Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
2005-10
Chronic Myeloproliferative Disorders • Research PaperPegylated interferon for the treatment of high risk essential thrombocythemia: results of a phase II study
Background and Objectives. Patients with high-risk essential thrombocythemia require
cytoreductive therapy in order to normalize the elevated platelet counts. We evaluated
the efficacy and toxicity of pegylated interferon in high-risk essential thrombocythemia
Design and Methods. Thirty-six patients with high-risk essential thrombocythemia
(median age 54 years; range, 24-72 years) were studied. The dose of pegylated inter-
feron was initially 50 mg per week and could be escalated up to 150 mg per week.
Results. During the first three months platelet counts decreased significantly from amedian baseline count of 895¥109/L (range: 383-1779) to a median count of
485¥109/L (range: 211-1283; p£0.001). A complete response was defined as platelet
counts < 450¥109/L. The complete response rate was 39%, 47%, 58% and 67% at 3,
6, 9 and 12 months of treatment, respectively. There were 25%, 11%, 8% and 0% poorresponders, defined as patients with platelet counts > 600¥109/L, at 3, 6, 9 and 12
months of treatment, respectively. After a median time of 23 months (range 3–39months) 23 of 36 patients (64%) are still receiving pegylated interferon. In ten patients(28%) treatment was stopped due to grade 1 to 2 toxicity, classified according to theWHO standard toxicity scale. One patient, who responded partially to pegylated inter-feron (platelet count 542¥109/L), had a cerebral stroke after 23 months of treatment. Interpretations and Conclusions. In high-risk essential thrombocythemia sustainedtreatment with pegylated interferon is effective and safe in reducing platelet countswith a toxicity comparable to that of conventional interferon.
Key words: pegylated interferon, treatment, essential thrombocythemia, ET. From the Department of MedicineIII, University of Ulm, Germany(CL, SS, MG, HB); Department ofMedicine III, Klinikum Mannheim,Fakultät für Klinische Medizin
Essential thrombocythemia is a Phi- the best studied drug and has been proven
to reduce complications related to essen-
als;8,9 however, this drug has a potential to
Mannheim der UniversitätHeidelberg, Mannheim, Germany(EL); Institue of Pathology, University
physicians are still reluctant to treat young
tions.2 However, in about one third of all
patients the disease is benign and there are
urea. However, there is no clear proof that
hydroxyurea alone is increasing the risk of
Center of Clinical Research,University Hospital Freiburg,
Therefore, the identification of patients at
genic drug, conventional interferon-a, has
risk is important. According to retrospec-
University of Vienna, Vienna,Austria (HG).
tive studies, high-risk patients are charac-
terized by an age > 60 years, a very high
years.14-16 The major disadvantage of inter-
bolic event.4-7 The need for cytoreductive
therapy in these high-risk patients is wide-
file of interferon-a through addition of a
Robert-Koch-Strasse 8, D-89081Ulm, Federal Republic of Germany.
ly accepted.3-9 Treatment options include
polyethyleneglycol (pegylation) has result-
cytoreductive drugs, such as hydroxyurea,
ed in slower absorption and a lower elim-
ination rate, thus enabling weekly admin-
sistration, potentially improving compli-
haematologica/the hematology journal | 2005; 90(10) | 1333 |
ance.17 The aim of this phase II study was to evaluatethe safety, toxicity and efficacy of pegylated interfer-
Table 1. Baseline characteristics of the 36 high-risk patients withessential thrombocythemia at enrollment into the study.
on in a group of 36 patients with high-risk essentialthrombocythemia. Design and Methods Patients’ characteristics and study design
Between December 2001 and September 2003 a total
of 36 patients with high-risk essential thrombo-
cythemia were enrolled into this study by 16 German
and Austrian centers. A total of 48 patients had beeneligible for the trial, but 12 patients refused to give their
consent and were thus excluded from the protocol.
Patients were eligible if they were older 18 years, had adiagnosis of essential thrombocythemia meeting the
WHO criteria for this disease and fulfilled at least one
of the following criteria for high-risk essential throm-bocythemia: a platelet count > 1500¥109/L, age > 60
years, or previous complications related to essential
thrombocythemia (thromboembolic or major hemor-rhagic events). Microvascular disturbances were notregarded as an inclusion criterion for high-risk essentialthrombocythemia. With the exception of conventional
ously described.21,22 Data is presented as a ratio between
interferon-a cytoreductive pretreatment was permit-
PRV-1 and the housekeeping gene GAPDH (PRV-
ted. A previous history of psychiatric disorders (in par-
1/GAPDH ratio). PRV-1 positivity was defined as a
ticular previous depression) or severe cardiac, liver or
PRV-1/GAPDH ratio of < 1.15 and PRV-1 negativity
renal dysfunction were regarded as exclusion criteria.
defined as a PRV-1/GAPDH ratio of > 1.19. Out of the
The study was approved by the local ethic committees
26 patients, 18 were negative and 8 were positive for
of the participating centers and written informed con-
PRV-1. Follow-up data are available for six patients: one
sent was obtained from each patient enrolled into this
patient became PRV-1 negative after 11 months and is
still negative after 24 months of therapy with pegylat-
The baseline characteristics at enrollment are shown
ed interferon, the other five patients with follow-up
in Table 1. Treatment was indicated for at least one of
data were already negative at entry into the study.
the following reasons: age > 60 years in 14 patients
Follow-up evaluations were performed on a weekly
(39%), a platelet count > 1500¥109/L in 13 patients
basis during the first three months and subsequently
(36%) or previous complications related to essential
every third month. The follow-up evaluations consist-
thrombocythemia in 18 patients (50%). Ten patients
ed of medical history, physical examination, full blood
(28%) had already received some treatment: eight had
count, serum biochemical assays including liver and
been treated with hydroxyurea and two with anagre-
lide. The median time between diagnosis and entryinto the study was 6.6 months (range: 0.3–93 months). Treatment plan and study endpoints
Pegylated interferon a-2b (Peg-IFNa2b, PegIntron)
Pretreatment evaluation and follow-up
was supplied by Essex Pharma, Germany in vials con-
Pretreatment evaluation included a complete medical
taining 50 mg, 100 mg and 150 mg lyophilized powder,
history and physical examination, abdominal ultra-
along with sterile water for injection. Pegylated inter-
sound, assessment of cardiovascular risk factors (ciga-
feron was administered subcutaneously once weekly
rette smoking, hypertension, diabetes mellitus, and
at a starting dose of 50 mg. In those patients who did
hyperlipidemia), full blood count, electrolytes, liver and
not achieve a platelet count below 500¥109/L after 8-12
renal functions, baseline coagulation tests, bone mar-
weeks, the dosages were increased by 25 mg per week
row cytology and histology and qualitative polymerase
up to 150 mg per week. Dose reduction by 25 mg per
chain reaction analysis to rule out the bcr-abl rearrange-
week was recommended in the case of adverse effects
ment. All 36 patients were bcr-abl negative. At study
related to pegylated interferon and in patients with a
entry, PRV-1 positivity or negativity was determined in
stable platelet count below <450¥109/L for at least four
a quantitative RT-PCR analysis in 26 patients as previ-
weeks. Concomitant therapy with acetaminophen
| 1334 | haematologica/the hematology journal | 2005; 90(10)
(500-1000 mg) was recommended approximately 30minutes before administration of the pegylated inter-
feron to reduce flu-like symptoms. The use of low
dose aspirin (100 mg/day) was optional and at the dis-
cretion of the attending physician. No other cytoreduc-
tive therapy was permitted while the patient was in
le te 1000
We defined the following events as end-points
regarding the treatment with pegylated interferon: (i)major thromboembolic events. (ii) major bleeding,
defined as a decrease in hemoglobin of more than 2
g/dL, life-threatening bleeding or cerebral bleeding; (iii)
microvascular disturbances; (iv) transformation into
baseline
myelofibrosis or blast crisis; (v) intolerable side effects
Months on therapy with pegylated interferon
or patient’s refusal to continue the treatment.
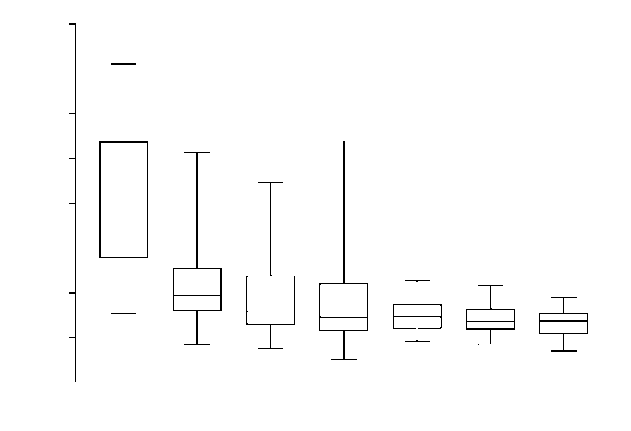
Figure 1. Box plot of the platelet counts at baseline and after 3,6, 9, 12, 18 and 21 months of therapy with pegylated interferon. Response and toxicity criteria
Each box represents the median and interquartile range of values,
A complete hematologic response was defined as a
with the ends of the vertical lines indicating the minimum andmaximum data values.
sustained reduction of platelet counts below 450¥109/Lfor at least one month. A partial hematologic responsewas defined as the reduction of platelets counts tobetween 450 and 600¥109/L. A poor hematologicresponse or no response was defined as a sustained
Efficacy of treatment with pegylated interferon
platelet count > 600¥109/L in spite of therapy.
During the first three months of treatment platelet
Treatment-related toxicity was graded according to the
counts decreased significantly from a median base-
WHO standard toxicity scale on a scale of 0 to 4.
line count of 895¥109/L (range: 383-1779) to a medi-an count of 485¥109/L (range: 211-1283; p<0.001). Statistical analyses
Figure 1 represents the course of the platelet counts
The SAS system was used for the statistical analyses.
as box plots at baseline and after 3, 6, 9, 12, 18 and 21
All response data of patients who received at least one
months of treatment with pegylated interferon. The
dose of pegylated interferon were calculated according
complete response rate (platelet counts <450¥109/L)
to an intention-to-treat analysis. Values were compared
was 39% (14 of 36 patients), 47% (17 of 36 patients),
using the two-sided Wilcoxon test for parallel groups.
58% (21 of 36 patients) and 67% (24 of 36 patients)
All significance levels are two-sided. A box plot analy-
at 3, 6, 9 and 12 months of treatment, respectively.
sis was used for the course of the platelet counts at
The overall response rate (complete and partial
baseline and after 3, 6, 9, 12, 18 and 21 months of ther-
response, i.e. platelet counts <600¥109/L) was 72%
apy. The box itself represents the middle 50% of the
(26 of 36 patients), 72% (26 of 36 patients), 69% (25
data. The upper edge of the box indicates the 75th per-
of 36 patients) and 75% (27 of 36 patients) at 3, 6, 9
centile of the data set, and the lower edge indicates the
and 12 months of therapy, respectively. The rate of
25th percentile. The line in the box indicates the median
poor responders (platelet counts > 600¥109/L) was
value of the data. The ends of the vertical lines indicate
25% (9 of 36 patients), 11% (4 of 36 patients), 8% (3
the minimum and maximum data values.
of 36 patients) and 0% (0 of 36 patients) at 3, 6, 9 and12 months of treatment, respectively. Figure 2 showsthe efficacy of pegylated interferon treatment for all
36 patients with essential thrombocythemia at 3, 6,9, 12, 18 and 21 months.
Patients and dosage level of pegylated interferon
In this phase II study 36 patients with high-risk
Discontinuation and side effects of pegylated
essential thrombocythemia were treated with pegy-
interferon therapy during follow-up
lated interferon (PegIntron). The initial dosage level
After a median time of 23 months (range 3–39
of pegylated interferon used was 50 mg per week.
months) with a total observation time of 763 months,
During follow up the median dose was 50 mg per
23 of 36 patients (64%) are still receiving pegylated
week (range 12.5-150 µg). After 12 months 81% of all
interferon. During the first six months of therapy
treated patients were on a dose £50 mg per week and
with pegylated interferon 28 of 36 patients (78%)
after 21 months 88% of all treated patients were on
reported flu-like symptoms including fever, fatigue,
headache and myalgia. After 12 months of treatment
haematologica/the hematology journal | 2005; 90(10) | 1335 |
Discontinuation of pegylated interferon NC (platelet count > 600¥109/L) PR (platelet count 450-600¥109/L) CR (platelet count < 450¥109/L)
Figure 2. Efficacy of pegylated interferon treatment for all 36
patients with essential thrombocythemia at 3, 6, 9, 12, 18 and21 months. CR: complete remission; PR: partial remission; NC:
no change or poor response. The black bars indicate patients
who discontinued therapy with pegylated interferon at the
Months on therapy with pegylated interferon
the frequency of flu-like symptoms among patients
ered sufficiently with pegylated interferon and an
still on therapy decreased to 36%. Other reported
alternative cytoreductive therapy was initiated. The
side effects included mild depression in up to 15% of
median duration of treatment until its cessation was
treated patients as well as mild hair loss in up to 18%
of treated patients. Furthermore, skin changes, main-ly consisting of increased dryness, were reported by
Thrombotic complications during follow-up
37% of the patients treated over time. All reported
After 23.0 months on therapy with pegylated inter-
side effects decreased in intensity over time. None of
feron a 45-year old patient suffered from a cerebral
the reported adverse events exceeded a grade 2 toxic-
stroke and was subsequently taken out of the study.
ity according to the WHO standard toxicity scale.
A cerebral stroke had been the initial presenting
Table 2 shows the reasons for discontinuation of
symptom of his essential thrombocythemia and the
pegylated interferon in the 13 patients who ceased to
reason why he had entered the study. At the time of
take the drug. In ten patients (28%) therapy was
the second event the dose of pegylated interferon
stopped at the patients´ request due to grade 1 or 2
being administered was 100 mg per week and his
drug related adverse effects: flu-like symptoms with
platelet count was 542¥109/L. This complication
sustained fatigue (n=6), depression (n=1), prolonged
accounted for the total complication rate of 1.7% per
diarrhea (n=1) and alopecia in female patients (n=2).
patient-year. No further thrombocythemia-related
One patient was lost to follow-up after 2.6 months. In
complications were observed in other patients during
another patient the platelet count could not be low-
the total observation period of our study.
Table 2. Reasons for therapy discontinuation in 13 out of 36 patients treated with pegylated interferon. Side effects are classified accord-ing to the WHO standard toxicity scale.
of therapy with pegylated interferon*not related to pegylated interferon.
| 1336 | haematologica/the hematology journal | 2005; 90(10)
patient under therapy with pegylated inter-
feron. This patient was PRV-1 positive at
time (months) 28.03.2003
after 11 months of therapy with pegylated
previously described.21,22 Data are presentedas a ratio between PRV-1 and the house-keeping gene GAPDH (PRV-1/GAPDH ratio).
PRV-1 positivity is defined as a PRV-1/GAPDH ratio of < 1.15 and PRV-1 negativ-
11.01.2005
> 1.19. The other five patients with PRV-1follow-up data were already negative at
17.02.2004
entry into the study and remained negativeduring follow-up (data not shown in this fig-
PRV-1 expression at study entry and during follow up
period of 23 months (range 3-39 months) ten of 36
At study entry, PRV-1 positivity or negativity was
patients (28%) stopped therapy with pegylated inter-
determined in quantitative reverse transcription
feron due to grade 1 or 2 drug-related side effects. The
polymerase chain reaction analysis in 26 patients. Of
observed side effects and the drop-out rate due to
these 26 patients, 18 were negative and 8 were posi-
adverse events are comparable to those reported for
tive for PRV-1. Follow-up data are available for six
patients: one patient became PRV-1 negative after 11
This trial demonstrates that pegylated interferon is
months and is still negative after 24 months of thera-
an effective platelet-lowering drug in patients with
py with pegylated interferon (Figure 3). The other
high-risk essential thrombocythemia. Pegylated inter-
five patients with follow-up data were already nega-
feron exerted its platelet-lowering efficacy not only in
newly diagnosed patients with a high initial plateletcount but also in patients who had been pretreatedwith hydroxyurea or anagrelide. After three months of
Discussion
therapy with pegylated interferon, the proportion ofpatients with a reduction of platelet count <600¥109/L
In this phase II trial 36 patients with high-risk essen-
was 72% (26 of 36 patients). However, after three
tial thrombocythemia were treated with pegylated
months nine of 36 patients (25%) still had a platelet
interferon (PegIntron) to evaluate the safety, toxicity
count >600¥109/L in spite of therapy with pegylated
and efficacy of this drug. Conventional, recombinant
interferon. The hematologic response improved over
interferon-a is an effective treatment in essential
time and after 12 months 75% of our patients (27 of 36
thrombocythemia and a complete hematologic remis-
patients) achieved a platelet count <600¥109/L (24
sion is obtained in about 54% of patients.5 However,
patients with a platelet count <450¥109/L). At this time
about 15% of all essential thrombocythemia patients
there was no patient on treatment with pegylated
are primarily resistant to interferon-a and frequent
interferon who had a platelet count > 600¥109/L. The
side effects limit therapy with this drug.5,14 In a meta-
complete hematologic response rate for pegylated
analysis of 273 patients with essential thrombo-
interferon was at least as good as that reported for con-
cythemia, interferon-a was terminated in 25% of all
ventional interferon-a, ranging from 54% to 70%.5,16,17
patients and in up to 66% of patients in individual tri-
One patient suffered from a cerebral stroke while on
als.14 Utilization of new interferon-a formulations such
pegylated interferon. This event rate of 1.7% per
as pegylated interferon may help to overcome some of
patient-year is comparable to the complication rate in
hydroxyurea-treated high-risk essential thrombo-
The administration of pegylated interferon was safe.
cythemia patients (1.6% per patient-year) observed in
With a median dosage of 50 mg pegylated interferon
a prospective study after a median observation time of
per week (range 12.5–150 mg) we observed no case in
which a dose reduction was necessary due to impaired
There is one small published pilot study concerning
hematopoiesis. In the majority of patients 50 mg pegy-
11 patients with essential thrombocythemia who were
lated interferon per week or less was sufficient to con-
treated with pegylated interferon. All patients were in
trol the platelet count. During the first six months most
complete remission after 4 months.18 After a median
of our patients suffered from mild to moderate flu-like
observation time of 9 months (range 4-17 months) two
symptoms. After one year these side effects disap-
of 11 patients (18%) discontinued therapy because of
peared in most patients. After a median observation
side effects. One patient discontinued therapy at 4
haematologica/the hematology journal | 2005; 90(10) | 1337 |
All authors contributed to the concept of the study, analysis and
months because of persistent grade III fatigue and a
interpretation of the data, and drafting and revising the article. All
second patient at 5 months because of anxiety and
approved the final version. In detail, CL was the secretary and co-
depression. No events related to essential thrombo-
ordinator of the trial; EL was in the steering committee of the trialand was one of its coordinators. HLP performed the PRV-1 assays;
cythemia were observed during the observation peri-
HB performed the statistical analyses; SS was the data manager
od. The initial dose of pegylated interferon was higher
of the trial; HG was in the steering committee of the trial and its co-
than that used in our study (1.5 – 4.5 mg/kg per week). ordinator in Austria; MG was the principal investigator of thistrial. Responsible for all Tables and Figures: MG. The authors also
Further trials with pegylated interferon in essential
declare that they have no potential conflicts of interest.
thrombocythemia are currently under way.19,20
This work was supported by the German Competence Net
Preliminary data from these trials report similar
“Acute and chronic Leukemias” (Project 25). We would like tothank Barbara Stade from essex pharma for organizing supply of
response rates with pegylated interferon20 but a higher
pegylated interferon. We are especially grateful to the following
discontinuation rate due to side effects.19 Our data sug-
centres for participating in this trial: Prof. Dr. Dreyling, Klinikum
gest that pegylated interferon is at least equally effec-
Großhadern Münschen, Dr. Fricke-Jjaya, Elisabeth-Kranken-haus, Recklinghausen, PD Dr. Matzdorff, Universität Giessen,
tive as unmodified interferon in reducing interferon
Dr. Wojatschek, Bad Friedrichshall, PD Dr. Kropff, Universität
platelet counts. Due to an initial slow response to
Münster, Dr. Goldmann, Lüneburg, Dr. Jakob, Medizinische
pegylated interferon, a large proportion of patients
Klinik II, Offenburg, Dr. Procaccianti, Karlsruhe, Dr. Kaesberger,Diakonissenkrankenhaus Stuttgart, Dr. Lengerke, Universiät
require sustained treatment for several months in order
Tübingen, Dr. Fuxius, Heidelberg, Prof. Dr. Kersting, Ev Stift St.
to achieve a hematologic remission. For those patients
who respond slowly in the first months of treatment
Essex Pharma provided the pegylated interferon free of chargefor this trial. Our department received an unrestricted educational
with pegylated interferon, concomitant cytoreductive
grant for the documentation work of this study. The data are owned
therapy with hydroxyurea might help to achieve a
by the main investigator and study participants and were evaluat-
more effective platelet count reduction. ed and analyzed by the principal investigator (MG).Manuscript received May 14, 2005. Accepted August 8, 2005References
16. Saba R, Jabbour E, Giles F, Cortes J,
1. Johansson P, Kutti J, Andreasson B, Safai-
Kutti S, Vilen L, Wedel H, et al. Trends in
Wheatley K, East CL, Bareford D, et al.
in high-risk essential thrombocythemia.
erative disorders in the city of Goteborg,
10. Nand S, Stock W, Godwin J, Fisher SG.
2. Besses C, Cervantes F, Pereira A, Florensa
L, Sole F, Hernandez-Boluda JC, et al.
Major vascular complications in essential
Thomas D, Faderl S, Estrov Z, et al. Pilot
tive factors in a series of 148 patients.
Demory JL, Caulier MT, Wattel E, et al.
19. Samuelsson J, Hasselbalch H, Bruserud
4. Cortelazzo S, Viero P, Finazzi G, D’Emi-
Phase II Trial of Pegylated Interferon a-
and risk factors for thrombotic complica-
5. Barbui T, Barosi G, Grossi A, Gugliotta L,
Liberato LN, Marchetti M, et al. Practice
20. Gugliotta L, Bulgarelli S, Tieghi A, Asioli
S, Gardini G, Vianelli N, et al. Bone mar-
Italian Society of Hematology, the Italian
Capnist G, Chisesi T, Finelli C, et al.
Acute leukemia in polycythemia vera.
An analysis of 1,638 patients enrolled in
21. Griesshammer M, Klippel S, Strunck E,
6. Tefferi A, Murphy S. Current opinion in
Temerinac S, Mohr U, Heimpel H, et al.
treatment of essential thrombocythemia.
7. Spivak JL, Barosi G, Tognoni G, Barbui T,
15. Bentley M, Taylor K, Grigg A, Kronen-
Bench AJ, Meinhardt G, Mohr U, et al.
Vestri O, Galli M, Rodeghiero F, et al.
| 1338 | haematologica/the hematology journal | 2005; 90(10)
Paragliding Vedere il mondo di sopra-e` una sensazione assolutamente nuova. Planare per il cielo con il paracadute e` un’avventura. Vedrete l’Armenia di sopra con una delle nostre spedizioni di paragliding, con la guida degli unici paragliders in Caucaso, licenzati dalla FAA che vi garantisce un’avventura allegra e senza pericolo. Se anche mai avete volato il panorama dell’A
« Economist Debate on Regulation: Scholes vs Stiglitz | Main | Wall Street Rug » Andrew Lahde: Goodbye! Friday, October 17, 2008 | 04:00 PM in Hedge Funds | Psychology/Sentiment Now, this is how you close a fund! Andrew Lahde, manager of a small California hedge fund, Lahde Capital, burst into the spotlight last year after his one-year-old fund returned 866% betting on the subprime col
 (500-1000 mg) was recommended approximately 30minutes before administration of the pegylated inter-
feron to reduce flu-like symptoms. The use of low
dose aspirin (100 mg/day) was optional and at the dis-
cretion of the attending physician. No other cytoreduc-
tive therapy was permitted while the patient was in
le
(500-1000 mg) was recommended approximately 30minutes before administration of the pegylated inter-
feron to reduce flu-like symptoms. The use of low
dose aspirin (100 mg/day) was optional and at the dis-
cretion of the attending physician. No other cytoreduc-
tive therapy was permitted while the patient was in
le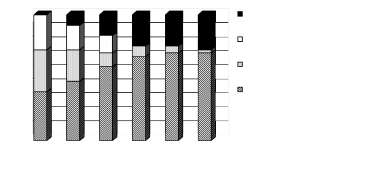 Discontinuation of pegylated interferon
Discontinuation of pegylated interferon