Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Drugs: telmisartan and amlodipine
Enobosarm, a selective androgen receptor modulator, prevents muscle wasting in advanced non-small cell lung cancer (NSCLC)
By R.M. Hadfield, PhD SYDNEY, Australia -- October 31, 2013 – Enobosarm was well tolerated and increased lean body mass in patients with advanced NSCLC according to a poster presentation here at the 15th World Conference on Lung Cancer (WCLC) on October 30. Jeffrey Crawford, MD, Professor of Medicine, Division of Medical Oncology, Duke University School of Medicine, Durham, NC, USA, conducted the study to determine whether Enobosarm, a selective androgen receptor modulator (SARM), could prevent and treat muscle wasting in advanced NSCLC. “Cancer induced muscle wasting is a selective and progressive cancer related symptom that begins early in the course of malignancy,” noted Professor Crawford. “Greater than 50% of NSCLC patients have muscle wasting at diagnosis, increasing to >80% prior to death,” he added. The two phase-3 randomized, placebo controlled trials, called POWER-1 and 2 (prevention and treatment of muscle wasting in patients with cancer), enrolled 641 patients diagnosed with stage III or IV NSCLC, ECOG score ≤1 and body mass index (BMI) ≤32 kg/m2. Patients received either Platinum + Taxane or Platinum + Non-Taxane and in each arm patients were randomized to receive either oral Enobosarm (3mg, once daily) or placebo. At day 84 co-primary endpoints of lean body mass (LBM) and physical function, measured by stair climb power (SCP), were assessed. In those patients receiving Platinum + Taxane, 41.9% in the Enobosarm arm vs. 30.4% in the placebo arm maintained or increased their LBM (P = 0.036). In patients receiving Platinum + Non-Taxane, 46.5% in the Enobosarm arm vs. 37.9% in the placebo arm maintained or increased their LBM (P = 0.113). For SCP, the proportion of patients with improvement of >10%, was not significantly different between Enobosarm and placebo for either group, with P values of 0.315 and 0.289, in the Platinum + Taxane and Platinum + Non-Taxane groups, respectively. Mixed model repeated measures (MMRM) for slopes and means at day 147 showed significant improvement in LBM, with P values of <0.0001and 0.0036 in the Platinum + Taxane and Platinum + Non-Taxane groups, respectively. For SCP, the improvement was only significant in the Platinum + Taxane group (P = 0.0486).
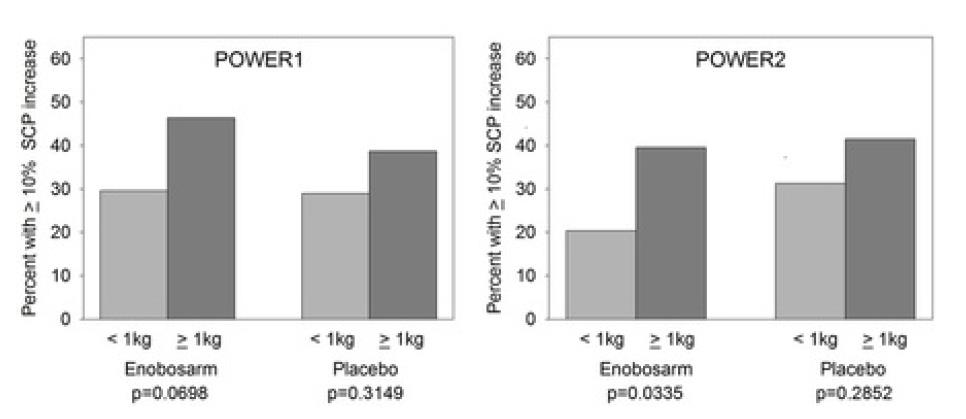
Baseline characteristics and adverse events were mostly similar between Enobosarm and placebo groups. Of note, decreased appetite was experienced in 16.8% of Platinum + Taxane placebo patients compared to only 6.9% of Enobosarm patients. “Enobosarm was very well tolerated in both trials,” commented Professor Crawford. “In general, patients that maintained or increased LBM had greater increases in SCP and survived longer regardless of treatment,” he added. [Presentation title:Results from two Phase 3 randomized trials of Enobosarm, selective androgen receptor modulator (SARM), for the prevention and treatment of muscle wasting in NSCLC. Abstract P3.11-026] P3.11-026 | Results from two Phase 3 randomized trials of enobosarm, selective androgen receptor modulator (SARM), for the prevention and treatment of muscle wasting in NSCLC. Authors: Jeffrey Crawford1, Carla M.M. Prado2, Michael L. Hancock3, Mary A. Johnston3, James T. Dalton3, Mitchell S. Steiner3 1Duke University School of Medicine, Durham, NC/UNITED STATES OF AMERICA, 2Florida State University, Tallahassee, FL/UNITED STATES OF AMERICA, 3GTx, Inc., Memphis/UNITED STATES OF AMERICA Background: Cancer induced muscle wasting is a selective and progressive cancer related symptom that begins early in the course of malignancy. Greater than 50% of NSCLC patients have muscle wasting at diagnosis, increasing to >80% prior to death. Previous evidence suggests that a 1kg gain in lean body mass (LBM) is beneficial for increasing muscle strength. Enobosarm is a first-in-class nonsteroidal oral SARM. We report herein results for two Phase 3 enobosarm clinical trials, POWER1 (P1) and POWER2 (P2), for the prevention and treatment of muscle wasting in patients with advanced NSCLC. Methods: Patients with Stage III or IV NSCLC were randomized into the trials at initiation of first-line chemotherapy based upon the chemotherapy regimen prescribed; platinum+taxane(P1, n=321) or platinum+non-taxane(P2, n=320). Patients (males and postmenopausal females ≥30y with ECOG ≤1) received either enobosarm 3mg or placebo for 5 months. LBM was measured by DXA and physical function was assessed by stair climb power (SCP) at days 84 (primary endpoint) and 147. Results: Enobosarm had a significant effect on LBM at day 84 and 147 in both trials (P1:p=0.0003 and < 0.0001; P2: p=0.0227 and 0.0036 by continuous variable analyses). Additionally, a larger proportion of patients receiving enobosarm maintained or increased LBM at day 84 and 147 in both trials (P1:p=0.036 and 0.026; P2:p=0.113 and 0.013) as compared to placebo. Regardless of treatment, patients with ≥1kg increase in LBM were more likely to demonstrate ≥10% increase in SCP than patients that had lesser increases or had decreases in LBM (P1: 43.7% vs 29.3%, p=0.0250 and P2: 40.5% vs 26.5%, p=0.0321). The percentage improvement in SCP from baseline to day 84 differed significantly between patients with and without a ≥1kg increase in LBM: 9.1% vs -1.0% in P1(p=0.0022) and 7.7% vs -.0.6% in P2(p=0.0046). Importantly, patients with ≥1kg increases in LBM were more likely to demonstrate a ≥10% increase in SCP if they received enobosarm (P1: p=0.0698[trend] and P2: p=0.0335) than placebo (P1:p=0.3149 and P2:p=0.2852), suggesting that LBM increases in enobosarm-treated patients were more highly associated with SCP improvements in both trials (Figure). In general, patients that maintained or increased LBM had greater increases in SCP and survived longer (landmark analysis) regardless of treatment. The incidence of adverse events was similar between enobosarm and placebo in both trials. Conclusion: Overall, enobosarm was safe and well tolerated. Enobosarm had an unambiguous effect on muscle that may translate into improvement in physical function and survival in NSCLC patients.
ANSWERS TO FREQUENTLY ASKED MEDICAL QUESTIONS What inoculations, if any, should a practitioner administer to my child before departure? SYA sends a special “Medical Care and Inoculations” document to SYA China families. For students going to Europe, we do not have firm recommendations. Therefore, we suggest you use the CDC Web site as a reference and consult with your personal physici
Transmission Symptoms Treatment Reduce Your Risk prevents the most common strains of HPV. can’t see a sore during penis, vagina, anus, Blood, semen, vaginal Possibly no symptoms. Blood, semen, vaginal Depleted immune system. No cure. infections in 2006. enters the body of an If you want to be protected against STIs, practice safer
 Conclusion:
Conclusion: