Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
7020883
Serum and cerebrospinal fluid concentrations of melatonin: a pilot study in healthy male volunteers A. Rousseau1, S. Petrén1, J. Plannthin1, T. Eklundh2, and C. Nordin1
1 Department of Neuroscience and Locomotion, Division of Psychiatry,
2 Department of Clinical Neuroscience and Family Medicine, Psychiatry Section,
Huddinge University Hospital, Huddinge, Sweden
Received November 17, 1998; accepted April 20, 1999
Summary. Melatonin was determined in serum and cerebrospinal fluid (CSF) obtained from 13 healthy males lumbar-punctured in the sitting position without preceding bed rest.
There was a significant correlation between the levels of melatonin in
The serum concentration was lower than that in the CSF, a finding that
calls in question the theory that melatonin is mainly released from the pinealgland into the bloodstream.
In conclusion, serum levels of melatonin in healthy male volunteers, mir-
ror the CSF concentrations when lumbar puncture is carried out using thedescribed technique. Keywords: Melatonin, cerebrospinal fluid, serum. Introduction
The indoleamine melatonin (5-methoxy-N-acetyltryptamine) is a peptide-hormone synthesised and secreted by the pineal gland. Melatonin secretiondisplays a circadian rhythm (Adrendt et al., 1977) and it also exhibits seasonalas well as interindividual variation (Bergiannaki et al., 1996). Various studieshave indicated that melatonin influences sleep (Chase and Gidal, 1997),body temperature (Deacon et al., 1994), the immune system (Hofbauer andHeufelder, 1996) and mental performance (Slotten and Krekling, 1996). Owing to the inversed relationship between melatonin and cortisol, melatoninis of specific interest in affective disorders (Wetterberg et al., 1979; Brown,1989).
Few studies have compared melatonin concentrations in human cere-
brospinal fluid (CSF) and blood. According to current concepts, melatonin
levels are higher in blood than in the CSF (Adrendt et al., 1977; Cardinali,1981; Young et al., 1984). However, a single report has shown higher levels inthe CSF (Bruce et al., 1991).
The concentrations of compounds in lumbar CSF have been assumed to
mirror the levels in the central nervous system (CNS), an assumption that hasbeen called in question, however (Meltzer and Lowy, 1987; Potter and Manji,1993; Altemus et al., 1994). One major reason is that CSF concentrations areinfluenced by confounding factors such as age, height, body weight, volumeof CSF drawn, diet, site of puncture (Bertilsson and Åsberg, 1984), motility(Post et al., 1980; Bertilsson and Åsberg, 1984), neuraxis distance (Nordinet al., 1993), atmospheric pressure (Nordin et al., 1992; Eklundh et al., 1994)and CSF collection time (tapping-time) (Nordin et al., 1993). If these factorsare of significance for melatonin in the CSF as well as for the other com-pounds, they have to be taken into consideration when interpreting CSF dataon melatonin.
The primary aim of the present study was to investigate whether there is
a relationship between the serum and CSF concentrations of melatonin. Fur-thermore, we wanted to elucidate whether the concentration of melatonin inlumbar CSF is influenced by the confounding factors mentioned above. Thestudy is exploratory and hypothesis generating. Subjects and methods
The subjects comprised 13 healthy males (aged 25.3 Ϯ s.d. 4.5, Table 1) recruited amongmedical students and their friends. Prior to experimentation, the subjects were inter-
Table 1. Clinical data on 13 lumbar punctured male volunteers (mean Ϯ SD)
viewed, physically examined and bloodtested based on the following exclusion criteria:having either neurological, cardiovascular, hepatic, renal, haematopoetic, gastrointesti-nal, metabolic or psychiatric dysfunction, receiving medication on a regular basis. Allsubjects participated in the study after giving their informed consent.
Lumbar puncture was performed at the L 4–5 level at 8–9 a.m. after a minimum of 8
hours in the fasting state. There was no restriction concerning rest during the 8 hourspreceding the puncture. With the volunteer in a sitting position, CSF was obtained byallowing it to drip into a test tube using a disposable needle (Becton – Dickinson 0.70 ϫ75 mm). The CSF collection time was recorded. The first two consecutive 6-ml fractions ofCSF were immediately protected from light, centrifuged at 3,500 rpm for 2 minutes andstored at Ϫ70°C until analysed. Immediately after the lumbar puncture, a 6-ml venousblood sample was obtained using a standard venipuncture technique.
Melatonin was analysed using radioimmunoassay technique using [3H] melatonin
as a tracer. The intra-assay variability is 7% and the inter-assay variability is 10%(Wetterberg et al., 1978).
Data on atmospheric pressure in Linköping were obtained from a meteorologist at
SAAB airport, located less than 10 km from the hospital.
The StatView 4.5 (Abacus Concepts Inc.) program was used for statistical calcula-
tions. Parametric statistics were employed according to Kleinbaum et al. (1988). Inrepeated stepwise regression analyses (F-to-Enter set at 4.75), the concentration of mela-tonin in 12 ml of CSF was used as the dependent variable. The serum concentration ofmelatonin, age of the volunteer, body mass index (BMI), CSF collection time, atmo-spheric pressure and neuraxis distance (from the external occipital protuberance to thesite of puncture) in the sitting position were used as regressors. Due to the study design,environmental light conditions were not controlled for.
The Ethics Committee of the University Hospital in Linköping, Sweden, approved
Clinical data on the volunteers are presented in Table 1. On using the stepwiseregression technique, we found that the concentration of melatonin in 12 ml ofCSF was influenced by the serum level (r ϭ 0.72, p ϭ 0.0059; Fig. 1), but notby any of the confounding factors.
The concentration of melatonin in 12 ml of CSF was significantly higher
than the serum level (paired t-test; t ϭ 2.52, p ϭ 0.0272).
There was no difference between the concentrations of melatonin when
comparing the first (0–6 mL) and the second (7–12 mL) CSF fraction (t ϭ 0.73;NS). Discussion
The major finding of the study is a correlation between the concentration ofmelatonin in serum and the CSF. This is in line with previous findings in sheep(Shaw et al., 1989) and in a small sample of 4 volunteers (Bruce et al., 1991). Our findings may be explained by a relatively unrestricted exchange of mela-tonin across the blood-brain barrier, owing to the fact that melatonin is highlylipid-soluble (Reiter et al., 1994). At any rate, the finding of a correlationindicates that serum melatonin can be used to predict the concentration inlumbar CSF, when sampled as described above with the volunteer in thesitting position after 8 hours of fasting. Fig. 1. Simple regression plot showing the correlation between melatonin in the CSF and
serum (r ϭ 0.72; p ϭ 0.0059; Y ϭ 0.048 ϩ 1.08 * X)
The level of melatonin in lumbar CSF was significantly higher than in
simultaneously sampled serum. This is an unexpected finding. The route bywhich melatonin reaches its targets is not known, but it has been assumed thatsecretion must be effectuated through venous drainage into the peripheralcirculation because of the pineal morphology (Kappers et al., 1974) andfindings of higher levels of melatonin in the blood than in the CSF (Arendtet al., 1977; Cardinali, 1981; Young et al., 1984). However, animal studies haveshown that intraventricular injections of melatonin elevates plasma melatoninlevels within one minute, while subcutaneous infusion yields three timeshigher melatonin levels in plasma than in CSF (Kanematsu et al., 1989; Vitteet al., 1988), indicating a rapid turnover of CSF melatonin and compatibilitywith the hypothesis of a direct pineal secretion of melatonin into the ventricu-lar system.
Each individual has his own temporal profile of circadian melatonin
secretion which varies little intra-individually but widely inter-individually(Coetzee et al., 1989; Bruce et al., 1991). It also seems as if the melatonin CSFprofile lags about 30 minutes compared to plasma levels, e.g. the nocturnalpeak comes 30 minutes earlier in plasma than in CSF (Bruce et al., 1991). Thismy be part of the explanation why CSF levels were higher than plasma levelsas melatonin levels were dropping at the time of sampling.
In previous studies on humans (e.g., Young et al., 1984), nothing was
reported on the position of the volunteers at lumbar puncture. When inter-
preting data on amine metabolites in the CSF, the position of the subject hasto be taken into account (Bertilsson and Åsberg, 1984). Posture is also ofinterest for plasma melatonin since moving from a supine to a standing posi-tion yields increasing levels (Deacon and Arendt, 1994).
No difference was found on comparing melatonin concentrations in two
consecutive CSF fractions. This homogeneity supports findings in earlierstudies (Young et al., 1984), but contrasts with observations regarding neu-rotransmitter metabolites, which usually display concentration gradients inCSF (Siever et al., 1975; Sjöström et al., 1975; Nordin et al., 1982, 1995). Thelack of a melatonin concentration gradient may be explained by a high rate ofexchange across the blood-brain barrier. Another plausible explanation mightbe that no metabolism of the hormone occurs in the lower part of the CSFcompartment.
The presumed confounding factors did not influence CSF melatonin levels
in the present study and apparently may not need to be taken into accountwhen following the described puncture procedure. Acknowledgements
This study was supported by grants from the Söderström-König Foundation and from theResearch Foundation of the University Hospital in Linköping. We thank our researchnurse, Ms. M. Mansfield, for her invaluable help and assistance. References
Altemus M, Swedo S, Leonard H, et al (1994) Changes in cerebrospinal fluid neuro-
chemistry during treatment of obsessive-compulsive disorder with clomipramine. Arch Gen Psychiatry51: 794–803
Adrendt J, Wetterberg L, Heyden T, Sizonenko PC, Paunier L (1977) Radioimmunoas-
say of melatonin: human serum and cerebrospinal fluid. Horm Res 8(2): 65–75
Bergiannaki JD, Paparrigopoulos TJ, Stefanis CN (1996) Seasonal pattern of melatonin
excretion in humans: relationship to daylength variation rate and geomagnetic fieldfluctuations. Experientia 52: 253–7
Bertilsson L, Åsberg M (1984) Amine metabolites in the cerebrospinal fluid as a measure
of central neurotransmitter function: methodological aspects. In: Usdin E, Åsberg M,Bertilsson L, Sjöqvist F (eds) Frontiers in biochemical and pharmacological researchin depression. Raven Press, New York, pp 27–34
Brown GM (1989) Psychoneuroendocrinology of depression (Review). Psychiatr J Univ
Bruce J, Tamarkin L, Riedel C, Markey S, Oldfield E (1991) Sequential cerebrospinal
fliud and plasma sampling in humans: 24-hour melatonin measurements in normalsubjects and after peripheral sympathectomy. J Clin Endocrinol Metabol72(4): 819–23
Cardinali DP (1981) Melatonin: a mammalian pineal hormone. Endocr Rev 2: 327–
Coetzee JA, Theron JJ, van der Merwe CA (1989) Consecutive melatonin circadian
rhythms in normal volunteers. S Afr Med J 75(4): 163–5
Deacon S, Arendt J (1994) Posture influences melatonin concentrations in plasma and
saliva in humans. Neurosci Lett 167: 191–194
Deacon S, English J, Arendt J (1994) Acute phase-shifting effects of melatonin asso-
ciated with suppression of core body temperature in humans. Neurosci Lett 178(1):32–4
A. Rousseau et al.: Melatonin in the cerebrospinal fluid
Eklundh T, Fernström V, Nordin C (1994) Influence of tapping time and atmospheric
pressure on concentrations of monoamine metabolites in cerebrospinal fluid – aprospective study in female volunteers. J Psychiatr Res 28: 511–17
Hofbauer LC, Heufelder AE (1996) Endocrinology meets immunology: T lymfocytes as
novel targets for melatonin. Eur J Endocrinol 134(4): 424–5
Kanematsu N, Mori Y, Hayashi S, Hoshino K (1989) Presence of a distinct 24-hour
melatonin rhythm in the ventricular cerebrospinal fluid of the goat. J Pineal Res7(2):143–152
Kappers JA, Smith AR, De Vries RAC (1974) The mammalian pineal gland and its
control of hypothalamic activity. Prog Brain Res 41: 149–174
Kleinbaum DG, Kupper LL, Muller KE (1988) Applied regression analysis and other
multivariable methods. PWS-KENT Publishing Company, Boston
Meltzer HY, Lowy MT (1987) The serotonin hypothesis of depression In: Meltzer HY
(ed) Psychopharmacology: the third generation of progress. Raven Press, New York,pp 513–526
Nordin C, Bertilsson L, Siwers B (1982) Site of lumbar puncture influences levels of
monoamine metabolites. Arch Gen Psychiatry 39: 1145
Nordin C, Swedin A, Zachau AC (1992) CSF 5-HIAA and atmospheric pressure. Biol
Nordin C, Swedin A, Zachau AC (1993) Tapping-time influences concentrations of
5-HIAA in the CSF. J Psychiatr Res 27(4): 409–414
Nordin C, Eklundh T, Fernström V, Swedin A, Zachau AC (1995) Gradients of CSF
monoamine metabolites: a comparison between male and female volunteers. JPsychiatr Res29(2): 133–140
Post R, Ballenger J, Goodwill F (1980) Cerebrospinal fluid studies of neurotransmitter
function in manic and depressive illness. In: Wood JH (ed) Neurobiology of cere-brospinal fluid. Plenum Press, New York London, pp 685–717
Potter W, Manji H (1993) Are monoamine metabolites in cerebrospinal fluid worth
measuring? Arch Gen Psychiatry50: 653–6
Reiter RJ, Tan D-X, Poeggeler B, Menendez-Pelaez A, Chen L-D, Saarela S (1994)
Melatonin as a free radical scavenger: implications for aging and age-related diseases. Ann NY Acad Sci 719: 1–12
Shaw PF, Kennaway DJ, Seamark RF (1989) Evidence of high concentrations of melato-
nin in lateral ventricular cerebrospinal fluid of sheep. J Pineal Res 6(3): 201–8
Siever L, Kraemer H, Sack R, Angwin P, Zarcone V, Barchas I, Brodie K (1975) Gradi-
ents of biogenic amine metabolites in cerebrospinal fluid. Dis Nerv Syst36: 13–16
Sjöström R, Ekstedt J, Änggård E (1975) Concentration gradients of monoamine me-
tabolites in human cerebrospinal fluid. J Neurol Neurosurg Psychiatry38: 666–8
Slotten HA, Krekling S (1996) Does melatonin have an effect on cognitive performance?
Vitte PA, Harthe C, Lestage P, Claustrat B, Bobillier P (1988) Plasma, cerebrospinal
fluid, and brain distribution of 14C-melatonin in rat: a biochemical and autoradio-graphic study. J Pineal Res 5(5): 437–453
Wetterberg L, Eriksson O, Friberg Y, Vangbo B (1978) A simplified radioimmunoassay
for melatonin and its application to biological fluids: preliminary observations on thehalf-life of plasma melatonin in man. Clin Chim Acta 86: 169–177
Wetterberg L, Beck-Friis J, Aperia B, Petterson U (1979) Melatonin/cortisol ratio in
Young SN, Gauthier S, Kiely ME, Lal S, Brown GM (1984) Effect of oral melatonin
administration on melatonin, 5-hydroxyindoleacetic acid, indoleacetic acid and cyclicnucleotides in human cerebrospinal fluid. Neuroendocrinology 39(1): 87–92
Authors’ address: Dr. A. Rousseau, Division of Psychiatry, University Hospital,
S-581 85 Linköping, Sweden, e-mail: [email protected]
____________________________________________________________________________________ FOR IMMEDIATE RELEASE Media Contacts: FDA Approves OXYTROL® FOR WOMEN, the First Over-the-Counter Treatment for Overactive Bladder in Women New Over-the-Counter Option for More Than 20 Million Women with Overactive Bladder WHITEHOUSE STATION, N.J., January 25, 2013 – Merck (NYSE: M
Medications Affected by Federal Pricing These drugs will remain available in TRICARE mail order without needing a provider pre-authorization; the implementation date for these drugs will not take affect until after 1 JAN 10 and no later than 180 days after the TRICARE Management Activity (TMA) Director’s approval; and if a Price Agreement is received prior to 14 OCT the drug may stay in Ti
 Serum and cerebrospinal fluid concentrations of melatonin:
Serum and cerebrospinal fluid concentrations of melatonin: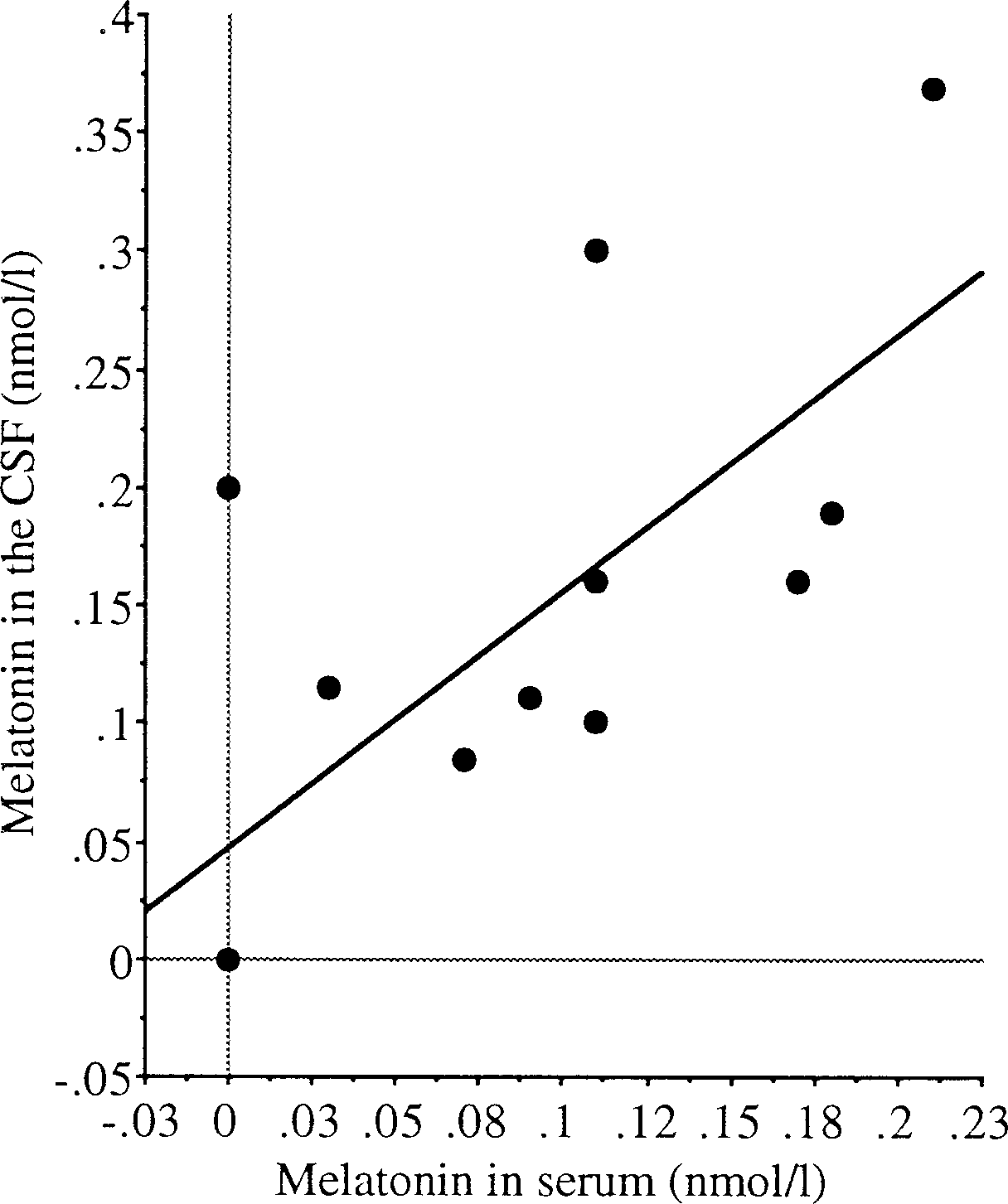 Fig. 1. Simple regression plot showing the correlation between melatonin in the CSF and
Fig. 1. Simple regression plot showing the correlation between melatonin in the CSF and