CLINICAL OBSERVATIONS, INTERVENTIONS, AND THERAPEUTIC TRIALS
Antiphospholipid antibodies and antiphospholipid syndrome in patients presentingwith immune thrombocytopenic purpura: a prospective cohort study
Reyhan Diz-Ku¨c¸u¨kkaya, Abdullah Hacıhanefiogˇlu, Mustafa Yenerel, Mehmet Turgut, Hu¨seyin Keskin, Meliha Nalc¸acı, and Murat l˙nanc¸
The pathogenetic role and the clinical initial platelet counts, or response to methyl- ing the initial platelet counts, response to importance of the presence of antiphos- prednisolone therapy. After 5 years of follow- the therapy, or ACA positivity. The positivity pholipid antibodies (APAs) in patients up, cumulative thrombosis-free survival of rate for LA was significantly higher in those with immune thrombocytopenic purpura APA-positive (n ؍ 31) and APA-negative patients with ITP who developed APS (2: (ITP) are not clear. In this study, the (n ؍ 51) ITP patients was 39% and 97.7%, P ؍ .0036; relative risk 7.15; 95% confi- prevalence and clinical significance of respectively. A significant difference was dence interval, 1.7-47). In conclusion, this APAs were investigated in patients with found between these groups by log-rank study indicates that a significant proportion ITP. Eighty-two newly diagnosed ITP pa- test (P ؍ .0004). In addition, LA was an im- of patients initially presenting with ITP and tients were prospectively studied. They portant risk marker for the development of APA positivity developed APS. In patients were evaluated for the presence of lupus thrombosis in ITP patients. After a median with ITP, the persistent presence of APAs is anticoagulant (LA) and immunoglobulin G/M follow-up of 38 months, 14 ITP patients an important risk factor for the development anticardiolipin antibodies (ACAs). Thirty- (45%) who had APA positivity developed of APS. (Blood. 2001;98:1760-1764) one patients (37.8%) were APA positive at clinical features (thrombosis or fetal losses) diagnosis. No statistically significant differ- of antiphospholipid syndrome (APS). There ences were found between the APA-positive were no differences between the APA-posi- and APA-negative groups regarding gender, tive patients with and without APS regard- 2001 by The American Society of Hematology Introduction
Immune (idiopathic) thrombocytopenic purpura (ITP) is an autoim-
on APS, thrombocytopenia was not included in the preliminary
mune disease defined by a low platelet count secondary to
accelerated platelet destruction by antiplatelet antibodies that
Because of our observation that some ITP patients with
generally recognize platelet membrane glycoproteins (GPs). An-
persistently positive APAs developed thrombosis after several
tiphospholipid syndrome (APS) is characterized by arterial and
years of follow-up, we decided to investigate APA-positive ITP
venous thrombosis, recurrent fetal loss, and thrombocytopenia in
patients prospectively for the development of APS. In the present
the presence of antiphospholipid antibodies (APAs).
study, newly diagnosed ITP patients were prospectively evaluated
Thrombocytopenia is reported in about 20% to 40% of patients
for APA positivity and clinical features of APS.
with APS and is usually mild.1 Although there is direct evidencethat APAs may bind platelet membranes and cause plateletdestruction, the relation between APA positivity and thrombocyto-
Patients and methods
penia is still unclear. Some investigators suggest that antibodiesother than APA, mainly those against GPIIb-IIIa and other mem-
We studied 82 patients who were newly diagnosed with ITP in our
brane GPs, cause thrombocytopenia in patients with APS.2,3
Hematology Division between July 1993 and July 1999. Their median age
Although Harris et al4 found anticardiolipin antibodies (ACAs)
was 31 years (range, 16-70 years) at the time of diagnosis (Table 1). Medianfollow-up was 32 months (range, 6-72 months). ITP was diagnosed by
in 30% of ITP patients at the time of diagnosis, many researchers
medical history, physical examination, peripheral blood smear, and bone
have questioned the clinical significance of this observation.
marrow aspiration. Patients who were referred with bleeding complaints
Elevated levels of APAs are common in ITP and often do not
(easy bruising, purpura, mucosal bleeding) and had isolated thrombocytope-
change significantly with immunosuppressive therapy. In addition,
nia with no history of other clinical conditions that can cause thrombocyto-
ITP patients with normal and elevated levels of APAs had similar
penia were included in our study. Peripheral blood smears and bone marrow
clinical profiles.5 The development of APS was found to be
smears were examined to rule out other causes of thrombocytopenia in all
uncommon in the long-term observation of chronic ITP patients.6
patients. At the time of the ITP diagnosis, patients were excludedfrom further study if they had a history or clinical findings of APS,
Because of this observed lack of clinical association between these
systemic lupus erythematosus (SLE), other autoimmune disorders,
antibodies and ITP, the American Society of Hematology ITP
acquired immunodeficiency syndrome, or malignancies. Although the
Practice and Guideline Panel recommended that evaluating ITP
upper limit for thrombocytopenia was accepted as 140 ϫ 109/L, only 5
patients for APAs is unnecessary.7 Similarly, in a recent symposium
patients had platelet counts greater than 100 ϫ 109/L (maximum level
From the Divisions of Hematology and Rheumatology, Department of Internal
Istanbul, 34750, Turkey; e-mail: [email protected].
Medicine, Istanbul Faculty of Medicine, Istanbul University, Turkey.
The publication costs of this article were defrayed in part by page chargepayment. Therefore, and solely to indicate this fact, this article is hereby
Submitted November 29, 2000; accepted May 21, 2001.
marked ‘‘advertisement’’ in accordance with 18 U.S.C. section 1734. Reprints: Reyhan Diz-Ku¨c¸u¨kkaya, Atako¨y 5. Kısım, C9 Blok, D: 4 Bakırko¨y,
2001 by The American Society of Hematology
BLOOD, 15 SEPTEMBER 2001 ⅐ VOLUME 98, NUMBER 6
Table 1. Characteristics of the patients
A total of 31 patients (37.8%) were found to be positive for APAs at the
time of diagnosis (Table 1). Fourteen patients developed thrombosis or fetal
loss in the presence of APAs (group A). APA-positive ITP patients without
APS symptoms were classified as group B. The clinical and laboratory
findings of the 2 groups were compared. Kaplan-Meier procedure, log-rank
test, and Fisher exact test were used for statistical analysis. Relative risks
(RRs) and confidence intervals (CIs) were calculated with the Instat
(Graphpad Software, San Diego, CA) and SPSS (Prentice Hall, Upper
Saddle River, New Jersey) computer programs.
Thirty-one patients (37.8%) were found to be positive for APAs atthe time of the ITP diagnosis (Table 1). We found no statistically
NS indicates not significant; CR, complete remission; MP, methylprednisolone;
significant differences between the APA-positive and APA-
negative groups for gender ratio, initial platelet counts, or responseto methylprednisolone therapy. Although the initial platelet counts
was 117 ϫ 109/L). Patients with mild thrombocytopenia (101-140 ϫ 109
were similar, follow-up with no treatment was found to be higher in
platelets/L) or moderate thrombocytopenia (51-100 ϫ 109 platelets/L)
APA-positive patients (2: P ϭ .017; RR ϭ 0.4; 95% CI, 0.15-1.0).
did not receive any therapy unless they had bleeding symptoms or were
Only one patient developed thrombosis or recurrent fetal losses in
to have surgical intervention. Patients who had moderate to severethrombocytopenia (0-50 ϫ 109 platelets/L) with bleeding complications
the APA-negative group. Only one patient developed acute myocar-
received oral methylprednisolone at 1-mg/kg doses for 1 month. The
dial infarction at the 14th month of follow-up in the APA-
methylprednisolone doses were tapered in those patients who responded
to therapy. Splenectomy was performed in patients who were resistant to
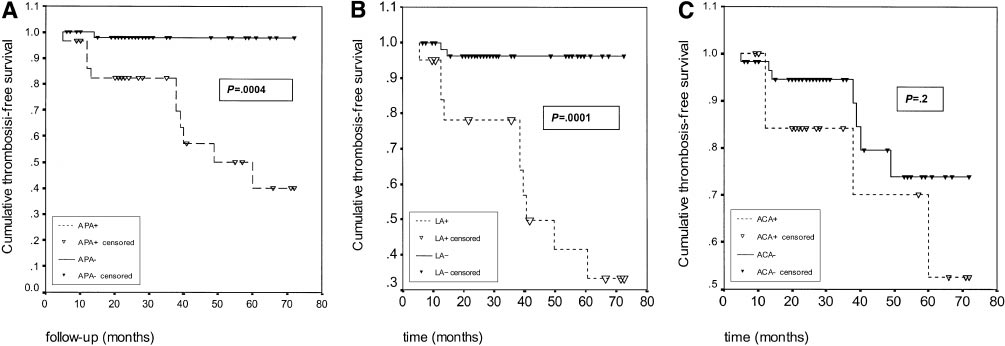
We compared the thrombosis-free survival of patients who were
methylprednisolone. Patients unresponsive to splenectomy received
APA positive (n ϭ 31) with those who were APA negative at
additional treatment with other drugs (azathioprine, vincristine, danazol,
presentation (n ϭ 51) by Kaplan-Meier test (Table 2). After 5 years
or intravenous immunoglobulin) (Table 1).
of follow-up, cumulative thrombosis-free survival rates of APA-
A predefined protocol for APS was used for the assessment of all
positive and APA-negative ITP patients were 39.9% and 97.7%,
patients included in the study. All patients with APS were seen by one of our
respectively (Figure 1A). These data were found to be highly
authors (M.I˙.) who is a member of the rheumatology unit. The finaldiagnoses were made for all patients by 2 of the authors. The diagnosis of
statistically significant by log-rank test (P ϭ .0004). We also
thromboembolic events was done by other specialists in emergency
analyzed the effect of the positivity of LA, ACA total, ACA IgG
situations without knowledge of the patient’s APA status, and later patients
(both greater than 10 GPL and greater than 20 GPL), and ACA IgM
(both greater than 10 MPL and 20 MPL) on thrombosis-free
APS was diagnosed in patients who had arterial or venous thrombosis
survival of ITP patients (Table 2). We found a highly statistically
and/or recurrent fetal losses in the presence of ACAs, lupus anticoagulant
significant difference for LA positivity (P ϭ .0001 by log-rank test)
(LA), or both. Doppler ultrasonography, ventilation and perfusion scanning
(Figure 1B). Although ACA IgG levels greater than 10 GPL units
of the lung, computed tomography, magnetic resonance imaging, and
were found to be a risk marker for developing thrombosis in
retinal angiography were used for documentation of thrombotic complica-
patients with ITP, we found no significant difference for ACA total
tions. Three or more unexplained spontaneous abortions were considered
(Figure 1C) or ACA IgM positivity (Table 2). The comparisons of
recurrent fetal losses. ITP patients who had 2 unexplained fetal losses andhad positive tests for APAs were also regarded as having APS and were
both the LA-positive and ACA-positive (greater than 10 GPL/
treated with aspirin or low-molecular-weight heparin in their consecutive
MPL) patients with the others were also found to be statistically
pregnancies. ACA immunoglobulin G (IgG) and IgM levels were screened
by enzyme-linked immunosorbent assay as described elsewhere.9 Samples
The patients who presented with ITP and subsequently devel-
of 0 to 10 GPL or MPL units (measuring IgG and IgM anticardiolipin
oped APS were designated group A (Table 3). Thirteen of them
antibodies, respectively) were regarded as negative, 11 to 19 units were
(92.8%) were positive for LA. KCT was prolonged in all LA-
regarded as low positive, 20 to 60 units were regarded as positive, and more
positive patients (100%), and aPTT was prolonged in 10 patients
than 60 units were regarded as high positive for both ACA IgG and ACA
(77%). Twelve patients were screened for ACAs; 7 had ACA IgG
IgM. LA was diagnosed according to the criteria of the International Society
positivity, IgM positivity, or both (Table 3). The median interval
of Haemostasis and Thrombosis.10 Fresh citrated venous blood sampleswere used for LA testing. All plasma samples were centrifuged at 2000g for
between the diagnosis of ITP and the first clinical symptom of APS
15 minutes and filtered through 0.22- filters, and both the activated partial
thromboplastin time (aPTT) and the kaolin clotting time (KCT) were
Four patients (nos. 2, 4, 8, and 12) did not receive any therapy at
measured twice. The results were compared with those from filtered,
the time of ITP diagnosis because of mild or moderate thrombocy-
normal pooled plasma, which was collected from at least 10 normal
topenia with no bleeding symptoms, and all subsequently devel-
controls. The aPTT and KCT were considered to be prolonged if they were
oped thrombosis. One patient (no. 9) achieved normal platelet
more than 3 SDs longer than the control (39 seconds for aPTT; 88 seconds
counts after methylprednisolone therapy, and APA positivity per-
for KCT). In mixing studies, the patients’ plasma samples were mixed 1:1
sisted. She has experienced 2 second-trimester fetal losses during
with normal pooled plasma, and both aPTT and KCT were performed on all
follow-up. Six patients (nos. 1, 5, 10, 11, 13, and 14) achieved
samples. Frozen-thawed platelets were used for the platelet neutralizationtest. Although it has been recommended that partial correction might
partial remission of thrombocytopenia after methylprednisolone
suggest phospholipid dependence,10 complete correction was obtained in all
therapy. Five of 6 have developed thrombosis. Three patients
LA-positive samples. The LA and ACA levels were repeated at intervals of
who had no response to methylprednisolone underwent splenec-
tomy (nos. 3, 6, and 7). One of them (no. 7) developed deep
BLOOD, 15 SEPTEMBER 2001 ⅐ VOLUME 98, NUMBER 6
Table 2. Thrombosis-free survival analysis of the patients by Kaplan-Meier procedure
TFS indicates thrombosis-free survival. *The patients who had both LA positivity and ACA IgG and/or IgM levels greater than 10 GPL/MPL units were included in this group. †The group included patients who had APA negativity and either LA positivity alone or ACA positivity alone.
vein thrombosis and pulmonary embolism during the postopera-
decreased visual acuity. Five patients experienced arterial throm-
tive period, and one patient (no. 6) developed mesenteric
botic events: 4 had stroke (nos. 5, 8, 10, and 14) and one had
embolism immediately before splenectomy. These 2 patients
mesenteric artery embolism (no. 6). Permanent right-sided hemiple-
had platelet counts greater than 100 ϫ 109/L at the time of
gia developed in one patient with stroke (no. 10), and the remaining
patients recovered with residual impairment. The thromboembolic
A total of 6 venous thrombotic events were documented in
complications developed when the platelet counts exceeded
group-A patients. Five patients (nos. 1, 4, 7, 12, and 13) experi-
100 ϫ 109 platelets/L in all but one patient. In patient 10, stroke
enced deep vein thrombosis, and 2 patients (nos. 4 and 7) also had
developed with a platelet count of 30 ϫ 109 platelets/L.
pulmonary embolism documented with ventilation and perfusion
Five patients (nos. 3, 6, 9, 11, and 14) had spontaneous
scanning. They were treated with intravenous heparin and oral
abortions (Table 4). Patients 3 and 6 had 3 first-trimester abortions,
warfarin with a target international normalized ratio of greater than
patient 11 had 2 first-trimester abortions, patient 9 had 2 second-
3.0. All patients recovered with no problems. One patient (no. 2)
trimester abortions, and patient 14 had a third-trimester stillbirth.
was admitted with blurred vision in the left eye, and retinal vein
Three patients (nos. 3, 11, and 12) fulfilled the criteria for SLE
thrombosis was found on retinal angiography. He recovered with
Figure 1. Thrombosis-free survival analysis of ITP patients by APA, LA, and ACA status. Thrombosis-free survival analysis of APA-positive and APA-negative (A), LA-positive and LA-negative (B), and ACA-positive (greater than 10 GPL/MPL) and ACA-negative (C) patients by the Kaplan-Meier method. Patients were censored for thrombosis. P values were calculated with the log-rank test. The data show that APA positivity, especially LA positivity, is an important risk factor for the development of thrombotic complications in patients who present with ITP. Table 3. Features of APA-positive patients Discussion
The mechanism of thrombocytopenia in patients with APS is
debated. It has been suggested that platelet-specific antibodies,
rather than APAs, play a role in the pathogenesis of thrombocytope-
nia in APS. In one study, antibodies directed against the GPIIb-IIIa
or GPIb-IX-V complexes were found in about 40% of the patients
with APS who had thrombocytopenia.11 Another study showed that
anti-GP antibodies are rare in patients with SLE and APS with
normal platelet counts.2,3 Anti-GP antibodies in thrombocytopenic
patients with APS do not cross-react with antibodies against
phospholipids or 2 GP-I.12 Immunosuppressive treatment of
thrombocytopenia in patients with APS increases the platelet count
and reduces the titers of anti-GP antibodies, but not the titers of
APAs.5 These data suggest that thrombocytopenia is a secondary
immune phenomenon that may develop at the same time as APS.
On the other hand, Fabris et al13 showed that platelet antigens in
thrombocytopenic patients with APS were different from those
in ITP, and surface GPs were not involved. They also found that
a 50- to 70-kd internal platelet protein had been specifically
found in patients with APS and thrombocytopenia, but not in
Whether thrombocytopenia in patients with APS is related to
Abbreviations are explained in Table 1. *APA-positive and APS-positive patients.
APAs or not, another critical issue is the clinical importance of the
†APA-positive and APS-negative patients.
presence of APAs in patients who present only with thrombocytope-nia. In this study, we investigated the frequency of APAs in patients
Group B consisted of 17 ITP patients with APA positivity who
with ITP, and we found that more than one third of these patients
did not subsequently develop APS (Table 1). Their median age was
(37.8%) had APAs at the time of diagnosis, a finding consistent
30 years (range, 16-66 years), and median follow-up was 35
with other reports.4,5 Although many researchers have suggested
months (range, 9-72 months). Seven patients had LA positivity
that APA positivity is not correlated with the development of APS
(41.1%), and 15 (88.2%) were found to be positive for ACA IgG,
in patients with ITP,5,7 there are case reports on the development of
IgM, or both (Table 3). Neither thrombotic events nor recurrent
APS in patients who initially presented with ITP.14 In this study, we
fetal losses were observed in group-B patients.
found that 14 of 31 patients (45.1%) who were persistently positive
There were no differences between the APA-positive patients
for APAs developed APS in the follow-up period. When we
with or without APS for the initial platelet counts, response to the
evaluated APA-positive and APA-negative ITP patients for throm-
therapy, or ACA IgG or IgM positivity. Although there was a trend
botic events, we found that thrombosis-free survival at 5 years was
toward a decreased complete-remission rate with methylpred-
nisolone therapy in group-A patients, the statistical analysis
What are the predictors for the development of APS in
showed no difference between the groups. On the other hand, the
APA-positive patients who present with ITP? To answer this
prevalence of LA positivity was found to be significantly higher in
question, we compared the APA-positive ITP patients with APS
group-A patients (2: P Ͻ .0036; RR ϭ 7.15; 95% CI, 1-47.6).
(group A) and those without APS (group B). During the follow-up
Table 4. Clinical and laboratory findings of ITP-onset APS (group A) patients
G indicates gender; IPC, initial platelet count; TFE, timing of first APS event (the time between ITP diagnosis and occurrence of the first thrombotic or obstetric event); DVT,
deep vein thrombosis; RVT, retinal vein thrombosis; FL, fetal loss; SLE, systemic lupus erythematosus; PE, pulmonary embolism; MesO, mesenteric artery occlusion; NA,not available.
BLOOD, 15 SEPTEMBER 2001 ⅐ VOLUME 98, NUMBER 6
period, 6 of our patients experienced venous thrombosis (5 had
nisolone therapy or splenectomy in ITP patients with persistent
deep vein thrombosis and pulmonary embolism; one had retinal
APA positivity. These data are consistent with the suggestion that
vein thrombosis), 5 had arterial thrombosis (4 had stroke; one had
severe thrombocytopenia might be a protective factor for the
mesentery artery thrombosis), and 3 patients had recurrent fetal
development of thrombosis in APS.1 Prospective studies are
losses (group A). Additionally, 3 patients in this group fulfilled the
needed to determine whether low-dose aspirin or other drugs have a
classification criteria for SLE in the follow-up period (Table 3).
prophylactic effect on thrombosis in these patients.
Group B comprised patients without recurrent fetal losses or
In conclusion, we propose that measurement of APAs, espe-
thrombotic events. We found no differences between these groups
cially LA, in patients with an initial diagnosis of ITP may identify a
regarding age, initial platelet counts, ACA IgG and IgM levels, or
subgroup of patients with a high risk of developing APS features
response to the methylprednisolone therapy. On the other hand, we
(ie, thrombosis or fetal loss). The episodic nature of the clinical
found a significantly higher prevalence of LA positivity in group-A
complications of APS, compared with the gradual development of
patients (2: P Ͻ .0036; RR ϭ 7.15; 95% CI, 1-47.6). Our data
other autoimmune diseases such as SLE, warrants a need for a
demonstrate that persistent positivity for LA is an important risk
serologic workup rather than clinical follow-up. A prophylactic
factor for the development of APS in patients who present with ITP.
drug regimen may avoid the potential complications of APS in
Further studies are required to definitively establish the RRs for LA
patients with ITP and positive LA, considering the high correlation
between LA positivity and thrombosis. Future research may
The relation between LA positivity and high risk of thrombosis
determine other markers, including genetic factors, that may help
has been demonstrated by several groups.15,16 It has been reported
that the prevalence of thrombocytopenia is higher in LA-positivepatients,17 which may suggest an association between thrombocyto-penia and thrombosis in LA-positive patients.
Eleven ITP patients in our study experienced thrombosis (6
Acknowledgments
patients had venous thromboembolism and 5 had arterial thrombo-sis). We noticed that thrombotic complications mostly developed
We are grateful to Dr Jose´ A. Lo´pez (Baylor College of Medicine,
after the platelet counts had exceeded 100 ϫ 109/L after methylpred-
Houston, TX) for his kind help in reviewing the manuscript. References
1. Galli M, Finazzi G, Barbui T. Thrombocytopenia in
7. George JN, Woolf SH, Raskob GE, et al. Idio-
thrombocytopenia. Eur J Haematol. 1998;60:283-
the antiphospholipid syndrome. Br J Haematol.
pathic thrombocytopenic purpura: a practice
guideline developed by explicit methods for the
13. Fabris F, Steffan A, Cordiano I, et al. Specific anti-
2. Godeau B, Piette JC, Fromont P, Intrator L,
American Society of Hematology. Blood. 1996;88:
platelet autoantibodies in patients with antiphos-
Schaeffer A, Bierling A. Specific antiplatelet gly-
pholipid antibodies and thrombocytopenia. Eur J
coprotein autoantibodies are associated with the
8. Wilson WA, Gharavi AE, Koike T, et al. Interna-
thrombocytopenia of primary antiphospholipid
tional consensus statement on preliminary classi-
syndrome. Br J Haematol. 1997;98:873-879.
fication criteria for definite antiphospholipid syn-
14. Moccia F. Two cases of autoimmune thrombocy-
3. Macchi L, Rispal P, Clofent-Sanchez G, et al. An-
drome. Arthritis Rheum. 1999;42:1309-1311.
topenic purpura associated with antiphospholipid
tiplatelet antibodies in patients with systemic lu-
antibodies. Ann Ital Med Int. 1999;14:114-117.
9. Harris EN, Phil M. The second international anti-
pus erythematosus and the primary antiphospho-
cardiolipin standardization workshop. The King-
15. Horbach DA, Oort EV, Donders RCJM, Derksen
lipid antibody syndrome: their relationship with
ston Anti-Phospholipid Antibody Study (KAPS)
RHWM, de Groot PG. Lupus anticoagulant is the
the observed thrombocytopenia. Br J Haema-
group. Am J Clin Pathol. 1990;94:476-484.
strongest risk factor for both venous and arterial
thrombosis in patients with systemic lupus ery-
10. Brandt JT, Triplett DA, Alving B, Scharrer I. Crite-
4. Harris EN, Gharavi AE, Hedge U, et al. Anticar-
thematosus. Thromb Haemost. 1996;76:916-924.
ria for the diagnosis of lupus anticoagulants: an
diolipin antibodies in autoimmune thrombocyto-
update. Thromb Haemost. 1995;74:1185-1188.
penic purpura. Br J Haematol. 1985;59:231-234.
16. Ginsberg JS, Wells PS, Brill-Edwards P, et al. An-
tiphospholipid antibodies and venous thrombo-
5. Stasi R, Stipa E, Oliva F, et al. Prevalence and
11. Galli M, Daldossi M, Barbui T Anti-glycoprotein
clinical significance of elevated antiphospholipid
Ib/IX and IIb/IIIa antibodies in patients with an-
antibodies in patients with idiopathic thrombocy-
tiphospholipid antibodies. Thromb Haemost.
17. Galli M, Finazzi G, Marziali S, Marchioli R, Barbui
topenic purpura. Blood. 1994;84:4203-4207.
T. The risk of thrombosis in patients with lupus
6. Stasi R, Stipa E, Masi M, et al. Long-term obser-
12. Lipp E, von Felten A, Sax H, Muller D, Berchtold
anticoagulants is predicted by their specific co-
vation of 208 adults with chronic thrombocytope-
P. Antibodies against platelet glycoproteins and
agulation profile. Thromb Haemost. 1999;81:695-
nic purpura. Am J Med. 1995;98:436-442.
antiphospholipid antibodies in autoimmune
LIFT OFF to BUSINESS, LIFT OFF to CERTIFICATE, LIFT OFF to CONVERSATION Tip Type of activity: Reading for gist; reading for detail. Teacher's needs: 1. OHP transparency of photo, (Download 1). If no OHP available, make enough photocopies to distribute among the class working in groups of four. 2. Blank OHP transparency and suitable pen. 3. OHP of the article (Download 2). If
 BLOOD, 15 SEPTEMBER 2001 ⅐ VOLUME 98, NUMBER 6
Table 2. Thrombosis-free survival analysis of the patients by Kaplan-Meier procedure
BLOOD, 15 SEPTEMBER 2001 ⅐ VOLUME 98, NUMBER 6
Table 2. Thrombosis-free survival analysis of the patients by Kaplan-Meier procedure