Copyright � The Korean Academy
Inflammatory Myofibroblastic Tumor on Intercostal Nerve Presentingas Paraneoplastic Pemphigus with Fatal Pulmonary Involvement
Inflammatory myofibroblastic tumors (IMTs) are benign neoplasms that can occur
at different anatomic sites with nonspecific clinical symptoms. A 48-yr-old woman
presented with a 2-month history of a relapsed oral ulcer, progressive dyspnea, and
Department of Neurosurgery, School of Medicine,
a thoracic pain induced by breathing. A tumorous mass was noticed in the right
Kyungpook National University, Daegu, Korea
costodiaphragmatic recess on chest computed tomography and magnetic reso-nance imaging, and the patient underwent a right costotransversectomy with exci-sion of the tumor, which originated from the 12th intercostal nerve. Histology andimmunohistochemistry showed that the tumor was an IMT of the intercostal nerve. The patient’s postoperative course was not favorable; dyspnea persisted after sur-
Received : 6 March 2006Accepted : 16 June 2006
gery, and a progressive pulmonary compromise developed. The cause of the res-piratory failure was found to be bronchiolitis obliterans, which in this case provedto be a fatal complication of paraneoplastic pemphigus associated with an IMT. This case of IMT of the spinal nerve in the paravertebral region is unique in terms
of its location and presentation in combination with paraneoplastic pemphigus,
which is rare. A brief review of the heterogeneous theories concerning the patho-
Department of Neurosurgery, School of Medicine,
genesis, clinicopathological features, and differential diagnosis of this disease enti-
Kyungpook National University, 50 Samduk-2-ga,
Jung-gu, Daegu 700-721, KoreaTel : +82.53-420-5649, Fax : +82.53-423-0504
Key Words : Inflammatory Myofibroblastic Tumor; Intercostal Nerves; Paraneoplastic PemphigusINTRODUCTION CASE REPORT
Inflammatory myofibroblastic tumors (IMTs) are benign
A 48-yr-old woman presented with a 1-month history of
tumor-like lesions of unknown etiology that can occur at dif-
progressive dyspnea and pleuritic pain in the right lower
ferent anatomic sites and have variable non-specific clinical
chest, and also a thoracic back pain of 1-month duration.
symptoms. Moreover, this variability has led to a heteroge-
There was no history of trauma. She had a history of a chro-
neous nomenclature. Plasma-cell granuloma, inflammatory
nic relapsing oral ulcer, and had been admitted to the Depart-
pseudotumor, fibrous xanthoma, histiocytoma, and mast-cell
ment of Internal Medicine at our institution 3 months earli-
granuloma are among the terms most frequently used as
er due to a fever and multiple oral ulcers (Fig. 1A), the lat-
pathomorphologic descriptions (1). The common sites of
ter of which had been diagnosed as pemphigus vulgaris by
this lesion are the lung (the originally described location),
biopsy. However, unfortunately, several examinations failed
respiratory tract, gastrointestinal tract, orbit, liver, spleen,
to detect the exact origin of the fever. After discharge, she
lymph nodes, heart, and brain (2, 3). Seven cases of intras-
had been treated with prednisolone and azathiopurine for 3
pinal IMT have been reported (4, 5), and only five cases of
IMT involving peripheral nerves have been previously des-
When she was readmitted, physical examination revealed
cribed (6, 7). Although imaging techniques have made evi-
an oral ulcer, multiple blisters and erythematous papules on
dent progress, they cannot be used for a preoperative diag-
trunk skin (Fig. 1B). All laboratory tests, including WBC
nosis of IMT, and only histological examinations are capable
count, RBC count, erythrocyte sedimentation rate, C-reac-
of identifying its inflammatory character.
tive protein, and hemoglobin level were normal, as well as
This paper describes an IMT of the intercostal nerve, a pre-
plain chest and spine radiographs. However, computed tomo-
viously unreported location, in combination with paraneo-
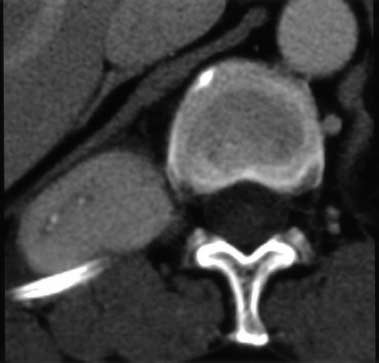
graphy (CT) with intravenous contrast visualized a clearly
plastic pemphigus (PNP), in a 48-yr-old woman, and includes
demarcated paraspinal mass with homogeneous enhancement
a discussion of its clinicopathological features and diagnosis.
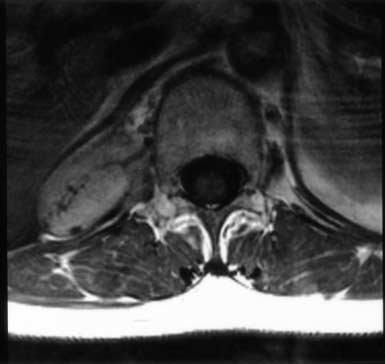
in the right costodiaphragmatic recess (Fig. 2A). Magneticresonance imaging showed an extradural and paraspinal ellip-
soidal mass at the T12 level extending into the spinal fora-
cumscribed tumor of 5×3×4 cm3 originating from the
men. Large vessels were present at the center of the mass
proximal part of the 12th intercostal nerve, but not infiltrat-
(Fig. 2B). In view of her progressive symptoms, she was trans-
ing the nerve grossly, was found to be bulging into the right
ferred to the Neurosurgery Department for further evalua-
thoracic cavity. The mass was removed en-bloc with a portion
tion and treatment. Under the differential diagnosis for the
of the parietal pleura. No involvement of any adjacent organ
mass including schwannoma, osteogenic sarcoma, chondro-
(lung, diaphragm, or vertebra) was found after complete exci-
sarcoma, or metastasis, we approached via costotransversec-
sion. Biopsy specimens showed proliferation of a heteroge-
tomy and resected it completely. Intraoperatively, a well cir-
neous population of inflammatory cells, including macro-
Fig. 1. (A) Erosions of the vermilion border, tongue, and buccal mucosa. (B) Multiple erythematous papules on trunk skin.
Fig. 2. (A) Contrast-enhance abdominal CT revealing a solitary paraspinal soft tissue mass with homogeneous attenuation in the posterioraspect of the right hemithorax. The mass displaced the right lower lobe superiorly. (B) Enhanced T1-weighted magnetic resonance axialsection through the disc at T12-L1 showing the mass and its large vessels. Vertebra and ribs were not eroded, and adjacent organs (liver,diaphragm, and thecal sac) were not involved by the mass.
IMT Presenting as Paraneoplastic Pemphigus
phages, lymphocytes, and neutrophils with peripheral fibro-
nal Medicine, and a repeat biopsy of an oral ulcer and direct
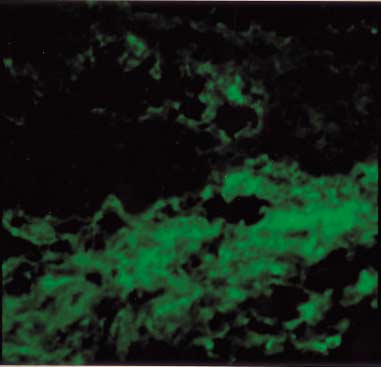
sis (Fig. 3A). Immunohistochemically, all were negative for
tissue immunofluorescence showed intracellular IgG and
S100, leu7, and SMA, but positivity for CD3 and CD20
complement C3 deposition within the epidermis (Fig. 3B).
indicated the presence of both mature B and T lymphocytes.
Finally, she was diagnosed as having PNP combined with
The final histological diagnosis was IMT.
bronchiolitis obliterans. She was continued on respiratory
Pleuritic pain improved progressively after surgery, but
therapy and with prednisone, cyclosporine, and intravenous
dyspnea persisted and a progressive pulmonary compromise
immunoglobulins. During the following months progressive
developed. She was retransferred to the Department of Inter-
dyspnea slightly improved after intravenous immunoglobu-
Fig. 3. Histology of tumor samples resected during operation. (A) Photomicrograph showing an admixture of spindle-shaped ovoid cellsand a conspicuous admixture of lymphocytes and plasma cells (H&E, ×400). (B) Direct immunofluorescence showed IgG deposits inthe basement membrane zone and epithelial layer in this biopsy specimen of ulcerated oral mucosa.
Table 1. Inflammatory myofibroblastic tumor of peripheral nerves: a review of the literature
Mass involving geniculate Resection of mass
2-yr progression of idiopathic Fusiform 16×2 cm
Resection of epineurium- Neurological recovery &
based lesion with sparing no evidence of recurrence
Mass affecting left greater Resection with segment
& hypesthesia in 1st 3 fingers mass infiltrating fascicles infiltrated fascicles
Present study 48/F Intercostal 1-mon pleuritic pain in right
Resection of epineurium- Pain decreased but expired
portion of parietal pleura with paraneoplastic
lins therapy, as did the skin and mucosal lesion. However, 3
tion with a complex of four proteins (desmoplakin I, BP Ag,
months after the operation she was readmitted to the inten-
envoplakin and desmoplakin II, and periplakin), whereas
sive care unit for progressive dyspnea. Unfortunately methyl-
minor signs include histologic evidence of acantholysis in
prednisolone and cyclosporin was ineffective, and she died
erythematous lichenoid papules, DIF findings of basement
membrane and intercellular epidermal IgG and C3, and IIFstaining of the rat bladder epithelium. Three major signs,or two major and two minor signs are required to diagnose
DISCUSSION
Several cases of PNP, including one case of IMT, which
The clinicopathological features of IMTs described in the
resulted in respiratory failure caused by airway obliteration,
literature as originating from the peripheral nerve are sum-
have been reported (19, 20). Moreover, after the onset of res-
marized in Table 1. The present case, an IMT that originat-
piratory failure, autoantibody reaction against plakins detect-
ed from the intercostal nerve in the paravertebral region, is
ed by serum immunoprecipitation at the onset of PNP, dis-
unique in terms of its location. IMTs are typically composed
appeared as determined by immunofluorescence of the bron-
of variable amounts of stromal and cellular elements, and
chial epithelium. Based on the above-mentioned findings,
myofibroblasts, which are involved in tissue repair, are now
it is postulated that autoantibodies against some of these
recognized as the principal cell type (4, 8). The precise eti-
antigens play a causative role in acute respiratory epithelial
ology of IMT is unknown. In some cases, they are consid-
inflammation (20). Moreover, when treating PNP the lethal
ered to result from inflammation following minor trauma
complication of bronchiolitis obliterans should be kept in
or surgery or to be associated with another malignancy (9,
mind. Furthermore, the prevention of autoantibody-medi-
10). Some authors believe that this tumor is a low-grade
ated injury to the respiratory epithelium should be an impor-
fibrosarcoma that contains inflammatory (lymphomatous)
tant treatment goal. Early diagnosis and tumor removal before
cells. Immunohistochemical studies of T- and B-cell subpop-
respiratory involvement are essential because of the typically
ulations may be helpful for differentiating IMT and lym-
poor response to immunosuppressive therapy shown in PNP.
phoma. An immune-autoimmune mechanism has also beenimplicated for the etiology of IMT. Many of the features ofIMTs can be related to the production of inflammatory me-
REFERENCES
diators, such as cytokines, particularly interleukin-1 (11). Locally, IMTs stimulate the proliferation of fibroblasts, the
1. Narla LD, Newman B, Spottswood SS, Narla S, Kolli R. Inflamma-
extravasation of neutrophils, and the activation and eleva-
tory pseudotumor. Radiographics 2003; 23: 719-29.
tion of vascular endothelium procoagulant activity (12).
2. Anthony PP. Inflammatory pseudotumour (plasma cell granuloma)
Complete surgical resection, if possible, is the treatment
of lung, liver and other organs. Histopathology 1993; 23: 501-3.
of choice for most IMTs, with the exception of orbital lesions
3. Dehner LP. The enigmatic inflammatory pseudotumors: the current
(13-16), and this approach may be successful in cases of recur-
state of our understanding, or misunderstanding (editorial). J Pathol
rence. Meanwhile, some authors have reported spontaneous
regression (17, 18), and successful radiation therapy in unre-
4. Despeyroux-Ewers M, Catalaa I, Collin L, Cognard C, Loubes-La-
sectable cases. Chemotherapy has also been used, but gener-
croix F, Manelfe C. Inflammatory myofibroblastic tumour of the
ally had had minimal effect, and although response to ste-
spinal cord: case report and review of the literature. Neuroradiolo-
roids is often unpredictable, they remain the primary treat-
5. Kim YO, Cho YJ, Ahn SK, Hwang JH, Ahn MS, Choi YH. Inflam-
Our patient developed progressive airflow obstruction in-
matory pseudotumor of the thoracic spinal cord meninges: A case
duced by undiagnosed PNP and this resulted in respiratory
report. J Korean Neurosurg Soc 1998; 27: 1419-23.
failure. PNP (19, 20) is an autoantibody-mediated mucocu-
6. Perez-Lopez C, Gutierrez M, Isla A. Inflammatory pseudotumor of
taneous blistering disease, which is associated with underly-
the median nerve: case report and review of the literature. J Neuro-
ing neoplasms (hematologic-related neoplasms, sarcoma, and
benign tumors such as Castleman tumors and IMT). Since
7. Weiland TL, Scheithauer BW, Rock MG, Sargent JM. Inflammato-
PNP was first described in 1990 by Anhalt et al. (21), approx-
ry pseudotumor of nerve. Am J Surg Pathol 1996; 20: 1212-8.
imately 60 cases have been reported, and the diagnostic cri-
8. Mountney J, Suvarna SK, Brown PW, Thorpe JA. Inflammatory
teria include clinical findings, histologic, direct immunoflu-
pseudotumour of the lung mimicking thymoma. Eur J Cardiothorac
orescence (DIF), indirect immunofluorescence (IIF), and im-
munoprecipitation test. The criteria were later revised by
9. Maves CK, Johnson JF, Bove K, Malott RL. Gastric inflammatory
Camisa and Helm (22) and divided into major and minor
pseudotumor in children. Radiology 1989; 173: 381-3.
signs. Major signs are polymorphic mucocutaneous eruption,
10. Sanders BM, West KW, Gingalewski C, Engum S, Davis M, Gros-
concurrent internal neoplasia, and serum immunoprecipita-
feld JL. Inflammatory pseudotumor of the alimentary tract: clinical
IMT Presenting as Paraneoplastic Pemphigus
and surgical experience. J Pediatr Surg 2001; 36: 169-73.
17. Maier HC, Sommers SC. Recurrent and metastatic pulmonary fibrous
11. Hytiroglou P, Brandwein MS, Stauchen JA, Mirante JP, Urken ML,
histiocytoma/plasma cell granuloma in a child. Cancer 1987; 60:
Biller HF. Inflammatory pseudotumor of the parapharyngeal space:case report and review of the literature. Head Neck 1992; 14: 230-4.
18. Pearson PJ, Smithson WA, Driscoll DJ, Banks PM, Ehman RL. Inop-
12. Coffin CM, Watterson J, Priest JR, Dechner LP. Extrapulmonaryerable plasma cell granuloma of the heart: spontaneous decrease ininflammatory myofibroblastic tumor (inflammatory pseudotumor):size during an 11-month period. Mayo Clin Proc 1998; 63: 1022-5.a clinicopathologic and immunohistochemical study of 84 cases. Am
19. Mar WA, Glaesser R, Struble K, Stephens-Groff S, Bangert J, Han-
sen RC. Paraneoplastic pemphigus with bronchiolitis obliterans in
13. Jenkins PC, Dickison AE, Flanagan MF. Cardiac inflammatory pseu-a child. Pediatr Dermatol 2003; 20:238-42.dotumor: rapid appearance in an infant with congenital heart dis-
20. Takahashi M, Shimatsu Y, Kazama T, Kimura K, Otsuka T, Hashi-
ease. Pediatr Cardiol 1996; 17: 399-401.
moto T. paraneoplastic pemphigus associated with bronchiolitis oblit-
14. Martin CJ. Orbital pseudotumor: case report and overview. J Am
21. Anhalt GJ, Kim SC, Stanley JR, Korman NJ, Jabs DA, Kory M. Para-
15. Rose AG, McCormick S, Cooper K, Titus JL. Inflammatory pseu-neoplastic pemphigus. An autoimmune mucocutaneous disease asso-dotumor (plasma cell granuloma) of the heart. Pathol Lab Med 1996;ciated with neoplasia. N Engl J Med 1990; 323: 1729-35.
22. Camisa C, Helm TN. Paraneoplastic pemphigus is a distinct neopla-
16. Scott L, Blair G, Taylor G, Dimmick J, Fraser G. Inflammatory pseu-sia-induced autoimmune disease. Arch Dermatol 1993; 129: 883-6. dotumors in children. J Pediatr Surg 1988; 23: 755-8.
CURRICULUM VITAE ROBERT ALAN RINGEL, M.D. DEGREES HELD POSITIONS HELD Curriculum Vitae – Robert Alan Ringel, MD ACADEMIC RESPONSIBILITIES AND ENDEAVORS Director, Electroencephalography Laboratory, West Virginia University Hospitals, Inc., 1986 – 1988 CPR Committee, West Virginia University Hospitals, Inc. Neurointensive Care Unit Committee, West Virginia Univ
Clinical staff use only: If PA Assessment by RN was required tick sign_____________Director of Nursing sign___________ This centre is owned and operated by Dr M. Stergoulis, Dr J. Cannon & Dr A. Theodore email: [email protected] Please answer ALL questions, printing clearly, and RETURN THE FORM TO THE DAY SURGERY AT LEAST ONE WEEK PRIOR TO YOUR ADMISSION. All informa


 soidal mass at the T12 level extending into the spinal fora-
cumscribed tumor of 5×3×4 cm3 originating from the
men. Large vessels were present at the center of the mass
proximal part of the 12th intercostal nerve, but not infiltrat-
(Fig. 2B). In view of her progressive symptoms, she was trans-
ing the nerve grossly, was found to be bulging into the right
ferred to the Neurosurgery Department for further evalua-
thoracic cavity. The mass was removed en-bloc with a portion
tion and treatment. Under the differential diagnosis for the
of the parietal pleura. No involvement of any adjacent organ
mass including schwannoma, osteogenic sarcoma, chondro-
(lung, diaphragm, or vertebra) was found after complete exci-
sarcoma, or metastasis, we approached via costotransversec-
sion. Biopsy specimens showed proliferation of a heteroge-
tomy and resected it completely. Intraoperatively, a well cir-
neous population of inflammatory cells, including macro-
Fig. 1. (A) Erosions of the vermilion border, tongue, and buccal mucosa. (B) Multiple erythematous papules on trunk skin.
soidal mass at the T12 level extending into the spinal fora-
cumscribed tumor of 5×3×4 cm3 originating from the
men. Large vessels were present at the center of the mass
proximal part of the 12th intercostal nerve, but not infiltrat-
(Fig. 2B). In view of her progressive symptoms, she was trans-
ing the nerve grossly, was found to be bulging into the right
ferred to the Neurosurgery Department for further evalua-
thoracic cavity. The mass was removed en-bloc with a portion
tion and treatment. Under the differential diagnosis for the
of the parietal pleura. No involvement of any adjacent organ
mass including schwannoma, osteogenic sarcoma, chondro-
(lung, diaphragm, or vertebra) was found after complete exci-
sarcoma, or metastasis, we approached via costotransversec-
sion. Biopsy specimens showed proliferation of a heteroge-
tomy and resected it completely. Intraoperatively, a well cir-
neous population of inflammatory cells, including macro-
Fig. 1. (A) Erosions of the vermilion border, tongue, and buccal mucosa. (B) Multiple erythematous papules on trunk skin.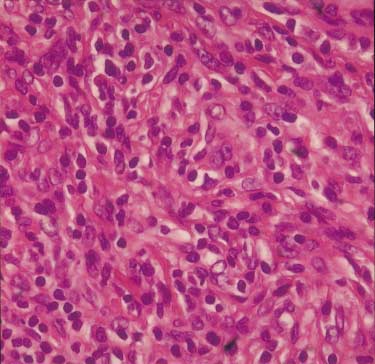
 IMT Presenting as Paraneoplastic Pemphigus
phages, lymphocytes, and neutrophils with peripheral fibro-
nal Medicine, and a repeat biopsy of an oral ulcer and direct
sis (Fig. 3A). Immunohistochemically, all were negative for
tissue immunofluorescence showed intracellular IgG and
S100, leu7, and SMA, but positivity for CD3 and CD20
complement C3 deposition within the epidermis (Fig. 3B).
IMT Presenting as Paraneoplastic Pemphigus
phages, lymphocytes, and neutrophils with peripheral fibro-
nal Medicine, and a repeat biopsy of an oral ulcer and direct
sis (Fig. 3A). Immunohistochemically, all were negative for
tissue immunofluorescence showed intracellular IgG and
S100, leu7, and SMA, but positivity for CD3 and CD20
complement C3 deposition within the epidermis (Fig. 3B).