs don’t respond to aggressive
acid therapy. Posterior laryngitis, medial erythema of
Older Adults
false/true vocal cords and contact changes (ulcers and granulomas) are more common in GERD patients and
predict a better response to acid reduction.
In a patient over the age of 50, new onset of GERD is an
alarm sign and endoscopy should be the initial diagnostic
Treatment. Aggressive acid reduction using PPIs BID
examination. If reflux is still considered the major cause
before meals for at least 2-3 months is now considered the
after negative endoscopy, empiric therapy would then be
standard treatment for atypical GERD and may be the best
way to demonstrate a causal relationship between GERD
and extraesophageal symptoms. Recent double blind,
Atypical Manifestations of GERD
placebo controlled trials have not shown significant benefit
for PPI BID treatment for laryngeal symptoms. Similar
As noted in Table 1, GERD may manifest atypically as
trials in asthma have shown marginal benefits in FEV
pulmonary (asthma, chronic cough), ENT (laryngitis,
only when nocturnal GERD symptoms are also present.
hoarseness, sore throat, globus, throat clearing) or cardiac
Both groups of studies demonstrate the need for better
(chest pain) symptoms, often without symptoms of
parameters for patient selection. Anti-reflux surgery aimed
heartburn and regurgitation. Mechanisms for this include
at controlling asthma through prevention of GERD has a
direct contact and microaspiration of small amounts of
lower rate of success than anti-reflux surgery aimed at
noxious gastric contents into the larynx and upper bronchial
treating heartburn (45-50% vs. 80-90% respectively).
tree (triggering local irritation, and cough), and acid
stimulation of vagal afferent neurons in the distal esophagus (causing non-cardiac chest pain and vagally-mediated
A systematic review on chronic cough found there is
Controversial Areas
insufficient evidence to definitely conclude that PPI
treatment is beneficial for cough associated with GERD in
Screening for Barrett's Esophagus
adults, although a small beneficial effect was seen in
GERD is the major cause for esophageal adenocarcinoma
(68-90%). Adenocarcinoma is more common (30-60x) in
patients with GERD and increases with increased frequency, severity and duration of reflux symptoms.
Initial screening is appropriate especially in Caucasian males over age 50 and in patients with reflux symptoms for more than 10 years. If Barrett’s esophagus and/or esophagitis is not found on initial endoscopy, repeat surveillance is not indicated unless the patient has a major change in symptoms. Surveillance of known Barrett’s esophagus is controversial because adenocarcinoma of the esophagus is rare in the US (6000-7000 cases/yr) and GERD/Barrett's occur in 0.4- 0.8% of the population. The discounted cost per quality adjusted patient year for surveillance is expensive ($100,000-$500,000). Current recommendations are for repeat endoscopy every two years. Follow-up of patients with dysplasia should be more frequent. Surveillance should stop if patient’s clinical situation would preclude esophageal resection. Endoscopic treatments such as thermal ablation, photodynamic therapy and endoscopic mucosal resection offer promise to the patient who is not an operative candidate. They are likely to have fewer complications, but also lower effectiveness (60-70% loss of cancer/high grade dysplasia at 2 years follow-up). Hidden cancers or high grade dysplasia below the epithelial surface may hamper endoscopic monitoring. Treatment for H. pylori
Patients with predominant GERD symptoms have a similar or lower frequency of H. pylori positivity than the general population. Successful treatment of H. pylori has not been shown to reduce predominant GERD symptoms. Some studies have shown decreased PPI effectiveness post successful H. pylori treatment, but this is still controversial. One RCT demonstrated that H. pylori eradication leads to more resilient GERD. Treatment of H. pylori is not indicated for patients with GERD. Related National Guidelines
This guideline is consistent with the American College of Gastroenterology’s Updated Guidelines for the Diagnosis and Treatment of Gastroesophageal Reflux Disease (2005) and the VA/DoD Clinical Practice Guideline for the Management of Adults with Gastroesophageal Reflux Disease in Primary Care Practice (2003). (See annotated references.)
Strategy for Literature Search Disclosures
The literature search began with the results of the literature
The University of Michigan Health System endorses the
search performed through September 2000 for the previous
Guidelines of the Association of American Medical
version of this guideline. The results of two more recent
Colleges and the Standards of the Accreditation Council for
Continuing Medical Education that the individuals who
American College of Gastroenterology: Updated
present educational activities disclose significant
Guidelines for the diagnosis and treatment of
relationships with commercial companies whose products
gastroesophageal reflux disease (2005), literature search
or services are discussed. Disclosure of a relationship is not
intended to suggest bias in the information presented, but is made to provide readers with information that might be of
VA/DOD Clinical Practice Guideline for the
potential importance to their evaluation of the information.
Management of Adults with Gastroesophageal Reflux
Disease in Primary Care Practice (2003), literature search through May 2002.
A search of more recent literature was conducted
prospectively on Medline from January 2004 through May
2006 using the major keywords of: gastroesophageal reflux disease (or GERD, NERD [non-erosive reflux disease], NEED [non-erosive esophageal disease]), human adults, English language, clinical trials, and guidelines. Terms
used for specific topic searches within the major key words
included: symptoms (atypical symptoms, heartburn, retrosternal burning sensation precipitated by meals or a recumbent position, hoarseness, laryngitis, sore throat, chronic cough, chest pain, bronchospasm/asthma, dental Annotated References erosions)nocturnal (or nocturnal breakthrough, night time), endoscopy, pH recording, manometry, provocative testing
American College of Gastroenterology: DeVault KR,
(Bernstein’s), video esophagography, empiric/therapeutic
Castell DO. Updated Guidelines for the Diagnosis and
trial to acid suppression, lifestyle measures/treatment
Treatment of Gastroesophageal Reflux Disease. American
(avoiding fatty foods, chocolate, peppermints, ethanol-
Journal of Gastroenterology, 2005; 100:190-200.
containing veverages; recumbency for 3 hours after a meal; elevating head of bed; weight loss), antacids, alginic acid
A consensus statement outlining the current
(gaviscon), carafate, prokinetic agents (cisapride,
recommendations by the American College of
metoclopramide, bethanechol, dromperidone), H2 receptor
Gastroenterology in the diagnosis and treatment of
antagonists (nizatidine, ranitidine, famotidine, cimetidine), proton pump inhibitors (omeprazole, lansoprazole, rabeprazole, pantoprazole, esomeprazole), fundoplication
American College of Gastroenterology: DeVault KR.
(open vs. laproscopy; endoscopic antireflux procedures),
Updated Guidelines for the Diagnosis and Treatment of
Barretts esophagus (screening, surveillance). Detailed
Gastroesophageal Reflux Disease. American Journal of
search terms and strategy available upon request.
Gastroenterology, 1999; 94(6):1434-1442.
This earlier consensus statement includes information
The search was conducted in components each keyed to a
that is simply referenced in the more recent update
specific causal link in a formal problem structure (available
upon request). The search was supplemented with very
recent information available to expert members of the
VA/DoD Clinical Practice Guideline for the Management
panel, including abstracts from recent meetings and results
of Adults with Gastroesophageal Reflux Disease in Primary
of clinical trials. Negative trials were specifically sought.
Care Practice. Department of Veterans Affairs and
Department of Defense, Draft 8a, March 12, 2003.
Conclusions were based on prospective randomized clinical
A 60 page report addressing each aspect of diagnosis
trials if available, to the exclusion of other data; if
randomized controlled trials were not available,
observational studies were admitted to consideration. If no
Heidelbaugh JJ, Nostrant TT. A Cost-Effective Approach
such data were available for a given link in the problem
to the Pharmacologic Management of Gastroesophageal
formulation, expert opinion was used to estimate effect size.
Reflux Disease. Drug Benefit Trends 2004;16:463-471.
An in-depth examination of various cost-effective approaches to GERD treatment
Heidelbaugh JJ, Nostrant TT. Medical and surgical management of gastroesophageal reflux disease. In: Heidelbaugh JJ (ed). Clinics in Family Practice: Gastroenterology. Philadelphia, PA: Elsevier, September 2004, 6(3):547-568.
A systematic review of the literature and evidence-based recommendations for practice in the diagnosis and treatment of GERD.
Kahrilas, PJ. Gastroesophageal Reflux Disease. JAMA. 1996;276(12):983-988.
A comprehensive review of treatment of GERD with less emphasis on diagnostic modalities.
Numans Me, Lau J, deWit NJ, Bonis PA. Short-term treatment with proton-pump inhibitors as a test for gastroesophageal reflux disease: a meta-analysis of diagnostic test characteristics. Annals of Internal Medicine, 2004; 140(7):518-27.
A systematic review of this literature, with 15 studies showing the limited sensitivity and specificity of successful short-term treatment with PPI in establishing the diagnosis when GERD is defined by 24-hour pH monitoring.
Sridhar, S. Clinical economics review: cost-effectiveness of treatment alternatives for gastro-oesophageal reflux disease. Alim Pharmacol Ther 1996;10:865-873.
An economic appraisal reviewing different treatment modalities and their cost-effectiveness. Proton pump inhibitors are considered more cost effective than H2 receptor antagonists in those with documented erosive esophagitis.
Vaezi, M. Gastroesophageal reflux disease and the larynx. J Clin Gastroenterol, 2003; 36(3):198-203.
Presents the rational for an approach to identifying patients whose laryngeal signs and symptoms are due to GERD.
A Parent’s Guide to Sports-Related Skin Infections Prepared by: Nick Esmonde, MS-3 OHSU School of Medicine Pioneer Memorial Hospital Preceptor: Russell Nichols, MD This guide was designed to inform parents of student-athletes about the most common or serious sports-related skin infections. If an athlete has new skin lesions or infections, they should see their primary care doctor for evaluation
PREDICTING THE EFFECTIVENESS OF HYDROXYUREA IN INDIVIDUAL SICKLE CELL ANEMIA PATIENTS Homayoun Valafar, Faramarz Valafar, Alan Darvill and Peter Albersheim, Complex Carbohydrate Research Center and the Department of Biochemistry and Molecular Biology, University of Georgia, 220 Riverbend Road, Athens, GA 30602 Abdullah Kutlar, Kristy F. Woods, and John Hardin, Department of Medicin

 University of Michigan
University of Michigan 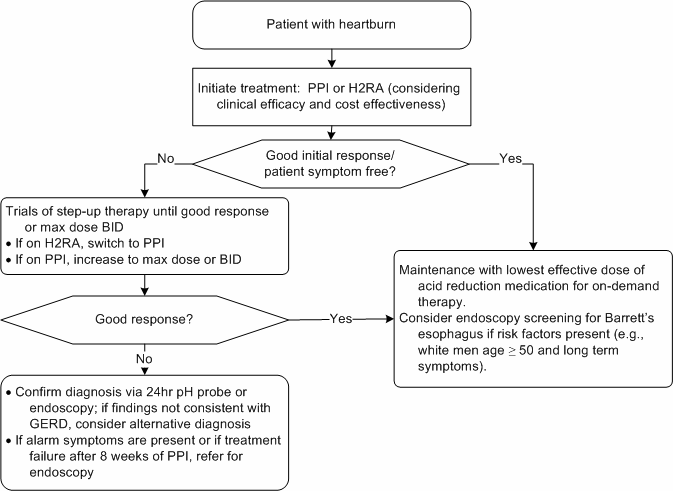 Figure 1. Diagnosis and Treatment of GERD
Figure 1. Diagnosis and Treatment of GERD