Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Nutrifisio.com.br2
GUIDELINES NEUROGENIC LOWER URINARY DYSFUNCTION M. Stöhrer, D. Castro-Diaz, E. Chartier-Kastler, G. Kramer, A. Mattiasson, J.J. Wyndaele TABLE OF CONTENTS
Dementia (Alzheimer, Binswanger, Nasu, Pick)
Guideline for timing of diagnosis and treatment
Guidelines for urodynamics and uro-neurophysiology
Guidelines for non-invasive conservative treatment
Guidelines for minimal invasive treatment
Denervation. deafferentation, neurostimulation, neuromodulation
1. AIM AND STATUS OF THESE GUIDELINES
The purpose of these clinical guidelines is to provide information on the incidence, definitions, diagnosis,therapy, and follow up observation of the condition of neurogenic lower urinary tract dysfunction (NLUTD), thatwill be useful for clinical practitioners. These guidelines reflect the current opinion of the experts in this specificpathology and thus represent a state of the art reference for all clinicians as of the date of its presentation tothe European Association of Urology. Standardization
The terminology used and the diagnostic procedures advised throughout these guidelines follow therecommendations for investigations on the lower urinary tract (LUT) as published by the InternationalContinence Society (ICS) (1-3). References
Stöhrer M, Goepel M, Kondo A, Kramer G, Madersbacher H, Millard R, Rossier A, Wyndaele JJ. The standardization of terminology in neurogenic lower urinary tract dysfunction with suggestions fordiagnostic procedures, Neurourol Urodyn 1999; 18:139-158.
Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, van Kerrebroeck P, Victor A, Wein A. The standardisation of terminology of lower urinary tract function: Report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn 2002; 21: 167-178.
Schäfer W, Abrams P, Liao L, Mattiasson A, Pesce F, Spångberg A, Sterling AM, Zinner NR, vanKerrebroeck P. Good Urodynamic Practices: Uroflowmetry, Filling Cystometry, and Pressure-FlowStudies. Neurourol Urodyn 2002; 21: 261-274. 2. BACKGROUND Risk factors and epidemiology
NLUTD may be caused by various diseases and events affecting the nervous systems controlling the LUT. Theresulting lower urinary tract dysfunction (LUTD) depends grossly on the location and the extent of theneurologic lesion (cf. 2.3.). Overall figures on the prevalence of NLUTD in the general population are lacking, but data are available on theprevalence of the underlying conditions and the relative risk of those for the development of NLUTD.
Diabetes: This common metabolic disorder has a prevalence of about 2.5% in the American population, but thedisease may be subclinical for many years. No specific criteria exist for secondary neuropathy in this condition,but it is generally accepted that 50% of the patients will develop somatic neuropathy and 75-100% of thosewill develop NLUTD (1-2).
Alcohol abuse: This will eventually cause peripheral neuropathy, but its reported prevalence varies widely: 5-15% (3) to 64% (4). The NLUTD is probably more present in patients with liver cirrhosis and theparasympathetic system is attacked more than the sympathetic system (5).
Less prevalent peripheral neuropathies:- Porphyria — bladder dilatation in up to 12% of patients (6). - Sarcoidosis — NLUTD rare (7). - Lumbosacral (8) zone and genital (9) herpes — NLUTD transient in most patients. - Guillain Barré — Urinary symptoms in 30% of patients, regressive in most (10).
This may cause NLUTD (11) but no prevalence figures were found (12).
Abdominoperineal resection of rectum or uterus may cause lesions of the lower urinary tract innervation in 10-60% of patients (13,14). The extent of the resection is important: <8% after colostomy only, but 29% afterposterior resection (15). Radical prostectomy is a risk factor also (16).
Multiple sclerosis causes NLUTD in 50-90% of the patients (17-19). NLUTD is the presenting symptom in 2-12% of the patients (20).
Alzheimer, Binswanger, Nasu and Pick diseases frequently cause non-specific NLUTD (21-25). Basal ganglia pathology (Parkinson, Huntington, Shy-Drager, etc.)
Parkinson’s disease is accompanied by NLUTD in 37.9-70% (26). In the rare Shy-Drager syndrome almost allpatients have NLUTD (27).
This causes hemiplegia with remnant incontinence NLUTD in 20-50% of patients (28 - 30) with decreasingprevalence in the post-insult period (30).
These tumours can cause LUTD in 24% of the patients (31).
Spinal cord lesions can be traumatic, vascular, medical, or congenital. An incidence of 30-40 new cases permillion population is the accepted average for the USA. Most patients will develop NLUTD (32). For spina bifidaand other congenital nerve tube defects, the prevalence in the UK is 8-9 per 10,000 aged 10-69 years with thegreatest prevalence in the age group 25-29 years (33), and in the USA 1 per 1000 births (34). About 50% ofthese children will have detrusor sphincter dyssynergia (DSD) (35). 2.1.10 Disc diseaseThis is reported to cause NLUTD in 6-18% of the patients (36, 37). Standardization of terminology
Several groups already presented guidelines for the care of patients with NLUTD for national or internationalurological community (38-41).These guidelines will evolve further as time goes by. They also contain definitionsof various important terms and procedures. The ICS NLUTD standardization report (39) is addressedspecifically at the standardization of terminology and urodynamic investigation in this patient group. Otherrelevant definitions are found in the general ICS standardization report (42). The definitions from these references, partly adapted, and other definitions that are judged useful for the clinicalpractice in NLUTD, are listed in section 2.2.2. For specific definitions relating to the urodynamic investigationtechnique the reader is referred to the appropriate ICS report (39).
Acontractility, detrusor — see below under voiding phaseAcontractility, urethral sphincter — see below under storage phaseAutonomic dysreflexia — Increase of sympathetic reflex due to noxious stimuli with symptoms or signs of
headache, hypertension, flushing face and perspiration
Capacity — see below under storage phaseCatheterization, indwelling — Emptying of the bladder by a catheter that is introduced (semi-)permanently Catheterization, intermittent (IC) — Emptying of the bladder by a catheter that is removed after the procedure,
mostly at regular intervals- Aseptic IC — The catheters remain sterile, the genitals are disinfected, and disinfecting lubricant is used- Clean IC — Disposable or cleansed re-usable catheters, genitals washed- Sterile IC — Complete sterile setting, including sterile gloves, forceps, gown and mask- Intermittent self-catheterization (ISC) — IC performed by the patient
Compliance, detrusor — see below under storage phaseCondition — The presence of specific observations associated with characteristic symptoms or signs
Diary, urinary — Record of times of micturitions and voided volumes, incontinence episodes, pad usage, and
other relevant information- Frequency volume chart (FVC) — Times of micturitions and voided volumes only- Micturition time chart (MTC) — Times of micturitions only
Filling rate, physiological — Below the predicted maximum: body weight [kg]/4 in ml/s (42, 43)
Hesitancy — Difficulty in initiating micturition; delay in the onset of micturition after the individual is ready to
Intermittency — Urine flow stops and starts on one or more occasions during voidingLeak point pressure (LPP) — see below under storage phaseLower motor neuron lesion (LMNL) — Lesion at or below the S1-S2 spinal cord level Neurogenic lower urinary tract dysfunction (NLUTD) — Lower urinary tract dysfunction secondary to confirmed
Observation, specific — Observation made during specific diagnostic procedureOveractivity, bladder — see below under symptom syndromeOveractivity, detrusor — see below under storage phaseRehabilitation, LUT — Non-surgical non-pharmacological treatment for LUT dysfunctionSign — Observation by the physician including simple means (direct observation, bladder diary, pad weighing)
Sphincter, urethral, non-relaxing — see below under voiding phaseSymptom — Subjective indicator of a disease or change in condition as perceived by the patient, carer, or
partner that may lead to seek help from health care professionals
Upper motor neuron lesion (UMNL) — Lesion above the S1-S2 spinal cord levelVoiding, balanced — In patients with NLUTD: voiding with physiologic detrusor pressure and low residual (<80
Voiding, triggered — Voiding initiated by manoeuvres to elicit reflex detrusor contraction by exteroceptive stimuliVolume, overactivity — see below under storage phase
Maximum anaesthetic bladder capacity — Maximum bladder filling volume under deep general or spinalanaesthesia
Increased daytime frequency — Self-explanatory; the normal frequency can be estimated at about 8times per day (44)
Nocturia — Waking at night one or more times to void
Urgency — The symptom of a sudden compelling desire to pass urine which is difficult to defer
Urinary incontinence — Any involuntary leakage of urine. This can be specified:- Stress urinary incontinence — On effort or exertion, or on sneezing or coughing- Urge urinary incontinence — Accompanied by or immediately preceded by urgency- Mixed urinary incontinence — Associated with urgency and also exertion, effort, sneezing, or coughing- Continuous urinary incontinence
Bladder sensation categorized as:- Normal — Symptom and history: Awareness of bladder filling and increasing sensation up to a strongdesire to void. Urodynamics: First sensation of bladder filling, first desire to void, and strong desire to void at realistic bladder volumes. - Increased — Symptom and history: An early and persistent desire to void.
Urodynamics: Any of the three urodynamic parameters mentioned under “normal” persistently at low bladder volume
- Reduced — Symptom and history: Awareness of bladder filling but no definite desire to void.
Urodynamics: Diminished sensation throughout bladder filling
- Absent — No sensation of bladder filling or desire to void- Non-specific — Perception of bladder filling as abdominal fullness, vegetative symptoms, or spasticity
Definitions valid after urodynamic confirmation only•
Cystometric capacity — Bladder volume at the end of the filling cystometry
Maximum cystometric capacity — Bladder volume at strong desire to void
High capacity bladder — Bladder volume at cystometric capacity far over the mean voided volume,
estimated from the bladder diary, with no significant increase in detrusor pressure under non-anaesthetized condition
Normal detrusor function — Little or no pressure increase during filling: no involuntary phasic
Detrusor overactivity — Involuntary detrusor contractions during filling; spontaneous or provokedSubgroups:- Phasic detrusor overactivity — Characteristic phasic contraction- Terminal detrusor overactivity — A single contraction at cystometric capacity
High pressure detrusor overactivity — Maximal detrusor pressure >40 cm H2O (39,45)
Overactivity volume — Bladder volume at first occurrence of detrusor overactivity
Detrusor overactivity incontinence — Self-explanatory
Leak point pressure- Detrusor leak point pressure (DLPP) — Lowest value of detrusor pressure at which leakage is
observed in the absence of abdominal strain or detrusor contraction
- Abdominal leak point pressure — Lowest value of intentionally increased intravesical pressure that
provokes leakage in the absence of a detrusor contraction
Detrusor compliance — Relationship between change in bladder volume (∆V) and change in detrusor
pressure (∆pdet): C=∆V/∆pdet [ml/cm H2O]
Low detrusor compliance — C=∆V/∆pdet <20 ml/cm H2O (39)
Break volume — Bladder volume after which a sudden significant decrease in detrusor compliance is
Urethral sphincter acontractility — No evidence of sphincter contraction during filling, particularly at
higher bladder volumes, or during abdominal pressure increase
Intermittent stream (intermittency) — Stopping and starting of urine flow during micturition
Hesitancy — Difficulty in initiating micturition
Straining — Muscular effort to initiate, maintain, or improve urinary stream
Terminal dribble — Prolonged final part of micturition when the flow has slowed to a trickle/dribble
Definitions valid after urodynamic confirmation only•
Normal detrusor function — Voluntarily initiated detrusor contraction that causes complete bladder
Detrusor underactivity — Contraction of reduced strength and/or duration
Acontractile detrusor — Absent contraction
Non-relaxing urethral sphincter — Self-explanatory
Detrusor sphincter dyssynergia (DSD) — Detrusor contraction concurrent with an involuntary
contraction of the urethral and/or periurethral striated musculature
Feeling of incomplete emptying (symptom only)
Post micturition dribble - Involuntary leakage of urine shortly after finishing the micturition
Pain, discomfort or pressure sensation in the lower urinary tract and genitalia that may be related to bladderfilling or voiding, may be felt after micturition, or be continuous
Symptom syndrome - Combination of symptoms•
Overactive bladder syndrome — Urgency with or without urge incontinence, usually with frequency andnocturia
Synonyms: Urge syndrome, urgency-frequency syndromeThis syndrome is suggestive for LUTD
Classification
The purpose of classification of NLUTD is to facilitate the understanding and management of NLUTD and toprovide a standardized terminology of these disease processes. The normal LUT function depends on neuralintegration at and between the peripheral, spinal cord, and central nervous systems. The gross type of NLUTDis dependent on the location and the extent of the lesion: suprapontine or pontine, suprasacral spinal cord, orsubsacral and peripheral (32,40).
The classification systems for NLUTD are based on either the neurologic substrate (type and location of
the neurologic lesion), the neuro-urologic substrate (neurologic lesion and LUTD), the type of LUTD, or are strictlyfunctional. Many descriptive terms were derived from these classification systems, but they are standardized onlywithin any specific system and have little meaning outside the system and can sometimes be confusing.
A perfect classification system is not yet available. Neurologic classification systems, by nature, cannot
describe the LUTD completely and vice versa. Individual variations exist in the NLUTD caused by a specificneurologic lesion. Thus for any particular patient the description of the NLUTD should be individualized.
Bors and Comarr’s (46) classic neuro-urologic classification system was deduced from clinical observations ofpatients with traumatic spinal cord injury. It specifies three elements: location of lesion, completeness of lesion,and co-ordination of LUT.
Hald and Bradley (47) reduced the number of categories in Bors and Comarr’s classification. The
authors describe their system as a simple neurotopographic classification.
Burgdörfer completed Bors and Comarr’s system with information on the LUTD, broken down for
detrusor, sphincter, and residual urine. This classification is published elsewhere (48).
Bradley (49) presented four control loops for the LUT. Loop I are the connections between the central nervoussystem and the pontine micturition center, loop II the intraspinal pathways between the detrusor to themicturition center (afferent) and the sacral spinal cord (efferent), loop III the sensory axons pathways from thedetrusor and the striated urethral sphincter to the sacral spinal cord, and loop IV describes the suprasacral andsegmental innervation of the periurethral striated muscles.
Lapides (50) classifies the clinical and urodynamic findings into five categories: sensory neurogenic bladder,motor paralytic bladder, autonomous neurogenic bladder, uninhibited neurogenic bladder, and reflexneurogenic bladder.
Krane and Siroky (51) present a descriptive classification of detrusor and sphincter co-ordination
observed during urodynamic evaluation in patients with NLUTD, focussed on the functional interaction betweendetrusor and urethral sphincter.
Quesada et al. (52) suggested that a classification based on the functional aspects of the LUT might be morepracticable for clinical decision making.
Wein (53) provides a practical approach towards the diagnosis and therapy of LUTD by classifying
against the storage and voiding functions of the LUT, and the activity of the detrusor and the urethra.
Fall et al. (54) proposed a more detailed classification of the overactive detrusor. This is included in the
The ICS (42) separates the storage and voiding phases and describes the detrusor and urethral
functions in each phase by specific designations (cf. 2.2.).
Madersbacher (40,55) presented a very simple classification that basically is focussed on the
therapeutic consequences (fig. 2.1). It is based on the clinical concept that the important differentiation in thediagnosis exists between the situations of high and low detrusor pressure during the filling phase and urethralsphincter relaxation and non- relaxation or DSD during the voiding phase. A non-relaxed sphincter or DSD willcause high detrusor pressure during the voiding phase. This classification is the easiest one for general use inclinical diagnosis of NLUTD. Detrusor Urethral sphincter Lesion: Spinal Detrusor Urethral sphincter Lesion:Subsacral Figure 2.1. Madersbacher classification system (40) with typical neurogenic lesions
The Madersbacher classification system (40) (fig. 2.1) is recommended for clinical practice. Timing of diagnosis and treatment
Both in congenital and in acquired NLUTD, early diagnosis and treatment is essential as irreversible changesmay occur in particular in children with myelomeningocele (56-61), but also in patients with traumatic spinalcord injury (62-64), even if the related neuropathologic signs may be normal (65). The fact must also be considered that LUTD by itself may be the presenting symptom for neurologic pathology(20,66). 2.4.1 GUIDELINE FOR TIMING OF DIAGNOSIS AND TREATMENT 1.
Diagnosis and treatment in NLUTD should be performed as soon as possible. REFERENCES
Ellenberg M. Development of urinary bladder dysfunction in diabetes mellitus. Ann Intern Med 1980; 92: 321-323.
Bradley WE. Diagnosis of urinary bladder dysfunction in diabetes mellitus. Ann Intern Med 1980; 92: 323-326.
Schuckit M. In: Isselbacher KJ, et al. (eds) Harrison’s principles of Internal Medicine. New York,McGraw-Hill 1981: 1475-1478.
Barter F, Tanner AR. Autonomic neuropathy in an alcoholic population. Postgrad Med J 1987; 63: 1033-1036.
Anonymous. Autonomic neuropathy in liver disease. Lancet 1989; 2(8665): 721-722
Bloomer JR, Bonkovsky HL. The porphyrias. Dis Mon 1989; 35: 1-54.
Chapelon C, Ziza JM, Piette JC, Levy Y, Raguin G, Wechsler B, Bitker MO, Bletry O, Laplane D, BousserMG, et al. Neurosarcoidosis: signs, course and treatment in 35 confirmed cases. Medicine (Baltimore); 1990; 69: 261-276.
Chen PH, Hsueh HF, Hong CZ. Herpes zoster-associated voiding dysfunction: a retrospective study andliterature review. Arch Phys Med Rehabil 2002; 83: 1624-1628
Greenstein A, Matzkin H, Kaver I, Braf Z. Acute urinary retention in herpes genitalis infection. Urodynamic evaluation. Urology 1988; 31: 453-456.
Lichtenfeld P. Autonomic dysfunction in the Guillain-Barré syndrome. Am J Med 1971; 50: 772-780.
Mardirosoff C, Dumont L. Bowel and bladder dysfunction after spinal bupivacaine. Anesthesiology 2001; 95: 1306.
Auroy Y, Benhamou D, Bargues L, Ecoffey C, Falissard B, Mercier F, Bouaziz H, Samii K. Major
complications of regional anesthesia in France: The SOS Regional Anesthesia Hotline Service. Anesthesiology 2002; 97: 1274-1280.
Seski JC, Diokno AC. Bladder dysfunction after radical abdominal hysterectomy. Am J Obstet Gynecol 1977; 128: 643-651.
Sekido N, Kawai K, Akaza H. Lower urinary tract dysfunction as persistent complication of radicalhysterectomy. Int J Urol 1997; 4: 259-264.
Emmett JL. Treatment of vesical dysfunction after operations on rectum and sigmoid. Surg Clin North Am 1957; 37: 1009-1017.
Zermann DH, Ishigooka M, Wunderlich H, Reichelt O, Schubert J. A study of pelvic floor function pre-and postradical prostatectomy using clinical neurourological investigations, urodynamics andelectromyography. Eur Urol 2000; 37: 72-78.
Holland NJ, Wiesel-Levison P, Schwedelson ES. Survey of neurogenic bladder in multiple sclerosis. J Neurosurg Nurs 1981; 13: 337-343.
Goldstein I, Siroky MB, Sax DS, Krane RJ. Neurourologic abnormalities in multiple sclerosis. J Urol 1982; 128: 541-545.
Fowler CJ, van Kerrebroeck PE, Nordenbo A, Van Poppel H. Treatment of lower urinary tract dysfunction inpatients with multiple sclerosis. Committee of the European Study Group of SUDIMS (Sexual andUrological Disorders in Multiple Sclerosis) J Neurol Neurosurg Psychiatry 1992; 55: 986-989.
Bemelmans BL, Hommes OR, Van Kerrebroeck PE, Lemmens WA, Doesburg WH, Debruyne FM. Evidence for early lower urinary tract dysfunction in clinically silent multiple sclerosis. J Urol 1991; 145: 1219-1224.
Sugiyama T, Hashimoto K, Kiwamoto H, Ohnishi N, Esa A, Park YC, Kurita T. Urinary incontinence insenile dementia of the Alzheimer type (SDAT). Int J Urol 1994; 1: 337-340.
McGrother C, Resnick M, Yalla SV, Kirschner-Hermanns R, Broseta E, Muller C, Welz-Barth A, FischerGC, Mattelaer J, McGuire EJ. Epidemiology and etiology of urinary incontinence in the elderly. World J Urol 1998; 16 (Suppl 1): S3-S9.
Madersbacher H, Awad S, Fall M, Janknegt RA, Stohrer M, Weisner B. Urge incontinence in the elderly-supraspinal reflex incontinence. World J Urol 1998; 16 (Suppl 1): S35-S43.
Olsen CG, Clasen ME. Senile dementia of the Binswanger’s type. Am Fam Physician 1998; 58: 2068-2074.
Honig LS, Mayeux R. Natural history of Alzheimer’s disease. Aging (Milano) 2001; 13: 171-82.
Murnaghan GF. Neurogenic disorders of the bladder in Parkinsonism. Br J Urol 1961; 33:403-409.
Salinas JM, Berger Y, De La Rocha RE, Blaivas JG. Urological evaluation in the Shy Drager syndrome. J Urol 1986; 135: 741-743.
Currie CT. Urinary incontinence after stroke. Br Med J 1986; 293: 1322-1323.
Codine PH, Pellissier J, Manderscheidt JC, Costa P, Enjalbert M, Perrigot M. Les troubles urinaires aucours des hémiplegies vasculaires. In: Pellisier J (ed) Hémiplegie vasculaire et médicine de rééducation. Paris, Masson 1988: 261-269.
Barer DH. Continence after stroke: useful predictor or goal of therapy? Age Ageing 1989; 18: 183-191.
Andrew J, Nathan PW. Lesions of the anterior frontal lobes and disturbances of micturition anddefecation. Brain 1964; 87: 233 ff.
Burns AS, Rivas DA, Ditunno JF. The management of neurogenic bladder and sexual dysfunction afterspinal cord injury. Spine. 2001; 26 (Suppl): S129-S136.
Lawrenson R, Wyndaele JJ, Vlachonikolis I, Farmer C, Glickman S. A UK general practice databasestudy of prevalence and mortality of people with neural tube defects. Clin Rehabil 2000; 14: 627-630.
Selzman AA, Elder JS, Mapstone TB. Urologic consequences of myelodysplasia and other congenitalabnormalities of the spinal cord. Urol Clin North Am 1993; 20: 485-504
van Gool JD, Dik P, de Jong TP. Bladder-sphincter dysfunction in myelomeningocele. Eur J Pediatr2001; 160: 414-420.
Rosomoff HL, Johnston JD, Gallo AE, Ludmer M, Givens FT, Carney FT, Kuehn CA. Cystometry in theevaluation of nerve root compression in the lumbar spine. Surg Gynecol Obstet 1963; 117: 263-270.
Scott PJ. Bladder paralysis in cauda equina lesions from disc prolapse. J Bone Joint Surg 1965; 47:224-235.
Burgdörfer H, Heidler H, Madersbacher H, Melchior H, Palmtag H, Richter R, Richter-Reichhelm M, RistM, Rübben H, Sauerwein D, Schalkhäuser K, Stöhrer M. Leitlinien zur urologischen BetreuungQuerschnittgelähmter. Urologe A 1998; 37: 222-228.
Stöhrer M, Goepel M, Kondo A, Kramer G, Madersbacher H, Millard R, Rossier A, Wyndaele JJ. Thestandardization of terminology in neurogenic lower urinary tract dysfunction with suggestions fordiagnostic procedures, Neurourol Urodyn 1999; 18:139-158.
Madersbacher H, Wyndaele JJ, Igawa Y, Chancellor M, Chartier-Kastler E, Kovindha A. Conservativemanagement in neuropatic urinary incontinence. In: Incontinence, 2nd Edition, Abrams P, Khoury S,
Wein A (eds.), Health Publication Ltd, Plymouth, 2002: 697-754.
Castro-Diaz D, Barrett D, Grise P, Perkash I, Stöhrer M, Stone A, Vale P. Surgery for the neuropathicpatient. In: Incontinence, 2nd Edition, Abrams P, Khoury S, Wein A (eds.), Health Publication Ltd,Plymouth, 2002: 865-891.
Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, van Kerrebroeck P, Victor A, Wein A. Thestandardisation of terminology of lower urinary tract function: Report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn 2002; 21: 167-178.
Klevmark B. Natural pressure-volume curves and conventional cystometry. Scand J Urol Nephrol(Suppl) 1999; 201: 1-4.
Homma Y, Ando T, Yoshida M, Kageyama S, Takei M, Kimoto K, Ishizuka O, Gotoh M, Hashimoto T. Voiding and incontinence frequencies: variability of diary data and required diary length. NeurourolUrodyn 2002; 21: 204-209.
McGuire EJ, Cespedes RD, O’Connell HE. Leak-point pressures. Urol Clin North Am 1996; 23: 253-262.
Bors E, Comarr AE. Neurological urology. Karger, Basel 1971.
Hald T, Bradley WE. The neurogenic bladder. Williams and Wilkins, Baltimore 1982.
Stöhrer M, Kramer G, Löchner-Ernst D, Goepel M, Noll F, Rübben H. Diagnosis and treatment ofbladder dysfunction in spinal cord injury patients. Eur Urol Update Series 1994; 3: 170-175.
Bradley WE, Timm GW, Scott FB. Innervation of the detrusor muscle and urethra. Urol Clin North Am1974; 1: 3-27.
Lapides J. Neuromuscular vesical and urethral dysfunction. In: Campbell MF, Harrison JH (eds) Urology. WB Saunders, Philadelphia 1970: 1343-1379.
Krane RJ, Siroky MB. Classification of neuro-urologic disorders. In: Krane RJ, Siroky MB (eds) Clinicalneuro-urology. Little Brown, Boston 1979: 143-158.
Quesada EM, Scott FB, Cardus D. Functional classification of neurogenic bladder dysfunction. Arch Phys Med Rehabil 1968; 49: 692-697.
Wein AJ. Pathophysiology and categorization of voiding dysfunction. In: Walsh PC, Retik AB, VaughanJr ED, Wein AJ (eds) Campbell’s Urology 7th Edition. WB Saunders, Philadelphia 1998: 917-926.
Fall M, Ohlsson BL, Carlsson CA. The neurogenic overactive bladder. Classification based onurodynamics. Br J Urol 1989; 64: 368-373.
Madersbacher H. The various types of neurogenic bladder dysfunction: an update of current therapeuticconcepts. Paraplegia 1990; 28: 217-229.
Cass AS, Luxenberg M, Johnson CF, Gleich P. Incidence of urinary tract complications withmyelomeningocele. Urology 1985; 25: 374-378.
Fernandes ET, Reinberg Y, Vernier R, Gonzalez R. Neurogenic bladder dysfunction in children: Review ofpathophysiology and current management. J Pediat 1994; 124: 1-7.
Stone AR. Neurourologic evaluation and urologic management of spinal dysraphism. Neurosurg Clin NAm 1995; 6: 269-277.
Satar N, Bauer SB, Shefner J, Kelly MD, Darbey MM: The effects of delayed diagnosis and treatment inpatients with an occult spinal dysraphism. J Urol 1995, 154: 754-758.
Pontari MA, Keating M, Kelly M, Dyro F, Bauer SB: Retained sacral function in children with high levelmyelodysplasia. J Urol 1995; 154: 775-777.
Kaefer M, Pabby A, Kelly M, Darbey M, Bauer SB. Improved bladder function after prophylactic treatment ofthe high risk neurogenic bladder in newborns with myelomeningocele. J Urol 1999; 162: 1068-1071.
Wyndaele JJ: Development and evaluation of the management of the neuropathic bladder. Paraplegia1995, 33: 305-307.
Cardenas DD, Mayo ME, Turner LR: Lower urinary changes over time in suprasacral spinal cord injury. Paraplegia 1995; 33: 326-329.
Amarenco G: Troubles vesico-sphincteriens d’origine nerveuse. Rev Prat 1995, 45: 331-335.
Watanabe T, Vaccaro AR, Kumon H, Welch WC, Rivas DA, Chancellor MB. High incidence of occultneurogenic bladder dysfunction in neurologically intact patients with thoracolumbar spinal injuries. J Urol 1998; 159: 965-968.
Ahlberg J, Edlund C, Wikkelsö C, Rosengren L, Fall M. Neurological signs are common in patients withurodynamically verified “idiopathic” bladder overactivity. Neurourol Urodyn 2002; 21: 65-70. 3. DIAGNOSIS Introduction
Before any functional investigation is planned, an extensive general and specific diagnosis should beperformed. Part of this diagnosis is specific for neurogenic pathology and its possible sequelae. The clinicalassessment of patients with NLUTD includes and extends that for other LUTD. The latter should consist of adetailed history, bladder diary and a physical examination. In urinary incontinence, leakage should bedemonstrated objectively. These data are indispensable for reliable interpretation of the findings in diagnostic investigations performedsubsequently in NLUTD.
The general history should include relevant questions to neurological and congenital abnormalities, informationon the previous occurrence and frequency of urinary infections and on relevant surgery. Information must beobtained on medication with known or possible effects on the lower urinary tract (1-3). The general historyshould also include the assessment of menstrual, sexual and bowel function, and obstetric history (3).
Hereditary or familial risk factors should be recorded. Symptoms of any metabolic disorder or
neurological disease that may induce neurogenic lower urinary tract dysfunction must be checked particularly. Specific signs such as pain, infection, hematuria, fever, etc., may justify further particular diagnosis.
A list of items of particular importance is:
Congenital anomalies with possible neurological impact
Metabolic disorders with possible neurological impact
Preceding therapy, including surgical interventions
Lifestyle factors such as smoking, alcohol, or addictive drug use
Urinary history: This consists of symptoms related to both the storage and the evacuation functions of thelower urinary tract. The onset and the nature of the NLUTD (acute or insidious) should be determined. Specificsymptoms and signs must be assessed in NLUTD and if appropriate be compared with the patients’ conditionbefore the neurogenic lower urinary tract dysfunction developed. The separate diagnostic fields items shouldbe diagnosed as detailed as possible (3). •
Mode and type of voiding (catheterization!)
The urinary diary gives (semi-)objective information about the number of voidings, daytime and nighttimevoiding frequency, volumes voided, and incontinence and urge episodes.
Bowel history: Patients with NLUTD may suffer from a related neurogenic condition of the lower gastro-intestinal tract. The bowel history also must address symptoms related to the storage and the evacuationfunctions and specific symptoms and signs must be compared with the patients’ condition before theneurogenic dysfunction developed. Again, the diagnostic items should be detailed (3). •
Sexual history: The sexual function may also be impaired because of the neurogenic condition. The details ofthis history of course differ between men and women (3). •
Sensation in genital area and for sexual functions
Neurologic history: This should concentrate on the following information. 1.
Acquired or congenital neurologic condition
Neurological symptoms (somatic and sensory), with onset, evolution, and performed therapy
Spasticity or autonomic dysreflexia (lesion level above Th6)
3.2.3 GUIDELINES FOR HISTORY TAKING 1.
An extensive general history is mandatory, concentrating on past and present symptoms and conditions for urinary, bowel, sexual, and neurologic functions, and on general conditions that might impair any of these.
Special attention should be paid to the possible existence of alarm signs, such as pain, infection, hematuria, fever, etc., that warrant further specific diagnosis.
Specific history should be taken for each of the four mentioned functions. Physical examination
Attention should be paid to the patient’s physical and possible mental handicaps with respect to planneddiagnostic investigations. Impaired mobility, particularly in the hips, or extreme spasticity may lead to problemsin patient positioning in the urodynamics laboratory. Patients with very high neurological lesions may sufferfrom a significant drop in blood pressure when moved in a sitting or standing position. Subjective indications ofbladder filling sensations may be impossible in retarded patients.
Prostate palpation or observation of pelvic organ descensus is made.
General neurological examination: This investigates the motor and sensory functions of the body, the limbs andthe hand function. A suprapubic globe is searched for and an appreciation of the skin condition in the genitaland perineal regions is made. Figure 3.1. Dermatomes of spinal cord levels L2-S4.Figure 3.2. Urogenital and other reflexes in lower spinal cord
Specific neuro-urologic examination: This investigation is necessary in patients with NLUTD. It includes severaltests for sacral reflex activity and an evaluation of the sensation in the perineal area. Fig. 3.1 shows the differentdermatomes and fig. 3.2 the associated reflexes in this area. Specified information should become available on:•
Sensation S2-S5 on both sides of the body
Volitional contraction of anal sphincter and pelvic floor
A high correlation exists between the clinical neurologic findings and the NLUTD in some types of neuropathy,but less so in other types (4-9). The correspondence is low, for instance, in myelomeningocele patients (6) andin combined traumatic spinal cord lesions, but high in single-level traumatic spinal cord lesions (9).
Besides urinalysis and blood chemistry other tests are specifically indicated in patients with NLUTD. Theresults of these tests should be detailed (3). •
Free flowmetry with assessment of residual urine. Because of natural variations, multiple estimations (atleast 2-3) are necessary (3,10,11).
Quantification of urine loss by pad testing if appropriate
3.3.4 GUIDELINES FOR PHYSICAL EXAMINATION 1.
Individual patient handicaps should be acknowledged in planning further investigations.
The neurological status should be described as completely as possible. Sensations and reflexes in the urogenital area must all be tested.
The anal sphincter and pelvic floor functions must be tested extensively.
Urinalysis, blood chemistry, imaging, free flowmetry and residual, and incontinence quantification should be performed. Urodynamics
Urodynamic investigation is the only method to objectify the (dys-)function of the LUT. This investigation is ofpivotal interest to describe the status of the LUT in patients with NLUTD.
In these patients, particularly when detrusor overactivity might be present, the invasive urodynamic
investigation is even more provocative than in other patients. Any technical source of artefacts must becritically considered. The quality of the urodynamic recording and its interpretation must be ensured (12).
In patients at risk for autonomic dysreflexia, blood pressure assessment during the urodynamic study is
In many patients with NLUTD, assessment of maximum anaesthetic bladder capacity may be useful. The rectal ampulla should be empty of stool before the start of the investigation. Medication by drugs
that influence the lower urinary tract function should be abandoned at least 48 hours before the investigation (iffeasible) or otherwise be taken into account for the interpretation of the data. All urodynamic findings must be reported in detail and performed according to the ICS technicalrecommendations and standards (3,12,13).
Bladder diary: This semi-objective qualification of the LUT is a highly advisable diagnostic tool. For reliableinterpretation it should be recorded over at least 2-3 days (3,14). Possible pathologic findings: High voidingfrequency, very low or very high voided volumes, nocturnal voidings, urgency, incontinence.
Free uroflowmetry and assessment of residual urine: This gives a first impression of the voiding function. It ismandatory before any invasive urodynamics is planned. For reliable information it should be repeated at least2-3 times (3,10,11). Possible pathologic findings: Low flow rate, low voided volume, intermittent flow, hesitancy,residual urine.
Care must be taken in judging the results in patients who are not able to void in a normal position. Both
the flow pattern and the flow rate may be modified by this inappropriate position and by any constructions todivert the flow.
Filling cystometry: The only method to quantify the filling function has limited significance as a solitaryprocedure. It is much more powerful if combined with bladder pressure measurement during micturition andeven more in video urodynamics. This investigation is necessary to document the status of the LUT functionduring the filling phase. The bladder should be empty at the start of filling. A physiological filling rate should beused with body-warm saline, as fast filling and room-temperature saline are provocative (3). Possiblepathologic findings: Detrusor overactivity, low detrusor compliance, abnormal bladder and other sensations,incontinence, incompetent or relaxing urethra.
Detrusor leak point pressure: This specific investigation is important to estimate the risk for the upper urinarytract or for secondary bladder damage. When the DLPP is >40 cm H2O the upper tract is endangered (3,15). The DLPP is a screening test only, because it gives no impression of the duration of the high pressure duringthe filling phase, which can be expected to have even more impact on the upper urinary tract (16). A high DLPPthus warrants further testing by video urodynamics to document the reflux also.
Pressure flow study: This measurement reflects the co-ordination between detrusor and urethra or pelvic floorduring the voiding phase. It is even more powerful in combination with filling cystometry and with videourodynamics. It is necessary to document the function of the lower urinary tract function during the voidingphase. Possible pathologic findings: Detrusor underactivity/acontractility, DSD, non-relaxing urethra, residualurine.
Most types of obstructions caused by NLUTD are due to DSD (17,18), non-relaxing urethra, or non-
relaxing bladder neck (3,19,20). Pressure-flow analysis mostly assesses the amount of mechanical obstructioncaused by the urethra’s inherent mechanical and anatomical properties and has limited value in patients withneurogenic lower urinary tract dysfunction.
Electromyography: Registration of the activity of the external urethral sphincter, the peri-urethral striatedmusculature, the anal sphincter, or the striated pelvic floor muscles. The correct interpretation may be difficultdue to artefacts introduced by other equipment used. In the urodynamic setting useful as a gross indication ofthe patient’s ability to control the pelvic floor. Possible pathologic findings: Inadequate recruitment on specificstimuli (bladder filling, hyperreflexive contractions, onset of voiding, coughing, Valsalva, etc.).
More detailed analysis (motor unit potentials, single fibre EMG) only possible as part of a
Urethral pressure measurement: This investigation has only a very limited place in NLUTD. There exists nobasic consensus on parameters indicating pathological findings (21).
Video urodynamics: This combination of filling cystometry and pressure flow study with imaging is the goldstandard for urodynamic investigation in NLUTD (3,22,23). Possible pathological findings: All as describedunder cystometry and pressure flow study, plus morphological pathology of the LUT and the upper urinarytract.
Ambulatory urodynamics: Functional investigation of the urinary tract utilizing predominantly natural filling ofthe urinary tract and reproducing normal subject activity (24).
This type of study should be considered when office urodynamics do not reproduce the patient’s
symptoms and complaints. Possible pathologic findings: as under filling cystometry and pressure flow studyprovided the flow is measured also. It should be kept in mind that during this study the actual bladder volumeis unknown.
Provocative tests during urodynamics: The LUT function can be provoked by coughing, triggered voiding, oranal stretch.
Fast filling cystometry with cooled saline (the “ice water test”) is considered a discriminative test
between UMNL and LMNL (25-30). Patients with UMNL will develop a detrusor contraction if the detrusormuscle is intact, patients with lower lesions will not. It gives false positive results in young children (27) andseems not fully discriminative in other patients (28,29)
A positive bethanechol test (31) (detrusor contraction >25 cm H2O) was presumed to proof detrusor
denervation hypersensitivity and the muscular integrity of an acontractile detrusor, but it turned out to giveequivocal results. Recently a variation of this method was reported with intravesical electromotiveadministration of the bethanechol (32). This test turned out to be both selective and predictive for successfuloral bethanechol treatment. Specific uro-neurophysiologic tests
These tests are advised as part of the neurological work-up of the patient. They comprise:•
Electromyography (in a neurophysiological setting) of pelvic floor muscles, urethral sphincter and/oranal sphincter
Nerve conduction studies of pudendal nerve
Reflex latency measurements of bulbocavernosus and anal reflex arcs
Evoked responses from clitoris or glans penis
Sensory testing on bladder and urethraOther elective tests may be asked for specific conditions that became obvious during patient work-up
Possible pathologic findings are dependent on the type of the test. 3.4.4 GUIDELINES FOR URODYNAMICS AND URO-NEUROPHYSIOLOGY 1.
Urodynamic investigation is necessary to document the (dys-)function of the LUT.
The recording of a bladder diary is highly advisable.
Free uroflowmetry and assessment of residual urine is mandatory before invasive urodynamics is planned.
Video urodynamics is the gold standard for invasive urodynamics in patients with NLUTD. Should this not be available, then a filling cystometry continuing into a pressure flow study should be performed.
A physiological filling rate and body-warm saline must be used.
DLPP is an important investigation in patients with endangered upper tracts.
Specific uro-neurophysiological tests are elective procedures. Typical manifestations of NLUTD
Typical findings in NLUTD are listed below. Filling phase•
Detrusor overactivity, spontaneous or provoked
Non-relaxing bladder neckThese signs warrant further neurological evaluation, as LUTD may be the presenting symptom of
REFERENCES
Bors E, Turner RD. History and physical examination in neurological urology. J Urol 1960; 83: 759-767.
Thuroff JW, Chartier-Kastler E, Corcus J, Humke J, Jonas U, Palmtag H, Tanagho EA. Medical treatmentand medical side effects in urinary incontinence in the elderly. World J Urol 1998; 16 (Suppl 1): S48-S61.
Stöhrer M, Goepel M, Kondo A, Kramer G, Madersbacher H, Millard R, Rossier A, Wyndaele JJ. Thestandardization of terminology in neurogenic lower urinary tract dysfunction with suggestions fordiagnostic procedures, Neurourol Urodyn 1999; 18:139-158.
Wyndaele JJ, De Sy WA. Correlation between the findings of a clinical neurological examination and theurodynamic dysfunction in children with myelodysplasia. J Urol 1985; 133: 638-640.
Wyndaele JJ. Correlation between clinical neurological data and urodynamic function in spinal cordinjured patients. Spinal Cord 1997; 35: 213-216.
Keshtgar AS, Rickwood AM. Urological consequences of incomplete cord lesions in patients withmyelomeningocele. Br J Urol 1998; 82: 258-260.
Wyndaele JJ. Is impaired perception of bladder filling during cystometry a sign of neuropathy? Br J Urol 1993; 71: 270-273.
Kirchhof K, Fowler CJ. The value of the Kurtzke Functional Systems Scales in predicting incompletebladder emptying. Spinal Cord 2000; 38: 409-413.
Weld KJ, Dmochowski RR. Association of level of injury and bladder behavior in patients with post-traumatic spinal cord injury. Urology 2000; 55: 490-494.
Reynard JM, Peters TJ, Lim C, Abrams P. The value of multiple free-flow studies in men with lowerurinary tract symptoms. Br J Urol 1996; 77: 813-818.
Sonke GS, Kiemeney LA, Verbeek AL, Kortmann BB, Debruyne FM, de la Rosette JJ. Lowreproducibility of maximum urinary flow rate determined by portable flowmetry. Neurourol Urodyn 1999; 18: 183-191.
Schäfer W, Abrams P, Liao L, Mattiasson A, Pesce F, Spångberg A, Sterling AM, Zinner NR, vanKerrebroeck P. Good Urodynamic Practices: Uroflowmetry, Filling Cystometry, and Pressure-FlowStudies. Neurourol Urodyn 2002; 21: 261-274.
Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, van Kerrebroeck P, Victor A, Wein A. Thestandardisation of terminology of lower urinary tract function: Report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn 2002; 21: 167-178.
Homma Y, Ando T, Yoshida M, Kageyama S, Takei M, Kimoto K, Ishizuka O, Gotoh M, Hashimoto T. Voiding and incontinence frequencies: variability of diary data and required diary length. NeurourolUrodyn 2002; 21: 204-209.
McGuire EJ, Cespedes RD, O’Connell HE. Leak-point pressures. Urol Clin North Am 1996; 23: 253-262.
Linsenmeyer TA, Bagaria SP, Gendron B. The impact of urodynamic parameters on the upper tracts ofspinal cord injured men who void reflexly. J Spinal Cord Med 1998; 21: 15-20.
Krongrad A, Sotolongo JR Jr. Bladder neck dysynergia in spinal cord injury. Am J Phys Med Rehabil1996; 75: 204-207.
Weld KJ, Graney MJ, Dmochowski RR. Clinical significance of detrusor sphincter dyssynergia type inpatients with post-traumatic spinal cord injury. Urology 2000; 56: 565-568.
Rossier AB, Fam BA. 5-microtransducer catheter in evaluation of neurogenic bladder function. Urology 1986; 27: 371-378.
Al-Ali M, Haddad L. A 10 year review of the endoscopic treatment of 125 spinal cord injured patientswith vesical outlet obstruction: does bladder neck dyssynergia exist? Paraplegia 1996; 34: 34-38.
Lose G, Griffiths D, Hosker G, Kulseng-Hanssen S, Perucchini D, Schafer W, Thind P, Versi E. Standardisation of urethral pressure measurement: Report from the Standardisation Sub-Committee ofthe International Continence Society. Neurourol Urodyn 2002; 21: 258-260.
Rivas DA, Chancellor MB: Neurogenic vesical dysfunction. Urol Clin North Am 1995, 22: 579-591.
Madersbacher HG. Neurogenic bladder dysfunction. Curr Opin Urol 1999; 9: 303-307.
van Waalwijk van Doorn E, Anders K, Khullar V, Kulseng-Hanssen S, Pesce F, Robertson A, Rosario D,Schafer W. Standardisation of ambulatory urodynamic monitoring: Report of the Standardisation Sub-Committee of the International Continence Society for Ambulatory Urodynamic Studies. NeurourolUrodyn 2000; 19: 113-125.
Geirsson G, Fall M, Lindstrom S. The ice-water test - a simple and valuable supplement to routinecystometry. Br J Urol 1993; 71: 681-685.
Geirsson G, Lindstrom S, Fall M. Pressure, volume and infusion speed criteria for the ice-water test. Br J Urol 1994; 73: 498-503.
Geirsson G, Lindstrom S, Fall M, Gladh G, Hermansson G, Hjalmas K. Positive bladder cooling test inneurologically normal young children. J Urol 1994; 151: 446-448.
Petersen T, Chandiramani V, Fowler CJ. The ice-water test in detrusor hyper-reflexia and bladderinstability. Br J Urol 1997; 79: 163-167.
Chancellor MB, Lavelle J, Ozawa H, Jung SY, Watanabe T, Kumon H. Ice-water test in the urodynamic
evaluation of spinal cord injured patients. Tech Urol 1998; 4: 87-91.
Ronzoni G, Menchinelli P, Manca A, De Giovanni L. The ice-water test in the diagnosis and treatment ofthe neurogenic bladder. Br J Urol 1997; 79: 698-701.
Lapides J. Neurogenic bladder. Principles of treatment. Urol Clin North Am 1974; 1: 81-97.
Riedl CR, Stephen RL, Daha LK, Knoll M, Plas E, Pfluger H. Electromotive administration of intravesicalbethanechol and the clinical impact on acontractile detrusor management: introduction of a new test. J Urol 2000; 164: 2108-2111.
Bemelmans BL, Hommes OR, Van Kerrebroeck PE, Lemmens WA, Doesburg WH, Debruyne FM. Evidence for early lower urinary tract dysfunction in clinically silent multiple sclerosis. J Urol 1991; 145: 1219-1224.
Lewis MA, Shaw J, Sattar TM, Bannister CM. The spectrum of spinal cord dysraphism and bladderneuropathy in children. Eur J Pediatr Surg 1997; 7 (Suppl 1): 35-37.
Wraige E, Borzyskowski M. Investigation of daytime wetting: when is spinal cord imaging indicated?Arch Dis Child 2002; 87: 151-155.
Silveri M, Capitanucci ML, Capozza N, Mosiello G, Silvano A, Gennaro MD. Occult spinal dysraphism:neurogenic voiding dysfunction and long-term urologic follow-up. Pediatr Surg Int 1997; 12: 148-150.
Ahlberg J, Edlund C, Wikkelsö C, Rosengren L, Fall M. Neurological signs are common in patients withurodynamically verified “idiopathic” bladder overactivity. Neurourol Urodyn 2002; 21: 65-70. 4. TREATMENT Introduction
The primary aims for treatment of NLUTD and their priorities are (1-5):1.
Improvement of the patient’s quality of life
Restoration of (parts of) the normal LUT functionFurther considerations are the patient’s disability, the cost effectiveness, the technical intricacy, and the
Preservation of the upper tract function is of paramount importance (1-9). Renal failure was the main
factor for mortality in the spinal cord injured patient surviving the trauma (6-9). This has lead to the golden rulein treatment of NLUTD: Assure that the detrusor pressure remains within safe limits during both the filling phaseand the voiding phase (1-5). This approach has indeed significantly reduced the mortality from urologicalcauses in this patient group (10).
The therapy of urinary incontinence is important for the social rehabilitation of the patient and thus
contributes substantially to the quality of life, but is also pivotal in the prevention of urinary tract infection (UTI)(7-9). When no complete continence can be achieved, methods to attain a socially acceptable control ofincontinence can be applied.
Complex procedures that might enable a satisfactory restoration or replacement of the LUT function
often may limit the patient so much that the quality of life is unacceptably impaired (1).
In patients with high detrusor pressure during the filling phase (detrusor overactivity, low detrusor
compliance) or during the voiding phase (DSD, other causes of bladder outlet obstruction) the therapy is aimedprimarily at “the conversion of an active, aggressive high-pressure bladder into a passive low-pressurereservoir” despite the resulting residual urine (1). Non-invasive conservative treatment
Incomplete bladder emptying is a serious risk factor for UTI, for developing high intravesical pressure duringthe filling phase, and for incontinence. Therefore, methods to improve the voiding process are practised inpatients with NLUTD.
Third party bladder expression (Credé): Regretfully, this method is still applied, foremost in infants and youngchildren with myelomeningocele, and sometimes in tetraplegics. The suprapubic downwards compression ofthe lower abdomen leads to an increase in the intravesical pressure, but also causes a compression of theurethra and thus a functional obstruction (11,12), that may reinforce an already existing high bladder outletresistance (13) and lead to inefficient emptying (12). Because of the high pressures that may be created duringthis procedure it is potentially hazardous for the urinary tract (14,15) and thus it is contra-indicated and its use
should be discouraged unless urodynamics shows intravesical pressure to stay within the safe range (1,14-16).
Voiding by abdominal straining (Valsalva): The considerations mentioned under Credé above also hold for theValsalva manoeuvre (1,12,14,16). As most patients are unable to scale the pressure they exert on the bladderduring Valsalva, the risk of exceeding the safe range is present.
For both methods of emptying long-term complications are hardly avoidable (12,14) and the already
weak pelvic floor function may be further impaired, thus exacerbating the existing incontinence (16).
Triggered reflex voiding: Stimulation of the sacral or lumbar dermatomes in patients with UMNL can elicit reflexcontraction of the detrusor (1,16). Morbidity occurs more often during the first decades of treatment (17-21). This method may be used in patients in whom it is urodynamically safe (1, 16). Lower urinary tract rehabilitation
Behavioural modification: Prompted voiding, timed voiding (bladder training), and modification of the lifepattern in patients with NLUTD are methods to improve the incontinence situation (2,22-25).
Pelvic floor muscle exercises: This training also aims at improving the incontinence. It has proven effective instress incontinence treatment and for patients with NLUTD it is mainly used in multiple sclerosis (26).
Pelvic floor electrostimulation: To improve the effect of pelvic floor muscle exercises, or to learn the patient howto contract the pelvic floor, or to improve the patient compliance with the exercises, this may be supported byelectrostimulation (16,27-29).
Biofeedback: This method can be used for supporting the voiding pattern modification (30-33).
A medical therapy for NLUTD is not available. Most drugs used only resolve part of the problems, or areadjunct to other measures (34-40).
Detrusor overactivity: This can be treated effectively by anticholinergic substances (23,24,34-54). Theirpotentiality extends from a small reduction of detrusor overactivity to complete relaxation, depending ontherapeutic regimen and individual tolerance. Increased drug tolerance during the basically life-long necessarytherapy and the occurrence of adverse effects are topics of concern in patients with NLUTD in particular. Generally, these patients need a higher dose then other patients with overactive detrusor (41-46) and this maylead to an early discontinuation of the therapy because of adverse events (24,41,44-46).
Oxybutynin (36-41,46-49), trospium chloride (39,41,45,50,51), and propiverine (39,43,45,52), are
established medical treatments. These drugs have diverse tolerance profiles and thus another anticholinergicmay be prescribed if the patient experiences adverse effects on one. Tolteridine has been studied only inchildren with NLUTD (42). Various other drugs have been tested (16,36,38,47,48,53).
Additional treatment with desmopressin might improve the efficacy of the treatment (54-58).
Detrusor underactivity: No success had been attained with drugs for improving detrusor contractility (16,59-63),but Riedl et al. (64) have successfully applied oral bethanechol treatment in NLUTD patients with detrusoracontractility who responded positive to the electromotive intravesical bethanechol testing.
Decreasing bladder outlet resistance: Alpha-blockers have been used partly successfully for decreasing thebladder outlet resistance (16,65-70).
Increasing bladder outlet resistance: Several drugs show efficacy in the treatment of selected cases of milderstress incontinence, but there are hardly any publications in patients with NLUTD (16,71,72).
A strong contraction of the urethral sphincter and/or pelvic floor, but also anal dilatation, manipulation of thegenital region, and physical activity reflexly inhibit the micturition (16,73). Whereas the first mechanism isaffected by activation of efferent fibres, the latter ones are produced by activation of afferents (16). Electricalstimulation of the pudendal nerve afferents produces a strong inhibition of the micturition reflex and of thedetrusor contraction (74). This stimulation then might support the restoration of the balance between excitatoryand inhibitory inputs at the spinal or supraspinal level (16,75,76) and it might imply that patients withincomplete lesions will benefit (16,76,77), but patients with complete lesions will not (78).
Stimulation of the tibial nerve afferents has not been applied in patients with NLUTD.
When incontinence cannot be resolved by any of the methods described above, the detrusor pressures are inthe safe region, eventually after sphincterotomy or bladder neck incision, and furthergoing non-invasive therapyis not feasible, social continence may be achieved by collecting the urine during the incontinence (1,16). Condom catheters with urine collection devices are a practical method for men. Otherwise incontinence padsmay offer a reliable solution. In both cases the infection risk must be closely observed (16). Because of the riskof developing high intravesical pressure, the penile clamp is absolutely contra-indicated. 4.2.6 GUIDELINES FOR NON-INVASIVE CONSERVATIVE TREATMENT 1.
The first aim of any therapy is the protection of the upper urinary tract.
The mainstay of the treatment for overactive detrusor is anticholinergic drug therapy.
Rehabilitation and neuromodulation may be effective in selected cases.
A condom catheter or pads may reduce the incontinence to a socially acceptable situation.
Any method of assisted bladder emptying should be used with the greatest caution. Minimal invasive treatment
Intermittent self- or third party catheterization (79,80) is the gold standard for the management of NLUTD (1,16). It is effective in patients with detrusor underactivity or acontractility (1) and in patients with detrusor overactivityif the overactivity can be successfully suppressed for instance by anticholinergic treatment (1,16,34-40).
The catheters used are made from a diversity of materials and the discussions on re-useable or
disposable catheters, use of lubricants, aseptic or clean technique are still going on (1,16,81). Sterile IC, asoriginally proposed by Guttmann and Frankel (79) significantly reduces the risk of UTI and/or bacteriuria(1,16,82,83), related to clean IC introduced by Lapides et al. (80), but the cost issue may be a limiting factor(16,83). Aseptic IC is believed to be in a mid position (1,84,85). Insufficient patient education and the inherentgreater risk of UTI in patients with NLUTD are contributing factors (16,85-91).The average frequency ofcatheterizations per day is 4-6 times. Less frequent catheterization results in higher catheterization volumesand a higher risk of UTI (1,85-90). More frequent catheterization increases the risk of cross infections and othercomplications (1,85-90).
Other complications may include lower fertility in men and compromizing the urethra (16,81), although
the direct relation with the IC is discussed controversely. It appears however that the prevalence of thesecomplications increases with the period that the IC has been practised and with the (temporary) use ofindwelling catheterization (89).
The prevalence of complications can be limited by adequate patient education, use of non-traumatizing
techniques, and adequate precautions to prevent cross-infections (16,91).
Indwelling transurethral catheterization and, although to a lesser extent, suprapubic cystostomy are
significant and early risk factors for UTI and other complications (16,21,92-102). Silicone catheters arepreferred because they are less susceptible for encrustation and because of the high incidence of latex allergyin the NLUTD population. 4.3.2 GUIDELINES FOR CATHETERIZATION 1.
Intermittent catheterization is the standard treatment for patients who are unable to empty the bladder.
Patients should be well instructed on the technique and risks of IC.
The frequency of IC is 4-6 times per day.
The bladder volume must remain below 400 ml and the post-IC residual low.
Indwelling transurethral and suprapubic catheterization should be used only exceptionally, under close control and the catheter should be changed frequently. Silicone catheters are preferred and should be changed every 2-4 weeks, (coated) latex catheters need to be changed every 1-2 weeks.
For the reduction of the detrusor overactivity, anticholinergics can be applied also intravesically (103-112). Thismight reduce the adverse effects because it metabolizes differently (110) and a greater amount is sequesteredin the bladder, even more so with electromotive administration (111,112).
The vanilloids capsaicin and resiniferatoxin desensitize the C-fibers and thereby reduce the detrusor
overactivity for a period of a few months until the sensation of these fibers has restored (15,113-121). Thedosage is 1-2 mMol capsaicin in 100 ml 30% alcohol or 10-100 nMol resiniferatoxin in 100 ml 10% alcohol for30 minutes. Resiniferatoxin has an about 1000-fold potency compared to capsaicin, with less pain during theinstillation, and was effective in patients refractory to capsaicin (121).
Botulinum toxin causes a long-lasting but reversible chemical denervation that lasts for about 9 months
(122-126). The toxin injections are mapped over the detrusor in a dosage that depends on the preparationused. Generalized muscular weakness may be a seldom adverse effect (126).
Intravesical electrostimulation (127) enhances the sensation for bladder filling and urge to void and may restorethe volitional control of the detrusor (16,128,129). Daily stimulation sessions of 90 minutes with 10 mA pulses of2 ms duration at a frequency of 20 Hz (129,130) are used for at least one week (130). It appears that patientswith peripheral lesions are the best candidates, that the detrusor muscle must be intact, and that at least someafferent connection between the detrusor and the brain must still be present (16,129,130). Also, the positioningof the stimulating electrodes and the bladder filling apparently are important parameters (131). With theseprecautions, the results in the literature are still not unequivocal: both positive (128,130,132-136) and negative(137,138) results are reported. Bladder neck and urethral procedures
Reduction of the bladder outlet resistance is often necessary to protect the upper urinary tract. This can be achievednot only by surgical interventions (bladder neck or sphincter incision or urethral stent) but also by chemicaldenervation of the sphincter. Stress incontinence may result and can be managed by external devices (4.2.5).
Botulinum toxin sphincter injection: Detrusor sphincter dyssynergia can be treated effectively by injection withbotulinum toxin in a dosage that depends on the preparation used. The dyssynergia is abolished for a fewmonths, necessitating repeat injections. The efficacy of this treatment is high and few adverse effects havebeen recorded (139-145).
Balloon dilatation: Although favourable immediate results were reported (146), no further reports were foundsince 1994.
Sphincterotomy: By staged incision, the bladder outlet resistance can be reduced without completely losing theclosure function of the urethra (1,14,147). The laser technique appears to be advantageous (1,148,149). Sphincterotomy also needs to be repeated at regular intervals in a substantial proportion of patients (150), butis efficient and without severe adverse effects (1,14,146-151). As secondary narrowing of the bladder neck mayoccur, combined bladder neck incision might be considered (1,152,153).
Bladder neck incision: This is indicated only for secondary changes at the bladder neck (fibrosis)(1,14,147,153). When the detrusor is hypertrophied and causes thickening of the bladder neck, this proceduremakes no sense (1).
Stents: The implantation of urethral stents causes the continence to be dependent on the adequate closure ofthe bladder neck only (1,5). Although the results are comparable with sphincterotomy and the stentingprocedure has a shorter surgery time and reduced hospital stay (154), the costs (1) and possible complicationsor re-interventions (154-160) are limiting factors in its use.
Increasing the bladder outlet resistance: This can improve the continence condition. Despite early positiveresults with urethral bulking agents, a relative early loss of continence is reported in patients with NLUTD(5,21,161-166).
Urethral inserts: Urethral plugs or valves for management of (female) stress incontinence have not been appliedin patients with NLUTD. The experience with active pumping urethral prosthesis for treatment of theunderactive or acontractile detrusor was disappointing (167). 4.3.6 GUIDELINES FOR MINIMAL INVASIVE TREATMENT 1.
Guidelines for catheterization are listed separately under 4.3.2.
Botulinum toxin injections in the detrusor are the most promising intravesical drug application for reduction of detrusor overactivity.
Intravesical electrostimulation may be of value in specific patients.
(Laser) sphincterotomy is the standard treatment for DSD or other increased bladder outlet resistance at the sphincteric area. Botulinum sphincter injections will be the first choice in patients ineligible for interventional surgery. Bladder neck incision is effective in a fibrotic bladder neck. Urethral stents still have too many complications.
Urethral bulking agents have disappointing long term effect. Surgical treatment Urethral and bladder neck procedures
Increasing the bladder outlet resistance has the inherent risk of causing high intravesical pressure during thefilling and even more during the voiding phase. These procedures to treat the sphincteric incontinence aresuitable only when the detrusor activity is or can be controlled, when no significant reflux is present. Moreoverthey require a good condition of the urethra and bladder neck and will mostly lead to perform intermittentcatheterization after the procedure (5,168).
Urethral sling: Various materials have been used for this procedure with enduring positive results (5,168-182). The procedure is established in women; for men the artificial sphincter is obviously the first choice (5).
Artificial urinary sphincter: This device stood the test of time in patients with NLUTD (5). It was introduced byLight and Scott (183) for this patient group and the need for revisions (184,185) have decreased significantlywith the new generations of devices (175,186-192).
Functional sphincter augmentation: By transposing the gracilis muscle to the bladder neck (193) or to theproximal urethra (194,195) the possibility exists to create a functional autologous sphincter by electricalstimulation (193,195). This would open the possibility to restore the control over the urethral closure.
Bladder neck and urethra reconstruction: The classical Young-Dees-Leadbetter (196) procedure forreconstruction of the bladder neck in children with bladder exstrophy and the Kropp urethral lengthening (197)improved by Salle (198) are established methods to restore continence provided that intermittentcatheterization is practised and/or bladder augmentation is performed (175,184,197-211). Detrusor myectomy (auto-augmentation)
The idea to enlarge a shrunken bladder by removal of lateral detrusor tissue to free the entrapped ureter in anon-functional fibrotic detrusor was put forward by Couvelaire (212). Since its clinical introduction byCartwright and Snow (213) in children and by Stöhrer (214,215) in adults, this procedure to reduce detrusoroveractivity or to improve low detrusor compliance has gained popularity because of its acceptable long-termresults, its low surgical burden, its low rate of long term adverse effects, its positive effect on the patient’squality of life, and because it does not preclude further interventions (1,5,45,213-244).
The procedure is performed extraperitoneally under general anesthesia and consists of the dissection of
about 20% of the detrusor tissue around the umbilicus, leaving the mucosa intact (1,213-215). A diverticulumwill develop, but this may take 1-2 years in adults (1,213-215). The laparoscopic procedure(219,220,222,228,233), the covering of the mucosa at the detrusor defect (transperitoneal!)(217,229,232,234,238), supporting the bladder (213,216,238), or simple incision of the detrusor muscle(detrusor myotomy) (221,240-244) are proposed variations of the procedure but offer no essential advantages.
Denervation, deafferentation, neurostimulation, neuromodulation
Various procedures that were estimated to destroy the peripheral detrusor innervation have been abandonedbecause of poor long term results and severe complications (5). These procedures include bladder distension,cystolysis, transvaginal denervation (Ingelman-Sundberg procedure) and subtrigonal phenol injections.
Sacral rhizotomy, also known as sacral deafferentation (SDAF), has achieved some success in reducing
detrusor overactivity (21,245-254), but it is used nowadays mostly as an adjuvant to sacral anterior rootstimulation (255-269). Alternatives for the rhizotomy are sought in this treatment combination (270-273).
Sacral anterior root stimulation (SARS) is aimed at producing a detrusor contraction. The technique was
developed by Brindley (274) and is applicable only in complete lesions above the implant location because ofits stimulation amplitude over the pain threshold. The urethral sphincter efferents are also stimulated, but as thestriated muscle relaxes faster than the smooth muscle of the detrusor, a so-called “post-stimulus voiding” willoccur. This approach has been successful in highly selected patients (255-269). By changing the stimulationparameters this method can also induce defecation or erection.
The sacral nerve stimulation or sacral neuromodulation is based on the research by Schmidt and
Tanagho (275). This technique stimulates the afferents and thereby probably restores the correct balancebetween excitatory and inhibitory impulses from and to the pelvic organs at a sacral and supra-sacral level,thus reducing the detrusor overactivity (75,276). It is used either as a temporary procedure using foramenelectrodes with an external stimulator, with the expectation of perseverance of the changes after treatment, oras a chronic procedure with an implanted stimulator. In the latter case a test procedure, the percutaneousnerve evaluation (PNE), with an external stimulator is performed before the implant to judge the patient’sresponse. This procedure also has considerable success in selected patients (230,277-283).
On the basis of the successful application of these systems, future developments towards a device that
may be more integrated in the body are under research (284,285). Bladder covering by striated muscle
When the bladder is covered by a (part of) striated muscle that can be stimulated electrically, or ideally couldbe contracted volitionally, an acontractile bladder could be restored to perform a voiding function. The rectusabdominis (286) and the latissimus dorsi (287) have been used successfully in patients with NLUTD. Bladder augmentation or substitution
Replacing or expanding the bladder by intestine or other passive expandable coverage will reduce the detrusorcompliance and at least reduce the pressure effect of the detrusor overactivity. The inherent complicationsassociated with these procedures include recurrent infection, stone building, perforation or diverticula, possiblemalignant changes, and for intestine metabolic abnormality, mucus production and impaired bowel function(5,288-290). As the NLUTD patient population’s age when the surgery is performed is generally much lowerthan the patients with bladder malignancy who are elected for this surgery, the possible very long termcomplications must be appraised in particular. Thus the procedures should be used with caution in NLUTDpatients, but may become necessary if all less invasive methods of treatment have failed.
Bladder augmentation, by procedures such as the clam cystoplasty, is a valid option to decrease
detrusor pressure and increase bladder capacity whenever more conservative approaches have failed. Anumber of different techniques have been published. The results of the various procedures are very good andcomparable (45,226,230-232,235-237,289-292). Bladder substitution to create a low pressure reservoir may beindicated in patients with severely thick and fibrotic bladder wall. Scaffolds, probably of tissue-engineeredmaterial for bladder augmentation or substitution or alternative techniques are promising future options(236,293-300).
When no other therapy has been successful urinary diversion must be considered for the protection of theupper tract and for the patient’s quality of life (5,301).
Continent diversion: This should be the first choice for diversion. In patients for whom indwellingcatheterization or suprapubic catheterization is the only feasible treatment option the change to a continentstoma may be a better prospect (5). Some patients with limited dexterity prefer a stoma above using theurethra for catheterization (5). The continent stoma is created following various techniques. All of them howeverdo show frequent complications, including leakage or stenosis (5,302). The short term continence rates areover 80% and good protection of the upper urinary tract is achieved (5,18,301-317). For cosmetic reasons, theumbilicus is often used for the stoma site, but this may have a higher risk of stenosis (305,308,314).
Incontinent diversion: If catheterization is impossible, incontinent diversion with a urine collecting device isindicated. Fortunately, nowadays, this indication is seldom because many appropriate alternatives can beoffered (5). Ultimately it could be considered in patients who are wheelchair bound or bed-ridden withintractable and untreatable incontinence, in devastated lower urinary tracts, when the upper urinary tract isseverely compromised, and in patients who refuse other therapy (5). An ileal segment is used for the deviationin most cases (5,318-323). The rather poor long term results and the expected complications warrant apermanent follow-up (5).
Undiversion: Long-standing diversions may be successfully undiverted or an incontinent diversion changed toa continent one with the emergence of new and better techniques for control of the detrusor pressure and theincontinence (5). Also, in young patients the body image may play a role (311). The patient must be carefullycounselled and must comply meticulously with the instructions (5). Successful undiversion than can beperformed (324-326). GUIDELINES FOR SURGICAL TREATMENT
1.1.1. Detrusor myectomy is an acceptable option for the treatment of overactive bladder when
more conservative approaches have failed. It is limited invasive and has minimal morbidity.
1.1.2. Sacral rhizotomy with SARS in complete lesions and sacral neuromodulation in incomplete
lesions are effective treatments in selected patients.
1.1.3. Bladder augmentation is an acceptable option to decrease detrusor pressure whenever less
invasive procedures have failed. For the treatment of a severely thick or fibrotic bladder wall a bladder substitution might be considered.
1.2.1. SARS with rhizotomy and sacral neuromodulation are effective in selected patients. 1.2.2. Restoration of a functional bladder by covering with striated muscle is still experimental.
Overactive (DSD) - refer to guidelines for minimal invasive treatment (4.3.6)
2.2.1. The placement of a urethral sling is an established procedure. 2.2.2. The artificial urinary sphincter is very effective. 2.2.3. Transposition of the gracilis muscle is still experimental. REFERENCES
Stöhrer M, Kramer G, Löchner-Ernst D, Goepel M, Noll F, Rübben H. Diagnosis and treatment ofbladder dysfunction in spinal cord injury patients. Eur Urol Update Series 1994; 3: 170-175.
Chua HC, Tow A, Tan ES. The neurogenic bladder in spinal cord injury-pattern and management. Ann Acad Med Singapore 1996; 25: 553-557.
Burns AS, Rivas DA, Ditunno JF. The management of neurogenic bladder and sexual dysfunction afterspinal cord injury. Spine. 2001; 26 (Suppl): S129-136.
Rickwood AM. Assessment and conservative management of the neuropathic bladder. Semin PediatrSurg. 2002 May;11(2):108-19.
Castro-Diaz D, Barrett D, Grise P, Perkash I, Stöhrer M, Stone A, Vale P. Surgery for the neuropathicpatient. In: Incontinence, 2nd Edition, Abrams P, Khoury S, Wein A (eds.), Health Publication Ltd,Plymouth, 2002: 865-891.
Donnelly J, Hackler RH, Bunts RC. Present urologic status of the World War II paraplegic: 25-yearfollow-up. Comparison with status of the 20-year Korean War paraplegic and 5-year Vietnamparaplegic. J Urol 1972; 108: 558-562.
Hackler RH. A 25-year prospective mortality study in the spinal cord injured patient: comparison withthe long-term living paraplegic. J Urol 1977; 117: 486-488.
Perkash I, Giroux J. Prevention, treatment, and management of urinary tract infections in neuropathicbladders. J Am Paraplegia Soc 1985; 8: 15-17.
Sandock DS, Gothe BG, Bodner RD. Trimethoprim-sulfamethoxazole prophylaxis against urinary tractinfection in the chronic spinal cord injured patient. Paraplegia 1995; 33: 156-160.
Frankel HL, Coll JR, Charlifue SW, Whiteneck GG, Gardner BP, Jamous MA, Krishnan KR, Nuseibeh I,Savic G, Sett P. Long-term survival in spinal cord injury: a fifty year investigation. Spinal Cord 1998; 36: 266-274.
Madersbacher H. The neuropathic urethra: urethrogram and pathophysiologic aspects. Eur Urol 1977;3: 321-332.
Barbalias GA, Klauber GT, Blaivas JG. Critical evaluation of the Crede maneuver: a urodynamic study of207 patients. J Urol 1983; 130: 720-723.
Clarke SJ, Thomas DG. Characteristics of the urethral pressure profile in flaccid male paraplegics. Br J Urol 1981; 53: 157-161.
Stöhrer M. Alterations in the urinary tract after spinal cord injury - diagnosis, prevention and therapy oflate sequelae. World J Urol 1990; 7: 205-211.
Reinberg Y, Fleming T, Gonzalez R. Renal rupture after the Crede maneuver. J Pediatr 1994; 124: 279-281.
Madersbacher H, Wyndaele JJ, Igawa Y, Chancellor M, Chartier-Kastler E, Kovindha A. Conservativemanagement in neuropatic urinary incontinence. In: Incontinence, 2nd Edition, Abrams P, Khoury S,Wein A (eds.), Health Publication Ltd, Plymouth, 2002: 697-754.
Van Kerrebroeck PE, Koldewijn EL, Scherpenhuizen S, Debruyne FM. The morbidity due to lower urinarytract function in spinal cord injury patients. Paraplegia 1993; 31: 320-329.
Sekar P, Wallace DD, Waites KB, DeVivo MJ, Lloyd LK, Stover SL, Dubovsky EV. Comparison of long-term renal function after spinal cord injury using different urinary management methods. Arch Phys Med
Linsenmeyer TA, Bagaria SP, Gendron B. The impact of urodynamic parameters on the upper tracts ofspinal cord injured men who void reflexly. J Spinal Cord Med 1998; 21: 15-20.
McKinley WO, Jackson AB, Cardenas DD, DeVivo MJ. Long-term medical complications after traumaticspinal cord injury: a regional model systems analysis. Arch Phys Med Rehabil 1999 ; 80: 1402-1410.
Weld KJ, Dmochowski RR. Effect of bladder management on urological complications in spinal cordinjured patients. J Urol 2000; 163: 768-772.
Menon EB, Tan ES. Bladder training in patients with spinal cord injury. Urology 1992; 40: 425-429.
Nijman RJ. Classification and treatment of functional incontinence in children. BJU Int 2000; 85 (Suppl3): 37-42.
Aslan AR, Kogan BA. Conservative management in neurogenic bladder dysfunction. Curr Opin Urol2002; 12: 473-477.
Christ KF, Kornhuber HH. Treatment of neurogenic bladder dysfunction in multiple sclerosis byultrasound-controlled bladder training. Arch Psychiatr Nervenkr 1980; 228: 191-195.
De Ridder D, Vermeulen C, Ketelaer P, Van Poppel H, Baert L. Pelvic floor rehabilitation in multiplesclerosis. Acta Neurol Belg 1999; 99: 61-64.
Ishigooka M, Hashimoto T, Hayami S, Suzuki Y, Nakada T, Handa Y. Electrical pelvic floor stimulation: apossible alternative treatment for reflex urinary incontinence in patients with spinal cord injury. SpinalCord 1996; 34: 411-415.
Vahtera T, Haaranen M, Viramo-Koskela AL, Ruutiainen J. Pelvic floor rehabilitation is effective inpatients with multiple sclerosis. Clin Rehabil 1997; 11: 211-219.
Balcom AH, Wiatrak M, Biefeld T, Rauen K, Langenstroer P. Initial experience with home therapeuticelectrical stimulation for continence in the myelomeningocele population. J Urol 1997; 158: 1272-1276.
Nørgaard JP, Djurhuus JC. Treatment of detrusor-sphincter dyssynergia by bio-feedback. Urol Int 1982;37: 236-239.
Klarskov P, Heely E, Nyholdt I, Rottensten K, Nordenbo A. Biofeedback treatment of bladderdysfunction in multiple sclerosis. A randomized trial. Scand J Urol Nephrol (Suppl) 1994; 157: 61-65.
Chin-Peuckert L, Salle JL. A modified biofeedback program for children with detrusor-sphincterdyssynergia: 5-year experience. J Urol 2001; 166: 1470-1475.
Porena M, Costantini E, Rociola W, Mearini E. Biofeedback successfully cures detrusor-sphincterdyssynergia in pediatric patients. J Urol 2000; 163: 1927-1931.
Baskin LS, Kogan BA, Benard F. Treatment of infants with neurogenic bladder dysfunction usinganticholinergic drugs and intermittent catheterisation. Br J Urol 1990; 66: 532-534.
Tanaka H, Kakizaki H, Kobayashi S, Shibata T, Ameda K, Koyanagi T. The relevance of urethralresistance in children with myelodysplasia: its impact on upper urinary tract deterioration and theoutcome of conservative management. J Urol 1999; 161: 929-932.
Stone AR. Neurourologic evaluation and urologic management of spinal dysraphism. Neurosurg Clin NAm 1995; 6: 269-277.
Edelstein RA, Bauer SB, Kelly MD, Darbey MM, Peters CA, Atala A, Mandell J, Colodny AH, Retik AB. The long-term urological response of neonates with myelodysplasia treated proactively with intermittentcatheterization and anticholinergic therapy. J Urol 1995; 154: 1500-1504.
Hernandez RD, Hurwitz RS, Foote JE, Zimmern PE, Leach GE. Nonsurgical management of threatenedupper urinary tracts and incontinence in children with myelomeningocele. J Urol 1994; 152: 1582-1585.
DasGupta R, Fowler CJ. Bladder, bowel and sexual dysfunction in multiple sclerosis: managementstrategies. Drugs 2003; 63: 153-166.
Buyse G, Verpoorten C, Vereecken R, Casaer P. Treatment of neurogenic bladder dysfunction in infantsand children with neurospinal dysraphism with clean intermittent (self)catheterisation and optimizedintravesical oxybutynin hydrochloride therapy. Eur J Pediatr Surg 1995; 5 Suppl 1: 31-34.
Madersbacher H, Stöhrer M, Richter R, Burgdörfer H, Hachen HJ, Mürtz G. Trospium chloride versusoxybutynin: a randomized, double-blind, multicentre trial in the treatment of detrusor hyperreflexia. Br J Urol 1995; 75: 452-456.
Goessl C, Sauter T, Michael T, Berge B, Staehler M, Miller K. Efficacy and tolerability of tolterodine inchildren with detrusor hyperreflexia. Urology 2000; 55: 414-418.
Madersbacher H, Mürtz G. Efficacy, tolerability and safety profile of propiverine in the treatment of theoveractive bladder (non-neurogenic and neurogenic). World J Urol 2001; 19: 324-335.
Schwantes U, Topfmeier P. Importance of pharmacological and physicochemical properties fortolerance of antimuscarinic drugs in the treatment of detrusor instability and detrusor hyperreflexia-chances for improvement of therapy. Int J Clin Pharmacol Ther 1999; 37: 209-218.
Madersbacher HG. Neurogenic bladder dysfunction. Curr Opin Urol 1999; 9: 303-307
Gajewski JB, Awad SA. Oxybutynin versus propantheline in patients with multiple sclerosis and detrusor
hyperreflexia. J Urol 1986; 135: 966-968.
Zeegers AG, Kiesswetter H, Kramer AE, Jonas U. Conservative therapy of frequency, urgency and urgeincontinence: A double-blind clinical trial of flavoxate hydrochloride, oxybutynin chloride, emeproniumbromide and placebo. World J Urol 1987; 5: 57-61.
Thuroff JW, Bunke B, Ebner A, Faber P, de Geeter P, Hannappel J, Heidler H, Madersbacher H, MelchiorH, Schafer W, et al. Randomized, double-blind, multicenter trial on treatment of frequency, urgency andincontinence related to detrusor hyperactivity: oxybutynin versus propantheline versus placebo. J Urol1991; 145: 813-816.
Kasabian NG, Vlachiotis JD, Lais A, Klumpp B, Kelly MD, Siroky MB, Bauer SB. The use of intravesicaloxybutynin chloride in patients with detrusor hypertonicity and detrusor hyperreflexia. J Urol 1994; 151:944-945.
Stöhrer M, Bauer P, Giannetti BM, Richter R, Burgdörfer H, Mürtz G. Effect of trospium chloride onurodynamic parameters in patients with detrusor hyperreflexia due to spinal cord injuries. A multicentreplacebo-controlled double-blind trial. Urol Int 1991; 47: 138-143.
Fröhlich G, Bulitta M, Strosser W. Trospium chloride in patients with detrusor overactivity: meta-analysisof placebo-controlled, randomized, double-blind, multi-center clinical trials on the efficacy and safety of20 mg trospium chloride twice daily. Int J Clin Pharmacol Ther 2002; 40: 295-303.
Stöhrer M, Madersbacher H, Richter R, Wehnert J, Dreikorn K. Efficacy and safety of propiverine in SCI-patients suffering from detrusor hyperreflexia—a double-blind, placebo-controlled clinical trial. SpinalCord 1999; 37: 196-200.
Jonas U, Petri E, Kissel J. Effect of flavoxate on hyperactive detrusor muscle. Eur Urol 1979; 5: 106-109.
Kinn AC, Larsson PO. Desmopressin: a new principle for symptomatic treatment of urgency andincontinence in patients with multiple sclerosis. Scand J Urol Nephrol 1990; 24: 109-112.
Chancellor MB, Rivas DA, Staas WE Jr. DDAVP in the urological management of the difficult neurogenicbladder in spinal cord injury: Preliminary report. J Am Paraplegia Soc 1994; 17: 165-167.
Eckford SD, Swami KS, Jackson SR, Abrams PH: Desmopressin in the treatment of nocturia andenuresis in patients with multiple sclerosis. Br J Urol 1994; 74: 733-735.
Fredrikson S. Nasal spray desmopressin treatment of bladder dysfunction in patients with multiplesclerosis. Acta Neurol Scand 1996; 94: 31-34.
Valiquette G, Herbert J, Maede-D’Alisera P. Desmopressin in the management of nocturia in patientswith multiple sclerosis. A double-blind, crossover trial. Arch Neurol 1996; 53: 1270-1275.
Light JK, Scott FB. Bethanechol chloride and the traumatic cord bladder. J Urol 1982; 128: 85-87.
Wheeler JS Jr, Robinson CJ, Culkin DJ, Nemchausky BA. Naloxone efficacy in bladder rehabilitation ofspinal cord injury patients. J Urol 1987; 137: 1202-1205.
Komersova K, Rogerson JW, Conway EL, Lim TC, Brown DJ, Krum H, Jackman GP, Murdoch R, LouisWJ. The effect of levcromakalim (BRL 38227) on bladder function in patients with high spinal cordlesions. Br J Clin Pharmacol 1995; 39: 207-209.
Wyndaele JJ, van Kerrebroeck P: The effects of 4 weeks treatment with cisapride on cystometricparameters in spinal cord injury patients. A double-blind, placebo controlled study. Paraplegia 1995; 33:625-627.
Costa P, Bressolle F, Sarrazin B, Mosser J, Sabatier R. Dose-related effect of moxisylyte on maximalurethral closing pressure in patients with spinal cord injuries. Clin Pharmacol Ther 1993; 53: 443-449.
Riedl CR, Stephen RL, Daha LK, Knoll M, Plas E, Pfluger H. Electromotive administration of intravesicalbethanechol and the clinical impact on acontractile detrusor management: introduction of a new test. J Urol 2000; 164: 2108-2111.
Swierzewski 3rd SJ, Gormley EA, Belville WD, Sweetser PM, Wan J, McGuire EJ. The effect of terazosinon bladder function in the spinal cord injured patient. J Urol 1994; 151: 951-954.
O’Riordan JI, Doherty C, Javed M, Brophy D, Hutchinson M, Quinlan D. Do alpha-blockers have a rolein lower urinary tract dysfunction in multiple sclerosis? J Urol 1995; 153: 1114-1116.
Perkash I. Efficacy and safety of terazosin to improve voiding in spinal cord injury patients. J SpinalCord Med 1995; 18: 236-239.
Yasuda K, Yamanishi T, Kawabe K, Ohshima H, Morita T. The effect of urapidil on neurogenic bladder: aplacebo controlled double-blind study. J Urol 1996; 156: 1125-1130.
Sullivan J, Abrams P. Alpha-adrenoceptor antagonists in neurogenic lower urinary tract dysfunction. Urology 1999; 53(3 Suppl 3a): 21-27.
Schulte-Baukloh H, Michael T, Miller K, Knispel HH. Alfuzosin in the treatment of high leak-pointpressure in children with neurogenic bladder. BJU Int 2002 ; 90: 716-720.
Al-Ali M, Salman G, Rasheed A, Al-Ani G, Al-Rubaiy S, Alwan A, Al-Shaikli A. Phenoxybenzamine in themanagement of neuropathic bladder following spinal cord injury. Aust N Z J Surg 1999; 69: 660-663.
Amark P, Beck O. Effect of phenylpropanolamine on incontinence in children with neurogenic bladders.
A double-blind crossover study. Acta Paediatr 1992; 81: 345-350.
Fall M, Lindström S. Electrical stimulation. A physiologic approach to the treatment of urinaryincontinence. Urol Clin North Am 1991; 18: 393-407.
Vodusek DB, Light KJ, Libby JM. Detrusor inhibition induced by stimulation of pudendal nerve afferents. Neurourol Urodyn 1986; 5: 381-389.
Bemelmans BL, Mundy AR, Craggs MD. Neuromodulation by implant for treating lower urinary tractsymptoms and dysfunction. Eur Urol 1999; 36: 81-91.
Primus G, Kramer G. Maximal external electrical stimulation for treatment of neurogenic or non-neurogenic urgency and/or urge incontinence. Neurourol Urodyn 1996; 15: 187-194.
Madersbacher H, Kiss G, Mair D. Transcutaneous electrostimulation of the pudendal nerve for treatmentof detrusor overactivity. Neurourol Urodyn 1995; 14: 501-502.
Previnaire JG, Soler JM, Perrigot M. Is there a place for pudendal nerve maximal electrical stimulationfor the treatment of detrusor hyperreflexia in spinal cord injury patients? Spinal Cord 1998; 36: 100-103.
Guttmann L, Frankel H. The value of intermittent catheterisation in the early management of traumaticparaplegia and tetraplegia. Paraplegia 1966; 4: 63-84.
Lapides J, Diokno AC, Silber SJ, Lowe BS. Clean, intermittent self-catheterization in the treatment ofurinary tract disease. J Urol 1972; 107: 458-461.
Wyndaele JJ. Intermittent catheterization: which is the optimal technique? Spinal Cord 2002; 40: 432-437.
Schlager TA, Dilks S, Trudell J, Whittam TS, Hendley JO. Bacteriuria in children with neurogenic bladdertreated with intermittent catheterization: natural history. J Pediatr 1995; 126: 490-496.
Prieto-Fingerhut T, Banovac K, Lynne CM. A study comparing sterile and nonsterile urethralcatheterization in patients with spinal cord injury. Rehabil Nurs 1997; 22: 299-302.
Matsumoto T, Takahashi K, Manabe N, Iwatsubo E, Kawakami Y. Urinary tract infection in neurogenicbladder. Int J Antimicrob Agents 2001; 17: 293-297.
Stöhrer M, Sauerwein D. Der intermittierende Katheterismus bei neurogener Blasenfunktionsstörung. Eine Standortbestimmung aus urologischer Sicht. Urologe B 2001; 41: 362-368.
Waller L, Jonsson O, Norlen L, Sullivan L. Clean intermittent catheterization in spinal cord injurypatients: long-term followup of a hydrophilic low friction technique. J Urol 1995; 153: 345-348.
Perrouin-Verbe B, Labat JJ, Richard I, Mauduyt de la Greve I, Buzelin JM, Mathe JF. Clean intermittentcatheterisation from the acute period in spinal cord injury patients. Long term evaluation of urethral andgenital tolerance. Paraplegia 1995; 33: 619-624.
Bakke A, Digranes A, Hoisæter PA. Physical predictors of infection in patients treated with cleanintermittent catheterization: a prospective 7-year study. Br J Urol 1997; 79: 85-90.
Günther M, Löchner-Ernst D, Kramer G, Stöhrer M. Auswirkungen des intermittierende aseptischenintermittierenden Katheterismus auf die männliche Harnröhre. Urologe B 2001; 41: 359-361.
Wyndaele JJ. Complications of intermittent catheterization: their prevention and treatment. Spinal Cord2002; 40: 536-541.
Sauerwein D. Urinary tract infection in patients with neurogenic bladder dysfunction. Int J AntimicrobAgents 2002; 19: 592-597.
Sullivan LP, Davidson PG, Kloss DA, D’Anna JA Jr. Small-bowel obstruction caused by a long-termindwelling urinary catheter. Surgery 1990; 107: 228-230.
Chao R, Clowers D, Mayo ME. Fate of upper urinary tracts in patients with indwelling catheters afterspinal cord injury. Urology 1993; 42: 259-262.
Chancellor MB, Erhard MJ, Kiilholma PJ, Karasick S, Rivas DA. Functional urethral closure withpubovaginal sling for destroyed female urethra after long-term urethral catheterization. Urology 1994;43: 499-505.
Bennett CJ, Young MN, Adkins RH, Diaz F. Comparison of bladder management complicationoutcomes in female spinal cord injury patients. J Urol 1995; 153: 1458-1460.
Larsen LD, Chamberlin DA, Khonsari F, Ahlering TE. Retrospective analysis of urologic complications inmale patients with spinal cord injury managed with and without indwelling urinary catheters. Urology1997; 50: 418-422.
West DA, Cummings JM, Longo WE, Virgo KS, Johnson FE, Parra RO. Role of chronic catheterization inthe development of bladder cancer in patients with spinal cord injury. Urology 1999; 53: 292-297.
Nomura S, Ishido T, Teranishi J, Makiyama K. Long-term analysis of suprapubic cystostomy drainage inpatients with neurogenic bladder. Urol Int 2000; 65: 185-189.
Mitsui T, Minami K, Furuno T, Morita H, Koyanagi T. Is suprapubic cystostomy an optimal urinarymanagement in high quadriplegics? A comparative study of suprapubic cystostomy and cleanintermittent catheterization. Eur Urol 2000; 38: 434-438.
Weld KJ, Wall BM, Mangold TA, Steere EL, Dmochowski RR. Influences on renal function in chronicspinal cord injured patients. J Urol 2000; 164: 1490-1493.
Zermann D, Wunderlich H, Derry F, Schroder S, Schubert J. Audit of early bladder managementcomplications after spinal cord injury in first-treating hospitals. Eur Urol 2000; 37: 156-160.
Park YI, Linsenmeyer TA. A method to minimize indwelling catheter calcification and bladder stones inindividuals with spinal cord injury. J Spinal Cord Med 2001; 24: 105-108.
Greenfield SP, Fera M. The use of intravesical oxybutynin chloride in children with neurogenic bladder. JUrol 1991; 146: 532-534.
Glickman S, Tsokkos N, Shah PJ. Intravesical atropine and suppression of detrusor hypercontractility inthe neuropathic bladder. A preliminary study. Paraplegia 1995; 33: 36-39.
Kaplinsky R, Greenfield S, Wan J, Fera M. Expanded followup of intravesical oxybutynin chloride use inchildren with neurogenic bladder. J Urol 1996; 156:753-756.
Holland AJ, King PA, Chauvel PJ, O’Neill MK, McKnight DL, Barker AP. Intravesical therapy for thetreatment of neurogenic bladder in children. Aust N Z J Surg 1997; 67: 731-733.
Amark P, Bussman G, Eksborg S. Follow-up of long-time treatment with intravesical oxybutynin forneurogenic bladder in children. Eur Urol 1998; 34: 148-153.
Haferkamp A, Staehler G, Gerner HJ, Dorsam J. Dosage escalation of intravesical oxybutynin in thetreatment of neurogenic bladder patients. Spinal Cord 2000; 38: 250-254.
Pannek J, Sommerfeld HJ, Botel U, Senge T. Combined intravesical and oral oxybutynin chloride inadult patients with spinal cord injury. Urology 2000; 55: 358-362.
Buyse G, Waldeck K, Verpoorten C, Bjork H, Casaer P, Andersson KE. Intravesical oxybutynin forneurogenic bladder dysfunction: less systemic side effects due to reduced first pass metabolism. J Urol1998; 160: 892-896.
Riedl CR, Knoll M, Plas E, Pflüger H. Intravesical electromotive drug administration technique:preliminary results and side effects. J Urol 1998; 159: 1851-1856.
Di Stasi SM, Giannantoni A, Navarra P, Capelli G, Storti L, Porena M, Stephen RL. Intravesicaloxybutynin: mode of action assessed by passive diffusion and electromotive administration withpharmacokinetics of oxybutynin and N-desethyl oxybutynin. J Urol 2001; 166: 2232-2236.
Fowler CJ, Beck RO, Gerrard S, Betts CD, Fowler CG. Related Intravesical capsaicin for treatment ofdetrusor hyperreflexia. J Neurol Neurosurg Psychiatry 1994; 57: 169-173.
Geirsson G, Fall M, Sullivan L: Clinical and urodynamic effects of intravesical capsaicin treatment inpatients with chronic traumatic spinal detrusor hyperreflexia. J Urol 1995; 154: 1825-1829.
Cruz F, Guimaraes M, Silva C, Rio ME, Coimbra A, Reis M. Desensitization of bladder sensory fibers byintravesical capsaicin has long lasting clinical and urodynamic effects in patients with hyperactive orhypersensitive bladder dysfunction. J Urol 1997; 157: 585-589.
Cruz F, Guimaraes M, Silva C, Reis M. Suppression of bladder hyperreflexia by intravesicalresiniferatoxin. Lancet 1997; 350: 640-641.
De Ridder D, Chandiramani V, Dasgupta P, Van Poppel H, Baert L, Fowler CJ. Intravesical capsaicin as atreatment for refractory detrusor hyperreflexia: a dual center study with long-term followup. J Urol 1997;158: 2087-2092.
Wiart L, Joseph PA, Petit H, Dosque JP, de Seze M, Brochet B, Deminiere C, Ferriere JM, Mazaux JM,N’Guyen P, Barat M. The effects of capsaicin on the neurogenic hyperreflexic detrusor. A double blindplacebo controlled study in patients with spinal cord disease. Preliminary results. Spinal Cord 1998; 36:95-99.
Lazzeri M, Spinelli M, Beneforti P, Zanollo A, Turini D. Intravesical resiniferatoxin for the treatment ofdetrusor hyperreflexia refractory to capsaicin in patients with chronic spinal cord diseases. Scand J UrolNephrol 1998; 32: 331-334.
de Seze M, Wiart L, Joseph PA, Dosque JP, Mazaux JM, Barat M. Capsaicin and neurogenic detrusorhyperreflexia: a double-blind placebo-controlled study in 20 patients with spinal cord lesions. NeurourolUrodyn 1998; 17: 513-523.
Chancellor MB, de Groat WC. Related Intravesical capsaicin and resiniferatoxin therapy: Spicing up theways to treat the overactive bladder. J Urol 1999; 162: 3-11.
Stöhrer M, Schurch B, Kramer G, Schmid D, Gaul G, Hauri D. Botulinum-A toxin in the treatment ofdetrusor hyperreflexia in spinal cord injury: A new alternative to medical and surgical procedures?Neurourol Urodyn 1999; 18: 401-402.
Schurch B, Schmid DM, Stohrer M. Treatment of neurogenic incontinence with botulinum toxin A (letter). N Engl J Med 2000; 342: 665.
For general laboratory and research use onlyQuantification of Human Herpes Virus 3 (Varicella-Zoster) genomes. Introduction to Human Herpes Virus 3 (Varicella-Zoster)Herpes zoster, colloquially known as shingles, is the reactivation (from the general area of thespinal cord) of varicella zoster virus (VZV, primary infection of which leads to chickenpox),one of the Herpesviridae group, leadin
MATERIAL SAFETY DATA SHEET IDENTIFICATION PRODUCT NAME: DuraSeal Powder CHEMICAL NAME: Poly Ethyl Methacrylate MANUFACTURER: Reliance Dental Mfg., Co., 5805 W. 117th Place, P.O. Box 38, Worth, IL 60482 TELEPONE: For Product Information: 708-597-6694 For Medical Information: 800-535-5053 SECTION II - HAZARDOUS INGREDIENTS OF MIXTURES HAZARDOUS COMPONENT CAS REG. NO. SE
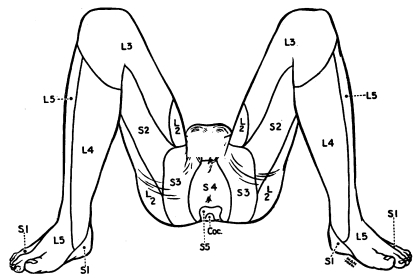 Neurologic history: This should concentrate on the following information.
Neurologic history: This should concentrate on the following information.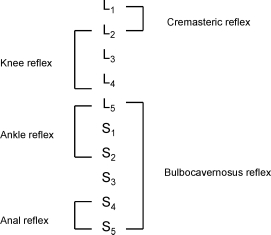 Figure 3.2. Urogenital and other reflexes in lower spinal cord
Specific neuro-urologic examination: This investigation is necessary in patients with NLUTD. It includes severaltests for sacral reflex activity and an evaluation of the sensation in the perineal area. Fig. 3.1 shows the differentdermatomes and fig. 3.2 the associated reflexes in this area.
Figure 3.2. Urogenital and other reflexes in lower spinal cord
Specific neuro-urologic examination: This investigation is necessary in patients with NLUTD. It includes severaltests for sacral reflex activity and an evaluation of the sensation in the perineal area. Fig. 3.1 shows the differentdermatomes and fig. 3.2 the associated reflexes in this area.