Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Litormed.com.br
Annals of Surgical Oncology, 10(9):1059–1069
Combined Resection and Radiofrequency Ablation for Advanced
Hepatic Malignancies: Results in 172 Patients
Timothy M. Pawlik, MD, MPH, Francesco Izzo, MD, Deborah S. Cohen, MS,
Jeffery S. Morris, PhD, and Steven A. Curley, MD
Background: Resection combined with radiofrequency ablation (RFA) is a novel approach in
patients who are otherwise unresectable. The objective of this study was to investigate the safety andefficacy of hepatic resection combined with RFA. Methods: Patients with multifocal hepatic malignancies were treated with surgical resection
combined with RFA. All patients were followed prospectively to assess complications, treatmentresponse, and recurrence. Results: Seven hundred thirty seven tumors in 172 patients were treated (124 with colorectal
metastases; 48 with noncolorectal metastases). RFA was used to treat 350 tumors. Combinedmodality treatment was well tolerated with low operative times and minimal blood loss. Thepostoperative complication rate was 19.8% with a mortality rate of 2.3%. At a median follow-up of21.3 months, tumors had recurred in 98 patients (56.9%). Failure at the RFA site was uncommon(2.3%). A combined total number of tumors treated with resection and RFA Ͼ10 was associatedwith a faster time to recurrence (P ϭ .02). The median actuarial survival time was 45.5 months. Patients with noncolorectal metastases and those with less operative blood loss had an improvedsurvival (P ϭ .03 and P ϭ .04, respectively), whereas radiofrequency ablating a lesion Ͼ3 cmadversely impacted survival (HR ϭ 1.85, P ϭ .04). Conclusions: Resection combined with RFA provides a surgical option to a group of patients
with liver metastases who traditionally are unresectable, and may increase long-term survival. Key Words: Hepatocellular cancer—Liver metastases—Resection—Radiofrequency ablation.
Patients with primary and secondary malignancies of
their liver and a significant subset of these patients has
the liver are extremely common. Worldwide, hepatocel-
isolated hepatic disease (20%).2 Although less frequent,
lular carcinoma (HCC) is one of the most widespread
other solid malignancies, such as neuroendocrine, breast,
solid cancers, with an estimated incidence of at least one
and sarcoma, can also metastasize solely to the liver.
million new patients per year.1 In the United States,
Surgical resection of primary and metastatic liver tumors
colorectal cancer represents the third most common type
is considered to be the optimal treatment modality with a
of cancer for both men and women, with an annual
curative effect, offering a 5-year survival rate between
incidence of 130,000 new cases. A majority of these
20% and 35%.3–5 Despite this, surgical extirpation is
patients develop secondary metastatic disease within
seldom undertaken. The majority of patients with pri-mary or metastatic malignancies confined to the liver are
Received March 7, 2003; accepted July 11, 2003.
not candidates for curative resection because of tumor
From the Departments of Surgery (TMP, SAC) and Biostatistics
location, multifocality, proximity of tumor to vessels, or
(DSC, JSM), The University of Texas, M.D. Anderson Cancer Center,
inadequate functional hepatic reserve. In fact, only 5% to
Houston, Texas; and the Department of Surgery (FI), The G. PascaleNational Cancer Institute, Naples, Italy.
15% of newly diagnosed primary or secondary liver
Address correspondence and reprint requests to: Steven A. Curley,
malignancies are amenable to surgical resection.6,7 In an
MD, The University of Texas MD Anderson Cancer, Department ofSurgical Oncology, Box 444, 1515 Holcombe Blvd, Houston, TX
attempt to provide treatment for the overwhelming ma-
77030; Fax: 713-745-5235; E-mail: [email protected].
jority of patients who are not candidates for isolated
Published by Lippincott Williams & Wilkins 2003 The Society of Surgical
hepatic resection, novel treatment approaches to control
and potentially cure primary and secondary liver disease
reserve inadequate to tolerate major hepatic resection. In
all cases, the intent of the surgical procedure could not
Radiofrequency ablation (RFA) has become a widely
have been curative had it not been associated with RFA.
used ablative technique for primary and secondary liver
Patients were considered for RFA even if they had tumor
tumors. RFA involves the localized application of ther-
abutting a major portal or hepatic vein branch or the
mal energy to destroy tumor cells. Alternating electric
inferior vena cava, but they were excluded if tumor
current in the range of radiofrequency (RF) waves (460
involved the main right or left bile duct (or both) because
kHz) is applied from an RF generator through a needle
of the probability of destruction of the major bile ducts
electrode placed directly into the tumor.8 This agitates
ions in tissue surrounding the electrodes, causing local-
All patients were evaluated with a baseline history and
ized frictional heating and thermal coagulative necrosis.
physical examination; serum laboratory tests consisting
Others have shown that RFA of liver malignancies is
of a complete blood count, platelets, coagulation profile,
safe, efficacious, and has acceptable local recurrence and
hepatitis B and C virus serology (HCC patients only),
short-term survival rates.9–14 Virtually all studies to date,
renal panel, electrolytes, albumin, alanine aminotransfer-
however, have investigated RFA as an isolated, alterna-
ase, aspartate aminotransferase, gamma-glutamyl trans-
tive therapy for unresectable hepatic disease. To our
ferase, alkaline phosphatase, total bilirubin, and serum
knowledge, hepatic resection combined with simulta-
alpha-fetoprotein (AFP) or serum carcinoembryonic an-
neous RFA of unresectable secondary lesions in a large
tigen (CEA) as deemed appropriate; computed tomogra-
series of patients has not been reported.
phy (CT) or magnetic resonance imaging (MRI) scan of
Combining hepatic resection with RFA allows the
the abdomen and pelvis; and a chest radiograph. Patients
surgeon to remove the bulk of disease or larger tumors
were excluded for combined modality treatment if their
while ablating any residual smaller lesions. By combin-
platelet count was Ͻ40,000/L or if the prothrombin
ing techniques, more patients may become candidates for
time was prolonged more than 1.5 times above normal.
hepatic resection, as any remaining “unresectable” tu-
However, if platelet or fresh-frozen plasma transfusions
mors can be ablated while still preserving an adequate
corrected the abnormal laboratory values to meet these
volume of perfused functional liver. Although conceptu-
criteria, the patient received treatment. Those patients
ally appealing, there is presently little empirical data to
with a white blood count below 2,000 or a bilirubin Ͼ2.0
support the use of this combination of therapy. In this
study, we review a large cohort of patients who under-
All patients were treated surgically with both resection
went combined multimodality treatment consisting of
and RFA during one operation. Upon entering the abdo-
hepatic resection with RFA of additional lesions for the
men, an initial exploration was performed to preclude the
treatment of primary or secondary hepatic malignancies.
presence of extrahepatic disease. An intraoperative he-
The objective of this study was to investigate and eluci-
patic ultrasound was then performed to identify, count,
date the feasibility, safety, and potential efficacy of he-
and characterize the nature and vascular proximity of the
hepatic lesions. Routinely, the hepatic resection was per-formed first. The location of the hepatic lesion and its
MATERIALS AND METHODS
relation to surrounding vascular and biliary structuresdictated whether or not a formal anatomic resection was
Between January 1996 and April 2002, a series of 172
performed. In general, hepatic resection was performed
patients underwent combined hepatic resection with in-
using a stapling technique as previously described.15
traoperative RFA. All patients with histologically con-
After removal of the index lesion(s), the remaining un-
firmed primary or metastatic hepatic malignancies with
resectable lesions were treated with RFA after a stan-
no clinical, radiographic, or intraoperative evidence of
dardized treatment algorithm.16,17 Intraoperative ultra-
extrahepatic disease were eligible for combined treat-
sonography was used to place the RF needle into the
ment. To be eligible, patients had to have multifocal
lesions to be treated by RFA. RFA was administered
hepatic disease that was deemed unresectable by classic
using the RF 2000 or 3000 generator system (Boston
standards due to either the location of the disease or the
Scientific Corp, Natick, MA), a LeVeen monopolar nee-
volume of liver involved. Patients were deemed surgi-
dle electrode (4.0-cm maximum array diameter), and
cally unresectable for cure based on the number or bilo-
four indifferent dispersive grounding pads applied to the
bar location of tumors, tumor proximity to major vascu-
patient’s skin. The RF 2000 system consists of a gener-
lar structures precluding a margin-negative resection,
ator that supplies up to 100 W of power, whereas the RF
and/or the presence of cirrhosis with a functional hepatic
3000 provides up to 200 W of power. The LeVeen needle
Ann Surg Oncol, Vol. 10, No. 9, 2003MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIES
electrode is a 15-gauge, 12- to 15-long insulated cannula
these patients are shown in Table 1. Combined hepatic
that contains 10 to 12 individual hook-shaped electrode
resection and RFA was used to treat metastatic colorectal
arms that are deployed in situ. For tumors Ͻ2.5 cm in
cancer in the overwhelming majority of cases: 124 pa-
diameter, the multiple array was deployed into the center
tients (72.1%). Metastatic leiomyosarcoma was the sec-
of the tumor. For larger lesions, the array was first
ond most commonly treated lesion (n ϭ 13, 7.6%),
deployed at the most posterior interface (ultrasono-
whereas only 5 patients (2.9%) had multifocal HCC.
graphically) between tumor and normal liver parenchy-
Other more uncommon lesions included metastatic car-
ma; it was subsequently withdrawn and redeployed at
cinoid, pancreatic cancer, neuroendocrine tumors, breast
1.5-cm intervals in the tumor. Each tumor or area within
metastases, cholangiocarcinoma, and one patient with
a large tumor was treated with a two-phase application of
ocular melanoma. This latter group of patients, however,
RF power before retracting the multiple array and repo-
only accounted for 17.6% of the total patients treated and
sitioning or removing the needle electrode. The electrode
represents a highly selected cohort of patients. The com-
was optimally positioned to achieve complete destruc-
mon factor in these patients with noncolorectal liver
tion of tumor and at least a 1-cm zone of normal liver
metastases was liver-only disease confirmed on multiple
imaging studies that was responding or stable on suitable
After hepatic resection and tumor ablation, the same
battery of serum blood tests as had been drawn preoper-
Resection combined with RFA was used to treat 737
atively were again obtained postoperatively on days 1, 7,
tumors. A total of 387 tumors were treated with hepatic
and 30. At 1 month and every 3 months up to 2 years
resection, whereas 350 tumors underwent RFA. The me-
after treatment, and then every 6 months thereafter, a CT
dian number of tumors per patient was 3 (range, 2–21);
or MRI scan of the abdomen, a chest radiograph, and
the median number of tumors surgically excised per
serum laboratory tests were obtained.
patient was 2 (range, 1–9), and the median number of
For purposes of this study, the following were col-
tumors ablated was 1 (range, 1–12). Surgery involved
lected for all patients: patient age and sex; tumor histol-
resection of a single tumor in 81 patients (47.1%), two
ogy, number, location, and size; type of surgical resec-
tumors in 30 patients (17.4%), three tumors in 31 pa-
tion; operative details; disease status; follow-up date;
tients (18.1%), and more than three in 30 patients
death date; and complication data. Disease status was
(17.4%) (Table 2). In performing the hepatic resection,
classified as no evidence of disease (NED), alive with
the type of procedure employed varied widely (Table 3).
disease (AWD), dead of disease (DOD), or dead of other
The majority of patients (n ϭ 101, 58.7%) had a resec-
causes at last known follow-up. Recurrences were de-
tion that involved the removal of at least 2 hepatic
tected by CT/MRI imaging or via biopsy diagnosis and
segments and a full one-half of the patients underwent at
were defined as tumors occurring either at local sites of
least a formal hepatic lobectomy in addition to the RFA
prior ablation, distant sites within the liver, or distant
treatment. Specifically, 31 patients (18%) underwent a
Distribution of survival time and time to progression
were analyzed in relation to the different variables col-
Characteristics of the 172 patients treated with
lected. Univariate tests (log-rank) were used to test for
differences in these distributions by any single factor.
Those factors that appeared to have significant impact on
survival or time to progression were entered into a Cox
proportional hazards model to test for significant effects
while adjusting for multiple factors simultaneously.
During the study period, a total of 172 patients were
treated using the combined modality of hepatic resection
with RFA. There were 102 men (59.9%) and 70 women
(40.1%), with a median age of 56.2 years (range, 12– 80
years). In all cases, RFA treatment and hepatic resection
were performed at The University of Texas M.D. Ander-son Cancer Center. The primary cancer diagnoses in
RFA, radiofrequency ablation; NOS, not otherwise specified. Ann Surg Oncol, Vol. 10, No. 9, 2003Patient tumor burden characteristics
the operation. The median operative time for the com-bined procedure was 3.0 hours (range, 1– 8.13 hours)
with a median blood loss of 200 cc (range, 50 –2000 cc).
Only one intraoperative RFA-associated complication
occurred: a partial thickness thermal injury to the adja-
cent stomach, which was recognized and repaired at the
time of injury; there were no long-term consequences of
The postoperative complication rate was 19.8% (34
complications occurring in 25 patients), including 4 post-
operative deaths for an overall mortality rate of 2.3%
(Table 4). A number of complications were minor and
not necessarily related to the type of procedure per-
formed. These included prolonged postoperative ileus
(2.3%), urinary tract infections (.6%), and pleural effu-
sion (.6%). Intermediate morbidity complications in-
cluded cardiac events such as tachycardia or dysrhyth-
mias (1.7%), biloma (2.3%), perihepatic abscess (1.7%),and pneumonia (2.9%). There was no correlation be-
right lobectomy, 11 patients an extended right lobectomy
tween the extent of the liver resection or number of
(6.4%), 28 patients a left lobectomy (16.3%), 14 patients
tumors treated with RFA and the development of post-
an extended left lobectomy (8.1%), and 2 patients (1.1%)
operative complications. Major complications such as
a right trisegmentectomy. Only 21 patients (12.2%) had
adult respiratory distress syndrome (.6%), multisystem
organ failure/hepatic failure (1.7%), postoperative bleed
After removal of the index lesion(s), the remaining
(.6%), and pulmonary embolus (.6%) were more uncom-
unresectable lesions were treated with RFA following a
mon and predominantly occurred in the 4 patients who
standardized treatment algorithm. RFA was used to treat
died postoperatively (Table 5). A review of the 4 post-
350 lesions: a single tumor in 97 patients (56.4%), two
operative deaths revealed that 2 deaths were related to
tumors in 34 patients (20.0%), and three or more tumors
liver failure. Patient 1 had cirrhosis and did not tolerate
in 41 patients (23.6%) (Table 2). The diameter of each
a limited resection involving the removal of hepatic
tumor was measured in three dimensions by ultrasonog-
segments V and VI. In contrast, patient 4 had normal
raphy before RFA. The median size of the lesions treated
preoperative liver function, but did not have enough
with RFA was 1.8 cm ϫ 1.6 cm ϫ 1.5 cm (range, .3 cm
hepatic reserve to tolerate an extended right lobectomy
ϫ .3 cm ϫ .3 cm to 12.0 cm ϫ 12.0 cm ϫ 5.5 cm). In
with RFA and postoperatively developed multisystem
general, adding RFA to the hepatic resection was welltolerated and added minimal complexity or morbidity to
Postoperative complications and deaths:complications (34 complications in 25 patients)
Multisystem organ failure/hepatic failure
Ann Surg Oncol, Vol. 10, No. 9, 2003MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIESPostoperative complications and deaths: postoperative deaths (n ϭ 4, 2.3%)
HCC, hepatocellular carcinoma; CRC, colorectal carcinoma metastasis; RFA, radiofrequency ablation; OR, operating room; EBL, estimated blood
loss; ARDS, adult respiratory distress syndrome; MSOF, multiple system organ failure.
organ failure. Patient 3 had a postoperative bleed result-
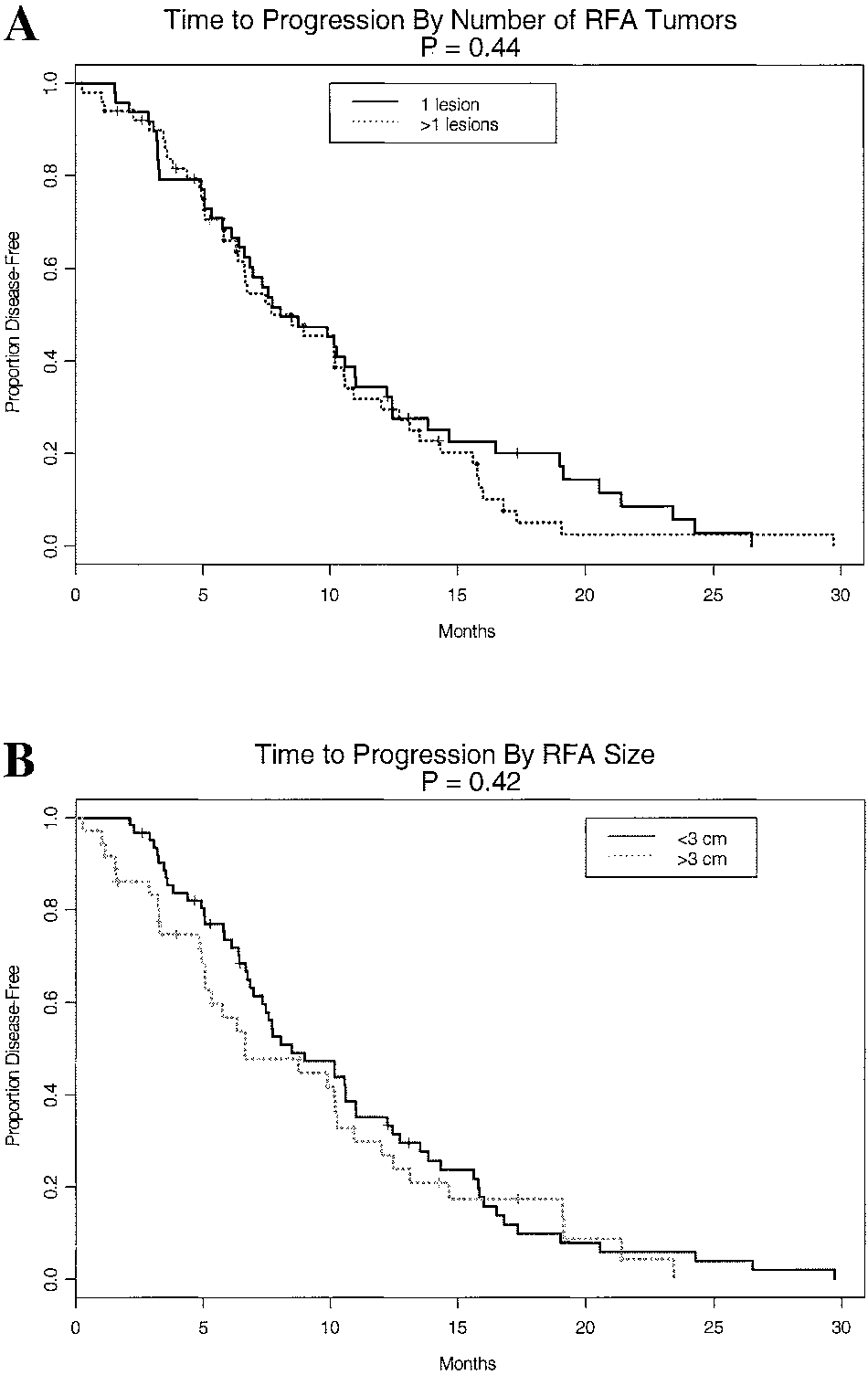
pared to those patients with fewer tumors (7.6 –10.3
months) (Fig. 1). Although the total numbers of tumors
At a median follow-up of 21.3 months, tumor had
treated seemed to impact time to recurrence, the number
and size of tumors treated with RFA did not effect
The site of first recurrence was isolated to the RFA site
median time to recurrence (P ϭ .44 and P ϭ .42, re-
in 8 patients (8.2%), a non-RFA hepatic recurrence in 38
spectively) (Fig. 2). Similarly, other factors such as age,
patients (38.8%), a non-RFA hepatic recurrence plus
type of cancer, simultaneous vs. metachronous metasta-
distant disease in 31 patients (31.6%), and isolated dis-
ses, and type of resection all did not impact time to
tant disease in 21 patients (21.4%). Interestingly, the
recurrence on univariate analysis (all P Ͼ .05). In all
median time to failure was about 7.5 months in all cases
cases, the median time to recurrence was Ͻ12 months,
(Table 6). Not unexpectedly, the most common site of
suggesting that the majority of patients who do recur will
distant disease was pulmonary metastases. A detailed
do so within a short period of time after surgery.
review of the 8 patients with RFA site recurrences re-
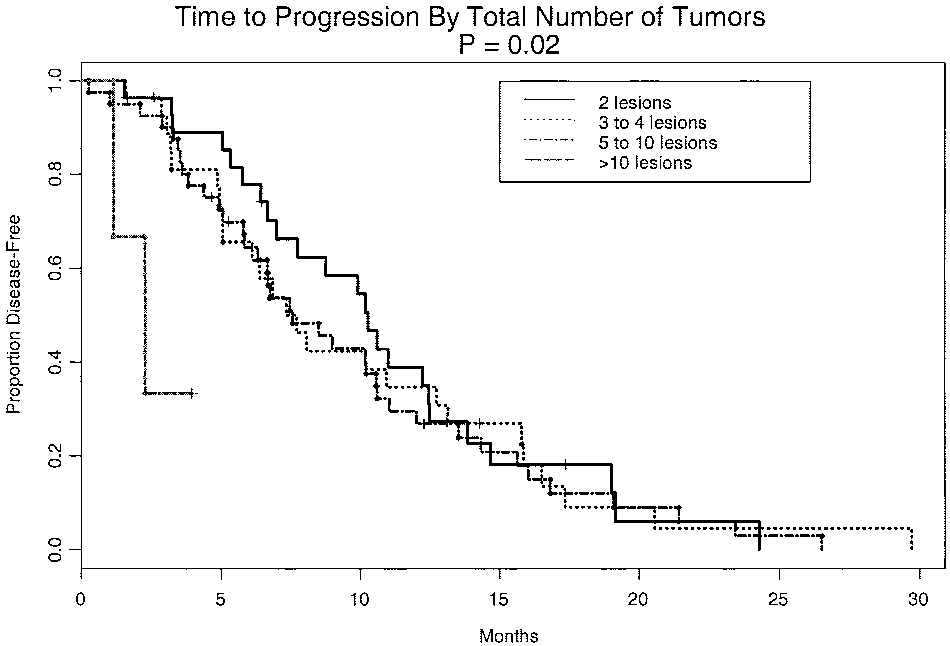
On multivariate analysis, the total number of tumors
vealed that 4 patients had lesions ablated that were Ն 3
was again the only significant variable that affected time
cm (Table 7). One patient had a 12-cm lesion treated
to recurrence. Those patients who had more than 10
with RFA but recurred Ͻ2 months postoperatively. It is
tumors treated with combined hepatic resection and RFA
important to note that although 8 patients out of 172
were significantly more likely to have a shorter time to
recurred at the RFA site for an overall patient failure rate
recurrence than those with less disease (HR ϭ 1.63, CI ϭ
of 8.2%, there were only 8 treatment site failures out of
With regard to survival, at last follow-up 60 patients
Univariate analysis was performed to detect which
(34.8%) had died of disease, whereas 112 patients
factors possibly had an effect on the time to recurrence.
(65.2%) were still alive. The overall median actuarial
As shown in Table 8, the only factor that affected time to
survival time was 45.5 months. Univariate analysis re-
recurrence was the total number of tumors treated (i.e.,
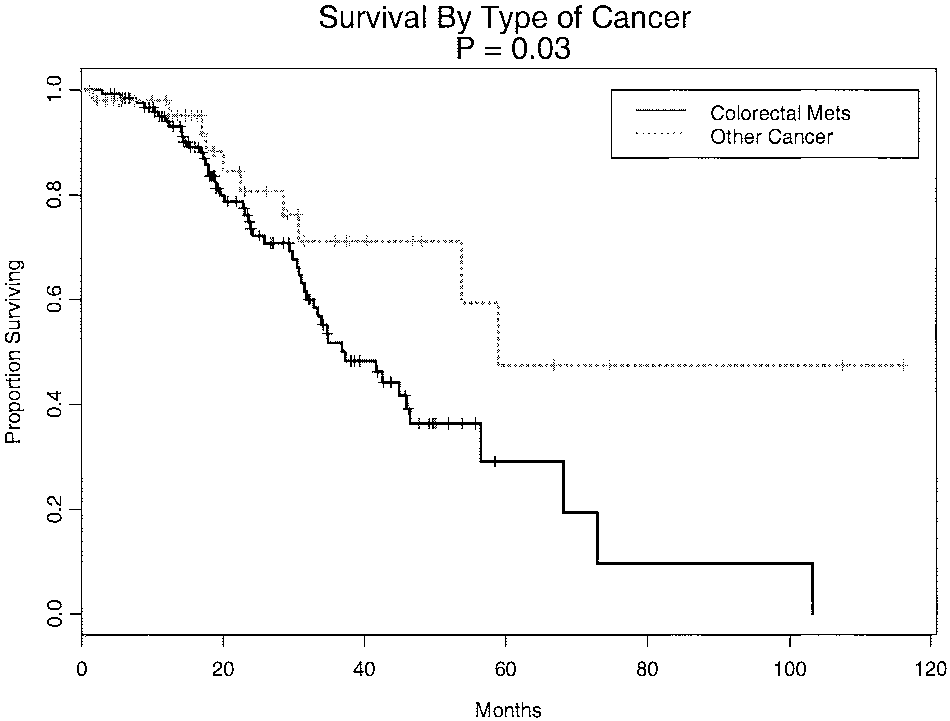
vealed that the type of cancer as well as the amount of
the total number of tumors surgically resected plus those
blood loss were significant factors affecting overall sur-
treated with RFA). When tested in a four-category sys-
vival. Those patients with noncolorectal metastases had a
tem, there was a statistically significant difference in the
significantly better median survival (59 months) as com-
time to recurrence in those patients who had more than
pared to those patients with colorectal metastases (37.3
10 tumors treated (P ϭ .02). These patients had a shorter
months) (P ϭ .03) (Fig. 3). The amount of surgical blood
median disease-free survival time (2.3 months) as com-
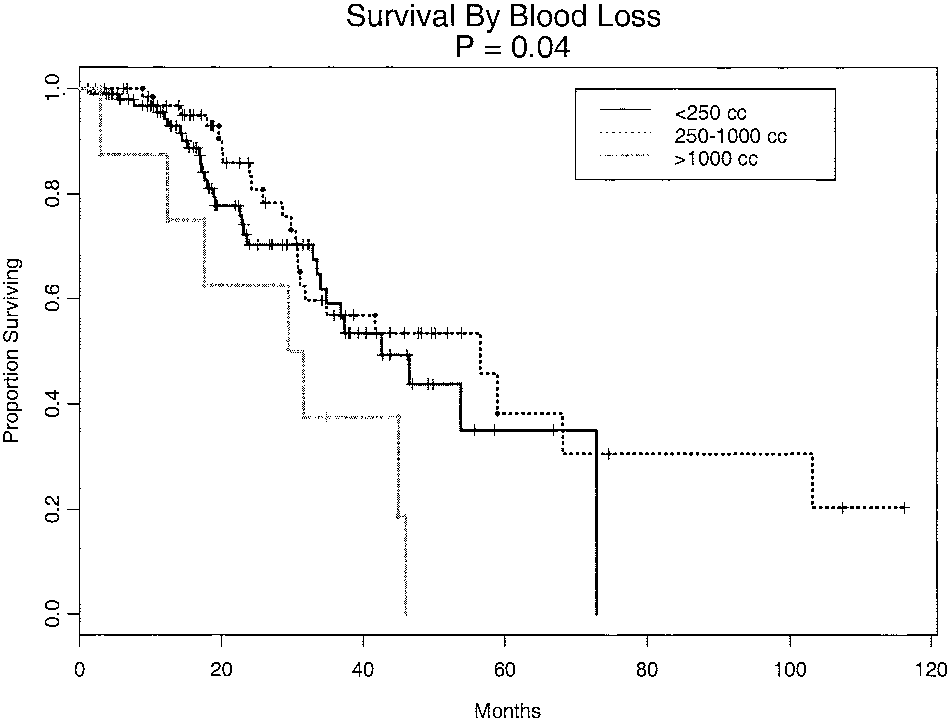
loss also significantly affected overall survival. Patientswith Ͼ 1000 cc blood loss had a median survival of 30.5
Details of tumor recurrence after hepatic
months as compared to 42.6 months and 56.6 months for
resection and RFA: overall recurrence rates
patients with Ͻ250 cc and 250 to 1000 cc blood loss,
respectively (P ϭ .04). The effect of blood loss on
survival was not seen in the immediate postoperative
period but rather became more evident in long-term
follow-up (Fig. 4). Although not statistically significant,
those patients who had RFA of a lesion Ͼ3 cm showed
a trend toward worse survival (P ϭ .14). Other factors
such as age, number of RFA tumors, type of surgery, and
total number of tumors treated did not significantly affect
survival on univariate analysis (all P Ͼ .05). Ann Surg Oncol, Vol. 10, No. 9, 2003Details of tumor recurrence after hepatic resection and RFA: recurrence at the RFA site
As colorectal cancer is the major type of hepatic
On multivariate survival analysis, the size of the RFA
metastasis confronting surgeons in the United States, we
lesion was the only factor that significantly impacted
felt it important to analyze this group separately. As
survival. Patients who underwent RFA of a lesion Ͼ3 cm
noted above, those patients with colorectal metastases
had a higher likelihood of death than those who under-
had a median actuarial survival of 37.3 months. Addi-
went RFA of a lesion Յ3 cm (HR ϭ 1.85, CI ϭ 1.02–
tional analysis revealed that patients with synchronous
3.37, P ϭ .04). Similar to univariate analysis, there was
colorectal metastasis had a better overall survival as
a trend suggesting that patients with synchronous hepatic
compared to patients with metachronous metastases
metastases did better than those patients with metachro-
nous lesions (HR ϭ .64, CI ϭ .36 –1.14, P ϭ .13). Univariate analysis of factors affecting timeDISCUSSION
Primary and secondary malignancies of the liver are
extremely common. The liver is second only to lymphnodes as the most frequent site of metastasis from other
solid cancers.2 In fact, liver failure from extensive me-
tastases often constitutes the main cause of death in
patients with both colorectal cancer as well as a number
of other common carcinomas. Surgical resection for pri-
mary and secondary hepatic malignancies is considered
Total burden of disease-treated (i.e., the total number of
tumors surgically resected plus those treated with radiofrequency ab-
lation ) impacts recurrence. Those patients with a total tumor burden of
Ͼ10 lesions treated do have a shorter median disease-free survival time
as compared to those with fewer tumors (P ϭ .02). Ann Surg Oncol, Vol. 10, No. 9, 2003MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIES
Patients with noncolorectal metastases had a significantly
better median survival (59 months) as compared with those patientswith colorectal metastases (37.3 months) (P ϭ .03).
for hepatic malignancies is critical if higher long-termsurvival rates are to be achieved. Unfortunately, mostpatients (80% to 90%) are not candidates for surgicalresection either due to extent or distribution of disease.20Traditionally, for a tumor to be considered appropriatefor resection, there must not be any extrahepatic diseaseor severe hepatic dysfunction, the tumor or tumors mustnot be so extensive that too little functioning liver re-mains after the resection, at least a 1-cm tumor-freeresection margin should be attained, and there should notbe any involvement of the confluence of the portalvein.20,21 Recent advances have led to the development
Although the total number of tumors treated seemed to
impact time to recurrence, the number (A) and the size (B) of tumors treated with radiofrequency ablation (RFA) did not affect median time to recurrence (P ϭ .44 and P ϭ .42, respectively).
the only treatment modality with potential for a curativeeffect. In selected patients with metastatic disease con-fined to the liver, reported five-year survival rates forpatients undergoing resection of secondary metastaticliver tumors range from 20% to 35%.3–5 In contrast,without any treatment, the median survival after thedetection of liver metastases is approximately 9 months,depending on the extent of the disease at the time ofdiagnosis.18 The outcomes for patients treated with sys-temic chemotherapy strongly depend on the regimenused and type and organ of origin of the cancer, butgenerally a 1-year survival rate of approximately 60% isreported, with a 2-year survival rate below 30%.19 Five-
Patients with Ͼ1000 cc blood loss had a median survival less
year survival and cure are both exceedingly rare for
than that of patients who had Ͻ250 cc and 250 to 1000 cc blood loss(P ϭ .04). Effect of blood loss on survival was not seen in the
patients with hepatic metastases treated with chemother-
immediate postoperative period but rather became evident in long-term
apy alone. Given this, the availability of surgical therapy
Ann Surg Oncol, Vol. 10, No. 9, 2003
of several alternative treatment methods designed to pro-
a population of patients who have a larger tumor burden
vide therapy for the majority of patients diagnosed with
associated with biologically more aggressive disease and
liver cancer who are not candidates for surgical
an inherently poorer prognosis. Performing a potentially
morbid procedure (such as a resection with RFA) would
Interstitial local ablative techniques involving either
be unwarranted if it could not lead to meaningful long-
freezing (cryoablation),22,23 chemical desiccation (alco-
term survival in a subset of patients. In reviewing the
hol ablation),24,25 or RFA9,26,27 have all been described.
literature, there have been occasional reports of RFA
Among these, rapid freezing of tissue with exposure to
being used as an adjunct to resection, but these studies
liquid nitrogen cryoprobes at 196°C has a high risk of
have included only small numbers of patients.40,41 The
liver fracture, hemorrhage, and tumor-lysis syndromes,
current study represents the largest series of patients
whereas alcohol injection results in nonhomogeneous dis-
reported to date who have been treated simultaneously
tribution within tumors and results in incomplete areas of
necrosis.28 Neither of these local therapies produces ex-
This study was performed to address the question of
tended long-term survival in most patients.29–33 In contrast,
feasibility and safety concerning the use of combined
isolated RFA of unresectable liver malignancies has been
hepatic resection and RFA applications. As other studies
shown to be safe and efficacious; however, local recurrence
have reported, intraoperative complications from RFA
rates ranging from 5% to 30% have been reported.9–14
are uncommon.9,17,40,41 In the current series, there was
In general, most data concerning RFA treatment of
only one intraoperative complication: a partial thickness
hepatic tumors has come from studies involving patients
thermal injury to the stomach that resulted in no long-
with unresectable disease who have had RFA as primary
term consequences. The complication rate for hepatic
therapy. In these studies, RFA has proven to be an
resection and RFA was 19.8%, which is comparable to
extremely safe procedure with a complication rate lower
the 11% to 35% morbidity rates reported for hepatic
than 10%.9,10 Previous studies using both imaging stud-
resection alone.42,43 Most of the complications were mi-
ies and pathological evaluation of ablated lesions have
nor or intermediate, including urinary tract infections,
shown complete tumor eradication.34–37 Recent studies
bilomas, or abscesses that were amenable to percutane-
with isolated RFA show a median survival of 34 months
ous drainage. Serious complications were less common,
and a 3-year survival rate of 36% from the time of
but when they did occur they were strongly associated
thermal ablation.38,39 Recurrence rates at the RFA site
with mortality. Overall the perioperative mortality rate
have been reported to be Ͻ10% after surgical RFA, with
was 2.3%, which again compares favorably to reported
most treatment failures occurring in larger tumors (Ͼ3– 4
rates of 0% to 3% for hepatic resection alone.42,43 It
cm in diameter).9,10,13,40 One explanation for local RFA
appears, therefore, that hepatic resection combined with
site failure in 4 of the 8 patients in the present study is the
RFA is safe and well tolerated. A review of the periopera-
large size of the ablated lesion with a corresponding
tive deaths, however, mandates a cautionary note. Two
inadequate tumor kill. Local RFA failure, however,
deaths were associated with liver failure, subsequent mul-
could not be completely attributed to the size of the
tisystem organ failure and death. These patients serve to
lesion ablated as the other 4 patients had tumors Յ3 cm.
emphasize that although combined therapy appears to be
We do not advocate use of RFA as a replacement for
safe in the majority of cases, resection combined with
resection, which remains the gold standard for the treat-
thermal destruction of too great a volume of liver may lead
ment of malignant liver tumors. Rather, RFA has been
to liver failure and death. Patients with cirrhosis and pre-
advocated as a treatment solely for those tumors that are
operative hepatic compromise, as well as those patients
unresectable by virtue of their number, location, or size
with normal liver function but in whom an extended resec-
relative to liver volume. At the University of Texas M.D.
tion combined with RFA is being considered must be care-
Anderson Cancer Center, in an attempt to increase the
fully evaluated to determine if an adequate volume of
number of patients who are eligible for aggressive sur-
perfused normal liver will remain after resection and RFA.
gical removal or destruction of tumors, we now perform
In general, adding RFA to the hepatic resection was
RFA in combination with hepatic resection. Despite the
well tolerated and added minimal complexity to the
theoretical appeal of combination therapy, there is some
operation. In the majority of cases, the operation in-
concern in the surgical community that the addition of an
volved a formal hepatic lobectomy plus RFA. Despite
ablative therapy to a major hepatic resection would be
this, the median operative time was only 3 hours and the
unsafe and add significant complexity to an already
median blood loss was only 200 cc. These numbers are
demanding operation. Additionally, there is concern that
comparable to historical operative data of isolated hepatic
patients with traditionally unresectable disease represent
resection performed at our institution. On univariate anal-
Ann Surg Oncol, Vol. 10, No. 9, 2003MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIES
ysis, the amount of blood loss did seem to affect overall
study, multivariate analysis revealed that a total number
survival with patients experiencing Ͼ 1000 cc blood loss
of tumors Ͼ10 was significantly associated with a short
having a significantly decreased median survival. One pos-
time to recurrence (Ͻ3.0 months). Patients with Ͼ10
sible reason for this is that blood loss may have acted as a
tumors clearly represent a cohort of patients with a
surrogate marker for not only the complexity of the surgical
significant tumor burden who may be more likely to
resection, but also the extent of hepatic disease.
harbor micrometastatic disease. Based on our data, we
The patients in the present study had a wide spectrum
would recommend caution in offering combined modal-
of tumors, with the majority having colorectal metasta-
ity therapy to this subset of patients, as a meaningful
ses. The study did include patients with other secondary
malignancies of the liver such as leiomyosarcoma, breast
At last follow-up, 65.2% of patients were alive, yield-
cancer, pancreatic cancer, and neuroendocrine tumors.
ing a median actuarial survival time of 45.5 months.
This latter group represented a minority of the patients
Three factors seemed to affect overall survival. As noted
treated with resection and RFA. Previously studies have
above, patients with noncolorectal metastasis and those
shown that RFA for noncolorectal hepatic metastases can
with Ͻ1000 cc blood loss had a significantly greater
be effective if the patient population is chosen careful-
probability of long-term survival. RFA of a tumor Ͼ3 cm
ly.9,40,44 In the present study, on univariate analysis,
in diameter was a significant factor on multivariate anal-
those patients with noncolorectal metastases had a sta-
ysis with these patients having a higher likelihood of
tistically significant better median survival as compared
death from cancer recurrence than those who underwent
to those patients with colorectal metastases. This may be
ablation of a lesion Յ3 cm (HR ϭ 1.85, CI ϭ 1.02–3.37,
related to selection bias. The therapeutic threshold for
P ϭ .04). Previous studies have also shown a correlation
operating on noncolorectal hepatic metastasis is consid-
between lesion size, recurrence risk, and survival. We do
erably higher than that for colorectal disease. Most pa-
not recommend abandoning combined hepatic resection
tients with noncolorectal liver metastases have been
and RFA of lesions Ͼ 3 cm, but this data does show that
heavily pretreated with systemic or regional chemother-
there is an increased risk of failure in this subset of
apy and have been followed for a period of time in order
patients. This may be because RFA of lesions Ͼ3 cm in
to document stable isolated hepatic disease. In contrast,
diameter requires more experience and creation of mul-
colorectal patients are more likely to undergo resection
tiple overlapping zones of thermal necrosis is usually
sooner, without a period of time to monitor the stability
required. For this reason, hepatic resection combined
of their disease. Thus, colorectal patients may be more
with RFA should be performed by those who have ex-
likely to harbor unsuspected regional or distant micro-
pertise in both techniques. Due to the inherent learning
metastatic disease that becomes clinically evident
curve associated with RFA, one should initially attempt
months or years after an operation. Our data supports the
ablation of smaller lesions before undertaking more com-
safety of an appropriately aggressive treatment plan for
plex larger lesions. Furthermore, clinical trials of adju-
patients with both colorectal and noncolorectal hepatic
vant systemic and/or regional therapies following resec-
metastasis. In patients with stable isolated noncolorectal
tion and RFA of hepatic malignancies must be performed
hepatic metastases, hepatic resection in combination with
to assess for reduction in rates of cancer recurrence.
RFA can lead to significant long-term survival periods.
One of the most surprising outcomes of the study was
Recurrence of cancer after liver resection and RFA
the finding that patients with synchronous colorectal
occurred in 56.9% of patients. RFA site recurrence oc-
metastases seemed to enjoy a better survival than pa-
curred in 8 patients (8.2%), but local recurrence occurred
tients with metachronous lesions. Although this was
in only 8 of 350 tumors ablated (2.3%). Thus, RFA site
found to be significant in univariate analysis, in the
recurrence was uncommon with regional or distant re-
multivariate model, it did not withstand competing risk
currence being much more frequent. RFA and resection
adjustment but a trend did persist (P ϭ .13). This finding
are treatments designed to achieve local control of ma-
is at odds with traditional reports showing that patients
lignant hepatic tumors. Resection or local destruction of
with synchronous lesions tend to have a relatively poor
tumor can produce long-term disease-free and overall
survival probability. Although we do not have a clear
survival in a subset of patients but cannot overcome the
explanation for this finding in the current study, it may
tumor biology in patients who already have micrometa-
be related to patient selection and pretreatment bias. The
static disease at the time of their surgical therapy. Thus,
majority of our patients who developed metachronous
even though we had a RFA site failure rate of only 2.3%,
colorectal liver metastases did so after receiving adjuvant
recurrent disease developed in over one-half of the pa-
fluoropyrimidine-based systemic therapy after resection
tients after combined resection and RFA. In the current
of their primary colorectal cancer. Thus, they had already
Ann Surg Oncol, Vol. 10, No. 9, 2003
failed one chemotherapy regimen and had fewer subse-
NIH conference on hepatocellular carcinoma. Ann Intern Med
quent treatment options. In contrast, patients with syn-
2. Weiss L, Grundmann E, Torhorst J, et al. Hematogenous metastatic
chronous liver metastases underwent resection of their
patterns in colonic carcinoma: an analysis of 1541 necropsies.
primary cancer followed by three drug-combined sys-
temic chemotherapy (IFL: irinotecan, 5-fluorouracil, leu-
3. Fong Y, Cohen AM, Fortner JG, et al. Liver resection for colo-
rectal metastases. J Clin Oncol 1997;15:938 – 46.
covorin) both before and after liver resection and RFA.
4. Blumgart LH, Fong Y. Surgical options in the treatment of hepatic
This aggressive multimodality approach may have a
metastases from colorectal cancer. Curr Probl Surg 1995;32:333–
greater impact on patient survival probabilities; however,
5. Tuttle TM. Hepatectomy for noncolorectal liver metastases. In:
further accrual and follow-up of these patients is needed.
Curley SA, ed. Liver Cancer. New York: Springer-Verlag Publish-
Our group of 172 patients treated with combined he-
patic resection and RFA of malignant liver tumors is the
6. Liver Cancer Study Group of Japan. Primary liver cancer in Japan:
clinicopathologic features and results of surgical treatment. Ann
largest series reported to date. Other reports contain
either patients treated with RFA alone or have small
7. Nagorney DM, van Heerden JA, Ilstrup DM, Adson MA. Primary
number of patients who underwent combined modality
hepatic malignancy: surgical management and determinants ofsurvival. Surgery 1989;106:740 – 8.
treatment. In this study, we showed that concurrent treat-
8. Rhim H, Dodd GD III. Radiofrequency thermal ablation of liver
ment with surgical resection and RFA is feasible and
tumors. J Clin Ultrasound 1999;27:221–9.
safe. Local recurrence rates at RFA sites treated using
9. Curley SA, Izzo F, Delrio P, et al. Radiofrequency ablation of
unresectable primary and metastatic hepatic malignancies: results
intraoperative ultrasound-guided therapy with multiple
in 123 patients. Ann Surg 1999;230:1– 8.
overlapping zones of thermal treatment is uncommon.
10. Wood TF, Rose DM, Chung M, Allegra DP, Foshag LJ, Bilchik
Regional or distant recurrence of disease is the more
AJ. Radiofrequency ablation of 231 unresectable hepatic tumors:indications, limitations, and complications. Ann Surg Oncol 2000;
frequent pattern of failure. We demonstrated that tumor
burden influences the time to recurrence, but age, gender,
11. de Baere T, Elias D, Dromain C, et al. Radiofrequency ablation of
histological type, RFA lesion size, and the type of resec-
100 hepatic metastases with a mean follow up of more than 1 year. Am J Roentgenol 2000;175:1619 –25.
tion performed do not. At a median follow-up of 21.3
12. Solbiati L, Ierace T, Tonolino M, Orti V, Cova L. Radiofrequency
months, 65.2% of patients were still alive for a median
thermal ablation of hepatic metastases. Eur J Ultrasound 2001;13:
actuarial survival of 44.5 months. It is difficult to com-
13. Bilchik AJ, Wood TF, Allegra DP. Radiofrequency ablation of
pare objectively resection plus RFA results with other
unresectable hepatic malignancies: lessons learned. Oncologist
modalities such as RFA alone or resection alone because of
the differences in the patient populations treated. Neverthe-
14. Vogl T, Mack M, Straub R. Thermal ablation of liver metastases.
Current status and prospects. Radiologe 2001;41:49 –55.
less, our data is provocative as it suggests that even patients
15. Curley SA, Cusack JC, Tanabe KK, Stoelzing O, Ellis LM. Ad-
with multifocal, liver-only, but otherwise unresectable liver
vances in the treatment of liver tumors. Curr Probl Surg 2002;39:
cancer may derive a significant survival benefit from com-
16. Pearson AS, Izzo F, Fleming RY, et al. Intraoperative radiofre-
bined hepatic resection and RFA. The selection of such
quency ablation or cryoablation for hepatic malignancies. Am J
patients is critical and results of this nonrandomized, retro-
spective study must be corroborated by further clinical
17. Curley SA, Izzo F, Ellis LM, Vauthey J, Vallone P. Radiofre-
quency ablation of hepatocellular cancer in 110 patients with
trials. Further studies will also be needed to evaluate the
cirrhosis. Ann Surg 2000;232:381–91.
impact of combining liver resection and RFA on patient
18. Stangl R, Altendorf-Hofmann A, Charnley RM. Factors influenc-
quality of life. Moreover, although local tumor control may
ing the natural history of colorectal liver metastases. Lancet 1994;343:1405–10.
be achieved with hepatic resection and RFA, the high
19. Ruers T, Bleichrodt RP. Treatment of liver metastases, an update
propensity for these malignant liver tumors to recur region-
on the possibilities and results. Eur J Cancer 2002;38:1023–33.
ally and systemically in a significant number of patients
20. Steele G, Ravikumar T. Resection of hepatic metastases from
colorectal cancer. Biologic perspective. Ann Surg 1989;210:127–
emphasizes the need for effective multimodality approaches
to aid in the control of distant disease.
21. Adson MA, van Heerden JA, Adson MH, Wagner JS, Ilstrup DM.
Resection of hepatic metastases from colorectal cancer. Arch Surg1984;119:647–51. ACKNOWLEDGMENTS
22. Zuro LM, Staren ED. Cryosurgical ablation of unresectable hepatic
tumors. AORN-J 1996;64:231– 44.
The acknowledgments are available online at
23. Tandan VR, Harmantas A, Gallinger S. Long-term survival after
hepatic cryosurgery versus surgical resection for metastatic colo-rectal carcinoma: a critical review of the literature. Can J Surg1997;40:175– 81.
24. Ishii H, Okada S, Nose H, et al. Local recurrence of hepatocellular
REFERENCES
carcinoma after percutaneous ethanol injection. Cancer 1996;77:1792– 6.
1. Di Bisceglie A, Rustgi V, Hoffnagle J, Dusheiko GM, Lotze MT.
25. Liviraghi T, Bolondi L, Lazzaroni S, et al. Percutaneous ethanol
Ann Surg Oncol, Vol. 10, No. 9, 2003MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIES
injection in the treatment of hepatocellular carcinoma in cirrhosis.
percutaneous radio-frequency ablation with cooled-tip electrodes.
A study on 207 patients. Cancer 1992;69:925–9.
26. MaGahan JP, Schneider P, Brock JM. Treatment of liver tumors by
36. Dodd GD III, Soulen MC, Kane RA, et al. Minimally invasive
percutaneous radiofrequency electrocautery. Semin Interven Ra-
treatment of malignant hepatic tumors: at the threshold of a major
breakthrough. Radio Graphics2000;20:9 –27.
27. Rossi S, Di Stasi M, Buscarini E, et al. Percutaneous radiofre-
37. Goldberg SN, Gazelle GS, Solbiati L, Rittman WJ, Mueller PR.
quency interstitial thermal ablation in the treatment of small hep-
Radiofrequency tissue ablation: increased lesion diameter with a
atocellular carcinoma. Cancer J Sci Am 1995;1:73– 81.
perfusion electrode. Acad Radiol 1996;3:636 – 44.
28. Ebra M. Percutaneous ethanol injection for the treatment of hep-
38. Gillams A, Lees WR. Image guided ablation of colorectal liver
atocellular carcinoma: study of 95 patients. Gastroenterol Hepatol
metastases: time for a randomized controlled trial versus hepatic
resection. Radiology 1999;213P:212.
29. Lencioni R, Pinto F, Armillotta N, et al. Long-term results of
39. Gillams A. Thermal ablation of liver metastases. Abdominal Im-
percutaneous ethanol injection therapy for hepatocellular in cirrho-
sis: a European experience. Eur Radiol 1997;7:514 –9.
40. Bleicher RJ, Allegra DP, Nora DT, Wood TF, Foshag LJ, Bilchik
30. Riley DK, Babinchak TJ, Zemel R, Weaver ML, Rotheram EB.
AJ. Radiofrequency ablation in 447 complex unresectable liver
Infection complications of hepatic cryosurgery. Clin Infect Dis
tumors: lessons learned. Ann Surg Oncol 2003;10:52– 8.
41. Elias D, Goharin A, El Otmany A, et al. Usefulness of intraoper-
31. Adam R, Akpinar E, Johann M, Kunstlinger F, Majno P, Bismuth
H. Place of cryosurgery in the treatment of malignant liver tumors.
ative radiofrequency thermoablation of liver tumors associated or
not with hepatectomy. Eur J Surg Oncol 2000;26:763–9.
32. Korpan NN. Hepatic cryosurgery for liver metastases: long-term
42. Que FG, Nagorney DM, Batts KP, Linz LJ, Kvols LK. Hepatic
follow-up. Ann Surg 1997;225:193–201.
resection for metastatic neuroendocrine carcinomas. Am J Surg
33. Yeh KA, Fortunato L, Hoffman JP, Eisenberg BL. Cryosurgical
ablation of hepatic metastases from colorectal carcinomas. Ann
43. Carty SE, Jensen RT, Norton JA. Prospective study of aggressive
resection of metastatic pancreatic endocrine tumors. Surgery 1992;
34. Rossi S, Di Stasi M, Buscarini E, et al. Percutaneous RF interstitial
thermal ablation in the treatment of hepatic cancer. Am J Roent-
44. Berber E, Flesher N, Siperstein AE. Laparoscopic radiofrequency
ablation of neuroendocrine liver metastases. World J Surg 2002;
35. Solbiati L, Goldberg SN, Ierace T, et al. Hepatic metastasis:
Ann Surg Oncol, Vol. 10, No. 9, 2003
ARVSFONDEN NYA PROJEKT DECEMBER 2013 I december 2013 delade Arvsfonden ut 118,9 miljoner kronor till 77 projekt. Av dessa var 25 projekt nya och fick dela på 33,3 miljoner kronor Nya projekt december 2013 IK Nordia,GRILLBY Nybyggnation av samlingslokalen Nordiahallen på Grillby 74:1 i Enköping kommun har beviljats stöd med 2272000 kronor för år 1 av 1 Idrottsföreningen IK N
HOW TO USE DR. PEAT’S 10% NATURAL BIOIDENTICAL PROGESTERONE IN VITAMIN E The minimum maintenance dose of Progest-E oil is 3 drops daily, usual y from mid-cycle to menses. Women who have little to no symptoms at al can take this dosage. The more severe your symptoms, the more doses you need. It is recommended that nearly everyone should begin with the high dose directions for 10 da
 Annals of Surgical Oncology, 10(9):1059–1069
Annals of Surgical Oncology, 10(9):1059–1069 and potentially cure primary and secondary liver disease
reserve inadequate to tolerate major hepatic resection. In
all cases, the intent of the surgical procedure could not
Radiofrequency ablation (RFA) has become a widely
have been curative had it not been associated with RFA.
and potentially cure primary and secondary liver disease
reserve inadequate to tolerate major hepatic resection. In
all cases, the intent of the surgical procedure could not
Radiofrequency ablation (RFA) has become a widely
have been curative had it not been associated with RFA. MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIES
electrode is a 15-gauge, 12- to 15-long insulated cannula
these patients are shown in Table 1. Combined hepatic
that contains 10 to 12 individual hook-shaped electrode
resection and RFA was used to treat metastatic colorectal
arms that are deployed in situ. For tumors Ͻ2.5 cm in
cancer in the overwhelming majority of cases: 124 pa-
diameter, the multiple array was deployed into the center
tients (72.1%). Metastatic leiomyosarcoma was the sec-
of the tumor. For larger lesions, the array was first
ond most commonly treated lesion (n ϭ 13, 7.6%),
deployed at the most posterior interface (ultrasono-
whereas only 5 patients (2.9%) had multifocal HCC.
MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIES
electrode is a 15-gauge, 12- to 15-long insulated cannula
these patients are shown in Table 1. Combined hepatic
that contains 10 to 12 individual hook-shaped electrode
resection and RFA was used to treat metastatic colorectal
arms that are deployed in situ. For tumors Ͻ2.5 cm in
cancer in the overwhelming majority of cases: 124 pa-
diameter, the multiple array was deployed into the center
tients (72.1%). Metastatic leiomyosarcoma was the sec-
of the tumor. For larger lesions, the array was first
ond most commonly treated lesion (n ϭ 13, 7.6%),
deployed at the most posterior interface (ultrasono-
whereas only 5 patients (2.9%) had multifocal HCC. Patient tumor burden characteristics
the operation. The median operative time for the com-bined procedure was 3.0 hours (range, 1– 8.13 hours)
with a median blood loss of 200 cc (range, 50 –2000 cc).
Patient tumor burden characteristics
the operation. The median operative time for the com-bined procedure was 3.0 hours (range, 1– 8.13 hours)
with a median blood loss of 200 cc (range, 50 –2000 cc). MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIES
Postoperative complications and deaths: postoperative deaths (n ϭ 4, 2.3%)
HCC, hepatocellular carcinoma; CRC, colorectal carcinoma metastasis; RFA, radiofrequency ablation; OR, operating room; EBL, estimated blood
loss; ARDS, adult respiratory distress syndrome; MSOF, multiple system organ failure.
MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIES
Postoperative complications and deaths: postoperative deaths (n ϭ 4, 2.3%)
HCC, hepatocellular carcinoma; CRC, colorectal carcinoma metastasis; RFA, radiofrequency ablation; OR, operating room; EBL, estimated blood
loss; ARDS, adult respiratory distress syndrome; MSOF, multiple system organ failure.
 Details of tumor recurrence after hepatic resection and RFA: recurrence at the RFA site
As colorectal cancer is the major type of hepatic
On multivariate survival analysis, the size of the RFA
metastasis confronting surgeons in the United States, we
lesion was the only factor that significantly impacted
felt it important to analyze this group separately. As
survival. Patients who underwent RFA of a lesion Ͼ3 cm
noted above, those patients with colorectal metastases
had a higher likelihood of death than those who under-
had a median actuarial survival of 37.3 months. Addi-
went RFA of a lesion Յ3 cm (HR ϭ 1.85, CI ϭ 1.02–
tional analysis revealed that patients with synchronous
3.37, P ϭ .04). Similar to univariate analysis, there was
colorectal metastasis had a better overall survival as
a trend suggesting that patients with synchronous hepatic
compared to patients with metachronous metastases
metastases did better than those patients with metachro-
nous lesions (HR ϭ .64, CI ϭ .36 –1.14, P ϭ .13).
Details of tumor recurrence after hepatic resection and RFA: recurrence at the RFA site
As colorectal cancer is the major type of hepatic
On multivariate survival analysis, the size of the RFA
metastasis confronting surgeons in the United States, we
lesion was the only factor that significantly impacted
felt it important to analyze this group separately. As
survival. Patients who underwent RFA of a lesion Ͼ3 cm
noted above, those patients with colorectal metastases
had a higher likelihood of death than those who under-
had a median actuarial survival of 37.3 months. Addi-
went RFA of a lesion Յ3 cm (HR ϭ 1.85, CI ϭ 1.02–
tional analysis revealed that patients with synchronous
3.37, P ϭ .04). Similar to univariate analysis, there was
colorectal metastasis had a better overall survival as
a trend suggesting that patients with synchronous hepatic
compared to patients with metachronous metastases
metastases did better than those patients with metachro-
nous lesions (HR ϭ .64, CI ϭ .36 –1.14, P ϭ .13).
 MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIES
Patients with noncolorectal metastases had a significantly
better median survival (59 months) as compared with those patientswith colorectal metastases (37.3 months) (P ϭ .03).
MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIES
Patients with noncolorectal metastases had a significantly
better median survival (59 months) as compared with those patientswith colorectal metastases (37.3 months) (P ϭ .03). of several alternative treatment methods designed to pro-
a population of patients who have a larger tumor burden
vide therapy for the majority of patients diagnosed with
associated with biologically more aggressive disease and
liver cancer who are not candidates for surgical
an inherently poorer prognosis. Performing a potentially
morbid procedure (such as a resection with RFA) would
Interstitial local ablative techniques involving either
be unwarranted if it could not lead to meaningful long-
freezing (cryoablation),22,23 chemical desiccation (alco-
term survival in a subset of patients. In reviewing the
hol ablation),24,25 or RFA9,26,27 have all been described.
of several alternative treatment methods designed to pro-
a population of patients who have a larger tumor burden
vide therapy for the majority of patients diagnosed with
associated with biologically more aggressive disease and
liver cancer who are not candidates for surgical
an inherently poorer prognosis. Performing a potentially
morbid procedure (such as a resection with RFA) would
Interstitial local ablative techniques involving either
be unwarranted if it could not lead to meaningful long-
freezing (cryoablation),22,23 chemical desiccation (alco-
term survival in a subset of patients. In reviewing the
hol ablation),24,25 or RFA9,26,27 have all been described. MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIES
ysis, the amount of blood loss did seem to affect overall
study, multivariate analysis revealed that a total number
survival with patients experiencing Ͼ 1000 cc blood loss
of tumors Ͼ10 was significantly associated with a short
having a significantly decreased median survival. One pos-
time to recurrence (Ͻ3.0 months). Patients with Ͼ10
sible reason for this is that blood loss may have acted as a
tumors clearly represent a cohort of patients with a
surrogate marker for not only the complexity of the surgical
significant tumor burden who may be more likely to
resection, but also the extent of hepatic disease.
MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIES
ysis, the amount of blood loss did seem to affect overall
study, multivariate analysis revealed that a total number
survival with patients experiencing Ͼ 1000 cc blood loss
of tumors Ͼ10 was significantly associated with a short
having a significantly decreased median survival. One pos-
time to recurrence (Ͻ3.0 months). Patients with Ͼ10
sible reason for this is that blood loss may have acted as a
tumors clearly represent a cohort of patients with a
surrogate marker for not only the complexity of the surgical
significant tumor burden who may be more likely to
resection, but also the extent of hepatic disease. failed one chemotherapy regimen and had fewer subse-
NIH conference on hepatocellular carcinoma. Ann Intern Med
quent treatment options. In contrast, patients with syn-
2. Weiss L, Grundmann E, Torhorst J, et al. Hematogenous metastatic
chronous liver metastases underwent resection of their
patterns in colonic carcinoma: an analysis of 1541 necropsies.
failed one chemotherapy regimen and had fewer subse-
NIH conference on hepatocellular carcinoma. Ann Intern Med
quent treatment options. In contrast, patients with syn-
2. Weiss L, Grundmann E, Torhorst J, et al. Hematogenous metastatic
chronous liver metastases underwent resection of their
patterns in colonic carcinoma: an analysis of 1541 necropsies. MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIES
injection in the treatment of hepatocellular carcinoma in cirrhosis.
MULTIMODAL TREATMENT OF HEPATIC MALIGNANCIES
injection in the treatment of hepatocellular carcinoma in cirrhosis.