Pquadros.com
INTLIFE PAIN MANAGEMENT CIC – FIRST CONSULTATION FORM
REGISTRATION NUMBER: . . . . . . . . . . . . . . . . . . . . . . .
FIRST NAME: . . . . . . . . . . . . . . . . . . . . . . . .
SURNAME: . . . . . . . . . . . . . . . . . . . . . .
(IF APPLICABLE) : . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
AGES: . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
OCCUPATION : . . . . . . . . . . . . . . . . . . . . .
Post Code . . . . . . . . . . . . . . .
DATE OF BIRTH: . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . .
TEL 2: . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . .
AT: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
REFERRED BY: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
FIRST CONSULTANT: . . . . . . . . . . . . . . . . . . DATE OF FIRST CONSULTATION . . . . . . . . . . . . . .
VENUE: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
DISCHARGE DATE . . . . . . . . . . . . . .
DATE . . . . . . . . DISCHARGE GP LETTER SENT
ATTENDANCE
THERAPIST
ACTION TAKEN & DATE
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . .
STORY / SUMMARY
PLEASE ANSWER AS MANY QUESTIONS AS YOU CAN – THEY ARE ALL RELEVANT
Questions asking for an intensity number from 0 – 10, 0 =equals no pain, 10 equals the worse possible pain
1. MAIN SITE OF PAIN (Now): . . . . . . . . . . . . . . . . . . . . . . . . . INTENSITY NOW (From 0 -10) . . . . .
2. IN THE PAST 3 MONTHS, ON AVERAGE, HOW INTENSE WAS YOUR PAIN? (From 0 -10) . . .
3. DID THE PAIN START SOMEWHERE ELSE? YES
3a. If it did, where did it start? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4. WHERE ELSE DO YOU HAVE PAIN? Nowhere else
1) . . . . . . . . . . . . . . . . . . . . . Since . . . . . . . . . . . . . . . Intensity (from 0-10) . . . . . .
2) . . . . . . . . . . . . . . . . . . . . . Since . . . . . . . . . . . . . . . Intensity (from 0-10) . . . . . .
3) . . . . . . . . . . . . . . . . . . . . . Since . . . . . . . . . . . . . . . Intensity (from 0-10) . . . . . .
4) . . . . . . . . . . . . . . . . . . . . . Since . . . . . . . . . . . . . . . Intensity (from 0-10) . . . . . .
5) . . . . . . . . . . . . . . . . . . . . . Since . . . . . . . . . . . . . . . Intensity (from 0-10) . . . . . .
5. HAVE YOU HAD THIS SAME PAIN BEFORE? YES
5a. IF ‘YES’, WHEN DID IT
FIRST APPEARED? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5b. IF ‘NO’, WHEN DID IT START (this time)? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6. IS THE PAIN USUALLY BETTER : AT NIGHT?
7. BRIEFLY, WHAT DO YOU DO THAT MAKES THE CURRENT PAIN BETTER? (even if just a little):
8. WHAT ARE THE MAIN ACTIVITIES THAT YOU COULD DO BEFORE AND THAT YOU CANNOT
DO NOW BECAUSE OF YOUR CURRENT PAIN?
1) . . . . . . . . . . . . . . . . . . . . . . . . . . .
2) . . . . . . . . . . . . . . . . . . . . . . . . . . .
3) . . . . . . . . . . . . . . . . . . . . . . . . . .
4) . . . . . . . . . . . . . . . . . . . . . . . . . .
9. PLEASE LIST ALL PAST AND PRESENT HEALTH ISSUES (physical and mental/emotional)
AND
INJURIES, WHICH HAVE REQUIRED GP INTERVENTION OR HOSPITAL VISIT
CONDITION
CONDITION
1) . . . . . . . . . . . . . . . . . . . . .
6) . . . . . . . . . . . . . . . . . . .
2) . . . . . . . . . . . . . . . . . . . . .
7) . . . . . . . . . . . . . . . . . . .
3) . . . . . . . . . . . . . . . . . . . . .
8) . . . . . . . . . . . . . . . . . . .
4) . . . . . . . . . . . . . . . . . . . . .
9) . . . . . . . . . . . . . . . . . . .
5) . . . . . . . . . . . . . . . . . . . . .
10) . . . . . . . . . . . . . . . . . . .
MAIN CONDITION
10. SINCE THE PAIN/CONDITION STARTED, HAVE YOU OR SOMEONE ELSE NOTICED ANY
CHANGES IN YOUR MOOD? YES
10a. If ‘YES’, how has your mood been affected?
. . . . . . . . . . . . . . . . . . .
11. HAVE YOU CONSULTED YOUR GP ABOUT YOUR CURRENT PAIN/CONDITION?
11a. IF ‘YES’, WHAT WAS THE DIAGNOSIS? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11b. IF ‘YES’, WHAT DID YOUR GP DO ABOUT IT? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11c. IF ‘YES’, DID YOUR GP INTERVENTION HELP?: A LOT
12. HAVE YOU TRIED ANY ALTERNATIVE WAYS TO DEAL WITH YOUR PAIN/CONDITION?
12a. If you have, what have you tried? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
13. ARE YOU TAKING ANY PRESCRIBE D MEDICATION FOR YOUR PAIN/CONDITION?
13a. If ‘YES’, what prescribed medication/s are you taking for your current pain?
1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
3 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
4 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
5 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
13b. Does your prescribed medication help make the pain/condition better?
13c. Does your prescribed medication help make you feel better (in general)?
13d. Do you suffer from side-effects from any of your prescribed medication?
13e. Have you stopped taking any prescribed medication because of its side-effects?
14. ARE YOU TAKING OVER THE COUNTER MEDICATION) FOR YOUR CURRENT
PAIN/CONDITION?
14a. If ‘YES’, what over the counter medication/s are you taking for your current pain?
1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
2 . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
3 . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
14b. Does your over the counter medication help make the pain better?
14c. Does your over the counter medication help make you feel better (in general)?
15. ARE YOU CURRENTLY TAKING MEDICATION FOR ANY OTHER CONDITIONS?
15a. If ‘YES’, please list the other medication below:
1 . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . .
2 . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . .
3 . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . .
4 . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . .
5 . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . .
6 . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . .
7 . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . .
8 . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . .
9 . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . .
10 . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . .
16. HAVE YOU EVER HAD TREATMENT FOR OSTEOPOROSIS OR PAGET’S DISEASE OR HAVE
YOU EVER TAKEN
Actonel and Actonel + Ca , Alendronate sodium tablets (Fosamax and Fosamax + D), Ibandronate sodium tablets (Boniva), Etidronate disodium tablets (Didronel), Tiludronate disodium tablets (Skelid, sanofi-aventis ), Pamidronate disodium injection (Aredia), Zoledronic acid injection (Reclast and Zometa)
17. ARE YOU CURRENTLY TAKING ANY KIND OF SUPPLEMENTS TO MAKE THE CURRENT
PAIN/CONDITION BETTER?
17a. If ‘YES’, what supplements are you taking for your current pain/condition?
1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
2 . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
3 . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
17b. Do your supplements help make the pain/condition better? YES
17c. Do your supplements help make you feel better (in general)? YES
18. ARE YOU CURRENTLY TAKING ANY KIND OF SUPPLEMENTS FOR ANY OTHER REASONS?
(Including vitamins, minerals, herbal remedies, etc) YES
18a. If ‘YES’, what supplements are you currently taking?
1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
2 . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
3 . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
4 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
5 . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
6 . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
7 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
19. HAVE YOU HAD ANY SIGNIFICANT EVENT(S) IN YOU LIFE IMMEDIATELY BEFORE YOUR
CURRENT PAIN/CONDITION STARTED OR EVER?
(These can include bereavement, separation/divorce, loss of employment, difficult childhood, history
of physical or emotional abuse, traumatic experience(s), etc)
1 . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . .
2 . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . .
3 . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . .
4 . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . .
20. ARE YOU ABLE TO WORK? YES
21. IF YOU ARE UNEMPLOYE D, IS IT MAINLY BECAUSE OF YOUR CURRENT PAIN/CONDITION?
22. IF YOU ARE EMPLOYED , HOW MANY DAYS OF WORK HAVE YOU MISSED BECAUSE OF
PAIN DURING THE PAST 12 MONTHS? (Please tick one)
23. DOES YOUR CURRENT PAIN/CONDITION PREVENT YOU FROM HAVING A GOOD SLEEP AT
24. CAN YOU DO NORMAL HOUSE CHORES? YES
25. CAN YOU SOCIALISE? YES
26. DOES YOU CURRENT PAIN/CONDITION NEGATIVELY AFFECT YOUR RELATIONSHIP WITH
YOUR FAMILY OR PARTNER?
27. DOES YOUR CURRENT PAIN/CONDITION MAKE YOU WORRY ABOUT YOUR FUTURE?
28. DO YOU SMOKE? YES
28a. IF ‘YES’ HOW MANY A DAY - ON AVERAGE? . . . . .
29. DO YOU DRINK 4 OR MORE GLASSES OF WATER A DAY? (Coffee/tea/soft drinks do not count)
30. DO YOU DRINK MORE THAN ONE CUP/MUG OF COFFEE A DAY? YES
31. DO YOU DRINK MORE THAN ONE DOSE OF ALCOHOL A DAY? (e.g. up to 1 large glass of wine,
1 dose of spirit, 1 bottle of beer, and so on) YES
32. ARE YOU AWARE OF ANY FOOD ALLERGIES OR INTOLERANCE YOU MAY HAVE?
1 . . . . . . . . . . . . . . . . . . . . . . . . . . .
4 . . . . . . . . . . . . . . . . . . . . . . . . . . .
2 . . . . . . . . . . . . . . . . . . . . . . . . . . .
5 . . . . . . . . . . . . . . . . . . . . . . . . . . .
3 . . . . . . . . . . . . . . . . . . . . . . . . . . .
6 . . . . . . . . . . . . . . . . . . . . . . . . . . .
33. DO YOU REGULARLY EAT POTATOES, TOMATOES AND/OR AUBERGINES (EGGPLANT)?
34. DO YOU REGULARLY CONSUME COW’S MILK, WHEAT, CORN, EGGS, BEEF, YEAST, OR
35. DO YOU REGULARLY EAT A LOT OF MEAT? (SPECIALLY RED)
36. DO YOU REGULARLY EAT FOOD MADE WITH WHITE FLOUR? (e.g. white bread, pasta, biscuits,
37. DO YOU REGULARLY HAVE SUGAR? (This includes ‘hidden’ sugar in ready-made meals, pies,
pastry, cakes, biscuits, marmalades, jam, sweets, soft drinks, etc) YES
38. WHAT DO YOU HOPE TO ACHIEVE BY COMING TO THIS CLINIC? (THIS ARE YOUR ‘GOALS’)
1) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
INTLIFE PAIN MANAGEMENT CIC – PERMISSION SLIP
REG No . . . . . . . . . . . . . . . . .
Please note that YOUR
CONFIDENTIALITY RIGHTS ARE PROTECTED IN EACH CASE
1. I give my permission to have my treatment details shared with my GP and other health care
2. I give my permission to have manual records retained by Intlife Pain Management for
3. I give my permission to have my details stored on Intlife Pain Management’s computer
database and accessed for evaluation purposes:
4. I give my permission to have my written comments on my experience of attending Intlife
Pain Management used for evaluation purposes and/or publicity
5. I give my permission to be contacted for publicity purposes
Please print your name in CAPITAL LETTERS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Signature . . . . . . . . . . . . . . . . . . . . . . . . . . .
Date . . . . . . . . . . . . . . . . . . .
Source: http://pquadros.com/Intlife%20Pain%20-%20First%20consultation%20form%20edited%20July%2008.pdf
Hemophilia OUTLOOK The Hemophilia Association of New York, Inc. ‚ SPRING 2010 ‚ Missing: Nearly 25% of the minimum goal for this year’s HANY GOLF 2010 3rd Annual Matthew Lee Greer Golf Classic – June 21st 17th Annual Nick Salerno Memorial Golf Tournament – July 12th form TODAY . Early bird sponsors include: Inspiration Biopharmaceuticals ,
Die Welt-Anti-Doping-Agentur (WADA) möchte der Deutschen Bundesregierung und der Nationalen Anti-Doping Agentur Deutschland (NADA) für den wertvollen Beitrag bei der Abfassung der deutschen Dokumente danken. Dadurch wird der weltweite Austausch der Dokumente sowie die Zusammenarbeit zwischen der WADA und den öffentlichen Behörden und Sportbewegungen zum Ziel der Beseitigung von Doping im Spor
A |
B |
C |
D |
E |
F |
G |
H |
I |
J |K |
L |
M |
N |
O |
P |
Q |
R |
S |
T |
U |V |
W |
X |
Y |
Z |
0-9 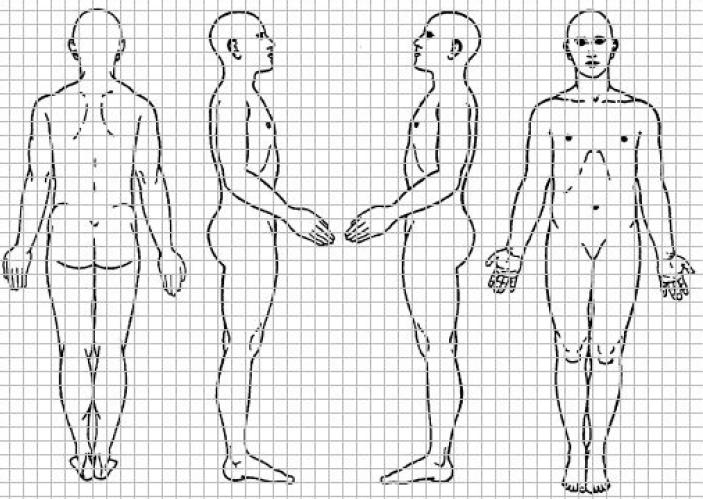
 PLEASE ANSWER AS MANY QUESTIONS AS YOU CAN – THEY ARE ALL RELEVANT
PLEASE ANSWER AS MANY QUESTIONS AS YOU CAN – THEY ARE ALL RELEVANT




 4. WHERE ELSE DO YOU HAVE PAIN? Nowhere else
4. WHERE ELSE DO YOU HAVE PAIN? Nowhere else