Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Microsoft word - proposed.doc
ATTENTION PHARMACIST: Detach “Patient’s Instructions for Use” from package insert and dispense with the product. Combivent®
(ipratropium bromide and albuterol sulfate) Inhalation Aerosol
Bronchodilator For Oral Inhalation Only Rx only Prescribing Information
DESCRIPTION
COMBIVENT Inhalation Aerosol is a combination of ipratropium bromide (as the monohydrate) and albuterol sulfate.
Ipratropium bromide is an anticholinergic bronchodilator chemically described as 8-azoniabicyclo[3.2.1] octane, 3-(3-hydroxy-1-oxo-2-phenylpropoxy)-8-methyl-8-(1-methylethyl)-, bromide monohydrate, (3-endo, 8-syn)-: a synthetic quaternary ammonium compound chemically related to atropine. Ipratropium bromide is a white to off-white crystalline substance, freely soluble in water and methanol, sparingly soluble in ethanol, and insoluble in lipophilic solvents such as ether, chloroform and fluorocarbons.
Albuterol sulfate, chemically known as (1,3-benzenedimethanol, α'-[[(1,1dimethylethyl) amino] methyl]-4-hydroxy, sulfate (2:1)(salt), (±)- is a relatively selective beta2-adrenergic bronchodilator. Albuterol is the official generic name in the United States. The World Health Organization recommended name for the drug is salbutamol. Albuterol sulfate is a
white to off-white crystalline powder, freely soluble in water and slightly soluble in alcohol, chloroform, and ether. The structural formula is:
Combivent® (ipratropium bromide and albuterol sulfate) Inhalation Aerosol contains a microcrystalline suspension of ipratropium bromide and albuterol sulfate in a pressurized metered-dose aerosol unit for oral inhalation administration. The 200 inhalation unit has a net weight of 14.7 grams. Each actuation meters 21 mcg of ipratropium bromide and 120 mcg of albuterol sulfate from the valve and delivers 18 mcg of ipratropium bromide and 103 mcg of albuterol sulfate (equivalent to 90 mcg albuterol base) from the mouthpiece. The excipients are dichlorodifluoromethane, dichlorotetrafluoroethane, and trichloromonofluoromethane as propellants and soya lecithin.
CLINICAL PHARMACOLOGY
COMBIVENT Inhalation Aerosol is a combination of the anticholinergic bronchodilator, ipratropium bromide, and the beta2-adrenergic bronchodilator, albuterol sulfate.
Mechanism of Action
Ipratropium bromide is an anticholinergic (parasympatholytic) agent which, based on animal studies, appears to inhibit vagally-mediated reflexes by antagonizing the action of acetylcholine, the transmitter agent released at the neuromuscular junctions in the lung. Anticholinergics prevent the increases in intracellular concentration of cyclic guanosine monophosphate (cyclic GMP) which are caused by interaction of acetylcholine with the muscarinic receptors on bronchial smooth muscle.
In vitro studies and in vivo pharmacologic studies have demonstrated that albuterol has a preferential effect on beta2-adrenergic receptors compared with isoproterenol. While it is recognized that beta2-adrenergic receptors are the predominant receptors on bronchial smooth muscle, recent data indicate that there is a population of beta2-receptors in the human heart
which comprise between 10% and 50% of cardiac beta-adrenergic receptors. The precise function of these receptors, however, is not yet established (see WARNINGS).
Activation of beta2-adrenergic receptors on airway smooth muscle leads to the activation of adenylyl cyclase and to an increase in the intracellular concentration of cyclic-3',5'-adenosine monophosphate (cyclic AMP). This increase of cyclic AMP leads to the activation of protein kinase A, which inhibits the phosphorylation of myosin and lowers intracellular ionic calcium concentrations, resulting in relaxation. Albuterol relaxes the smooth muscles of all airways, from the trachea to the terminal bronchioles. Albuterol acts as a functional antagonist to relax the airway irrespective of the spasmogen involved, thus protecting against all bronchoconstrictor challenges. Increased cyclic AMP concentrations are also associated with the inhibition of release of mediators from mast cells in the airway.
Albuterol has been shown in most clinical trials to have more bronchial smooth muscle relaxation effect than isoproterenol at comparable doses while producing fewer cardiovascular effects. However, all beta-adrenergic drugs, including albuterol sulfate, can produce a significant cardiovascular effect in some patients (see PRECAUTIONS).
Combivent® (ipratropium bromide and albuterol sulfate) Inhalation Aerosol is expected to maximize the response to treatment in patients with chronic obstructive pulmonary disease (COPD) by reducing bronchospasm through two distinctly different mechanisms, anticholinergic (parasympatholytic) and sympathomimetic. Simultaneous administration of both an anticholinergic (ipratropium bromide) and a beta2-sympathomimetic (albuterol sulfate) is designed to benefit the patient by producing a greater bronchodilator effect than when either drug is utilized alone at its recommended dosage.
Pharmacokinetics
Much of an administered dose is swallowed as shown by fecal excretion studies. Ipratropium bromide is a quaternary amine. It is not readily absorbed into the systemic circulation either from the surface of the lung or from the gastrointestinal tract as confirmed by blood level and renal excretion studies. Plasma levels of ipratropium bromide were below the assay sensitivity limit of 100 pg/mL.
The half-life of elimination is about 2 hours after inhalation or intravenous administration. Ipratropium bromide is minimally bound (0 to 9% in vitro) to plasma albumin and α1-acid glycoprotein. It is partially metabolized to inactive ester hydrolysis products. Following intravenous administration, approximately one-half of the dose is excreted unchanged in the urine. Autoradiographic studies in rats have shown that ipratropium bromide does not penetrate the blood-brain barrier.
Albuterol is longer acting than isoproterenol in most patients because it is not a substrate for the cellular uptake processes for catecholamines nor for metabolism by catechol-O-methyl transferase. Instead, the drug is conjugatively metabolized to albuterol 4'-O-sulfate.
In a pharmacokinetic study in 12 healthy male volunteers of two inhalations of albuterol sulfate, 103 mcg dose/inhalation through the mouthpiece, peak plasma albuterol concentrations ranging from 419 to 802 pg/mL (mean 599 ± 122 pg/mL) were obtained within three hours post-administration. Following this single-dose administration, 30.8 ± 10.2% of the estimated mouthpiece dose was excreted unchanged in the 24-hour urine. Since albuterol sulfate is rapidly and completely absorbed, this study could not distinguish between pulmonary and gastrointestinal absorption.
Intravenous pharmacokinetics of albuterol were studied in a comparable group of 16 healthy male volunteers; the mean terminal half-life following a 30-minute infusion of 1.5 mg was 3.9 hours with a mean clearance of 439 mL/min/1.73 m2.
Intravenous albuterol studies in rats demonstrated that albuterol crossed the blood-brain barrier and reached brain concentrations amounting to about 5% of the plasma concentrations. In structures outside the blood-brain barrier (pineal and pituitary glands), the drug achieved concentrations more than 100 times those in whole brain.
Studies in pregnant rats with tritiated albuterol demonstrated that approximately 10% of the circulating maternal drug was transferred to the fetus. Disposition in fetal lungs was comparable to maternal lungs, but fetal liver disposition was 1% of maternal liver levels.
Studies in laboratory animals (minipigs, rodents, and dogs) have demonstrated the occurrence of cardiac arrhythmias and sudden death (with histologic evidence of myocardial necrosis) when beta-agonists and methylxanthines were administered concurrently. The significance of these findings when applied to humans is unknown.
In a crossover pharmacokinetic study in 12 healthy male volunteers comparing the pattern of absorption and excretion of two inhalations of Combivent® (ipratropium bromide and albuterol sulfate) Inhalation Aerosol to the two active components individually, the co-administration of ipratropium bromide and albuterol sulfate from a single canister did not significantly alter the systemic absorption of either component.
Ipratropium bromide levels remained below detectable limits (<100 pg/mL). Peak albuterol level obtained within 3 hours post-administration was 492 ± 132 pg/mL. Following this single administration, 27.1 ± 5.7% of the estimated mouthpiece dose was excreted unchanged in the 24-hour urine. From a pharmacokinetic perspective, the synergistic efficacy of COMBIVENT Inhalation Aerosol is likely to be due to a local effect on the muscarinic and beta2-adrenergic receptors in the lung.
Special Populations
The pharmacokinetics of Combivent® (ipratropium bromide and albuterol sulfate) Inhalation Aerosol or ipratropium bromide have not been studied in patients with hepatic or renal insufficiency or in the elderly (see PRECAUTIONS). Drug-Drug Interactions
No specific pharmacokinetic studies were conducted to evaluate potential drug-drug interactions.
Pharmacodynamics
The bronchodilation following inhalation of ipratropium bromide is primarily a local, site-specific effect, not a systemic one.
Controlled clinical studies have demonstrated that ipratropium bromide does not alter either mucociliary clearance or the volume or viscosity of respiratory secretions. In studies without a positive control, ipratropium bromide did not alter pupil size, accommodation or visual acuity (see ADVERSE REACTIONS).
Ventilation/perfusion studies have shown no clinically significant effects on pulmonary gas exchange or arterial oxygen tension. At recommended doses, ipratropium bromide does not produce clinically significant changes in pulse rate or blood pressure.
Clinical Trials
In two 12-week randomized, double-blind, active-controlled clinical trials, 1067 patients with chronic obstructive pulmonary disease (COPD) were evaluated for the bronchodilator efficacy of COMBIVENT Inhalation Aerosol (358 patients) in comparison to its components, ipratropium bromide (362 patients) and albuterol sulfate (347 patients).
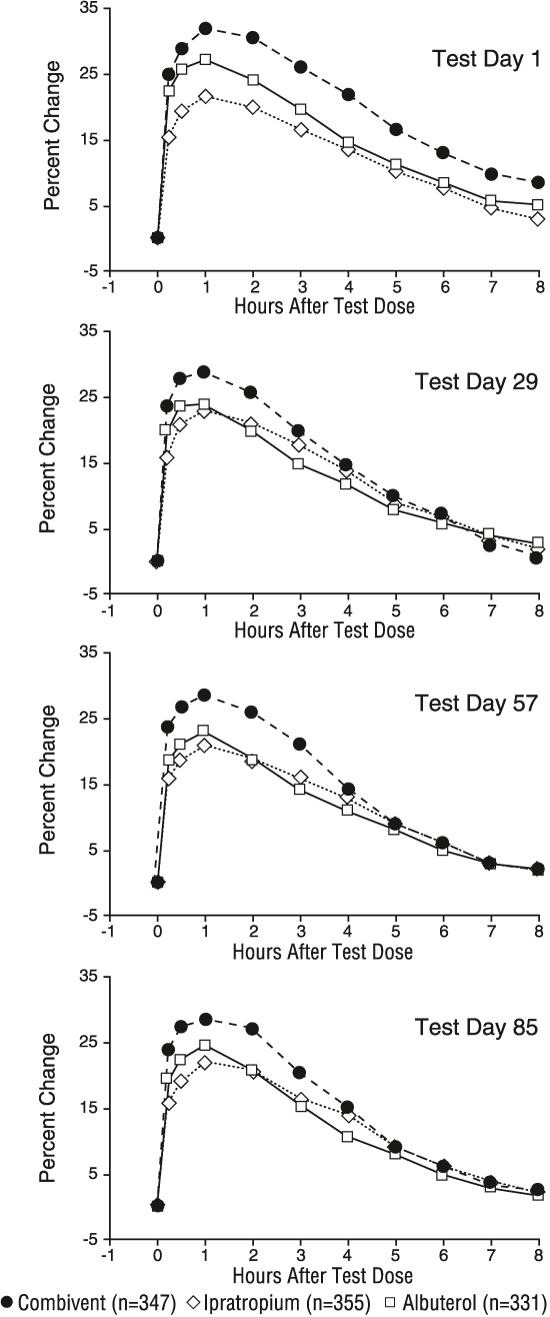
Serial FEV1 measurements (shown below as a percent change from test-day baseline) demonstrated that COMBIVENT Inhalation Aerosol produced significantly greater improvement in pulmonary function than either ipratropium bromide or albuterol sulfate when given separately. The median time to onset of a 15% increase in FEV1 was 15 minutes and the median time to peak FEV1 was one hour for COMBIVENT Inhalation Aerosol and its components. The median duration of effect as measured by FEV1 was 4-5 hours for COMBIVENT Inhalation Aerosol compared to 4 hours for ipratropium bromide and 3 hours for albuterol sulfate.
Percent Change in Adjusted Meana FEV1 from Test-Day Baseline - Endpoint Analysis of the Evaluable Data Set a Adjusted for test-day baseline FEV1, center and treatment-by-center interaction
These studies demonstrated that each component of Combivent® (ipratropium bromide and albuterol sulfate) Inhalation Aerosol contributed to the improvement in pulmonary function produced by the combination, especially during the first 4-5 hours after dosing, and that COMBIVENT Inhalation Aerosol was significantly more effective than ipratropium bromide or albuterol sulfate administered alone.
In the two controlled twelve-week studies, COMBIVENT Inhalation Aerosol did not produce any change in the secondary efficacy parameters including symptom scores, physician global assessments and morning PEFR, all of which were monitored throughout the study period.
INDICATIONS AND USAGE
COMBIVENT Inhalation Aerosol is indicated for use in patients with chronic obstructive pulmonary disease (COPD) on a regular aerosol bronchodilator who continue to have evidence of bronchospasm and who require a second bronchodilator.
CONTRAINDICATIONS
COMBIVENT Inhalation Aerosol is contraindicated in patients with a history of hypersensitivity to soya lecithin or related food products such as soybean and peanut. COMBIVENT Inhalation Aerosol is also contraindicated in patients hypersensitive to any other components of the drug product or to atropine or its derivatives.
WARNINGS 1. Paradoxical Bronchospasm: COMBIVENT Inhalation Aerosol can produce paradoxical bronchospasm that can be life-threatening. If it occurs, the preparation should be discontinued immediately and alternative therapy instituted. It should be recognized that paradoxical bronchospasm, when associated with inhaled formulations, frequently occurs with the first use of a new canister. 2.Cardiovascular Effect: The albuterol sulfate contained in COMBIVENT Inhalation Aerosol, like other beta-adrenergic agonists, can produce a clinically significant cardiovascular effect in some patients, as measured by pulse rate, blood pressure and/or symptoms. Although such effects are uncommon after administration of COMBIVENT Inhalation Aerosol at recommended doses, if they occur, discontinuation of the drug may be indicated. There is some evidence from post-marketing data and published literature of rare occurrences of myocardial ischemia associated with albuterol. In addition, beta-adrenergic agents have been reported to produce ECG changes, such as flattening of the T wave, prolongation of the QTc interval, and ST segment depression. Therefore, COMBIVENT Inhalation Aerosol should be used with caution in patients with cardiovascular disorders, especially coronary insufficiency, cardiac arrhythmias and hypertension. 3. Do Not Exceed Recommended Dose: Fatalities have been reported in association with excessive use of inhaled sympathomimetic drugs, in patients with asthma. The exact cause of death is unknown, but cardiac arrest following an unexpected development of a severe acute asthmatic crisis and subsequent hypoxia is suspected. 4.Immediate Hypersensitivity Reactions: Immediate hypersensitivity reactions may occur after administration of ipratropium bromide or albuterol sulfate, as demonstrated by rare cases of urticaria, angioedema, rash, bronchospasm, anaphylaxis, and oropharyngeal edema. 5.Storage Conditions: The contents of Combivent® (ipratropium bromide and albuterol sulfate) Inhalation Aerosol are under pressure. Do not puncture. Do not use or store near heat or open flame. Exposure to temperatures above 120°F may cause bursting. Never throw the container into a fire or incinerator. Keep out of reach of children. PRECAUTIONS
1. Effects Seen with Anticholinergic Drugs: COMBIVENT Inhalation Aerosol contains ipratropium bromide and, therefore, should be used with caution in patients with narrow-angle glaucoma, prostatic hyperplasia or bladder-neck obstruction.
2. Effects Seen with Sympathomimetic Drugs: Preparations containing sympathomimetic amines such as albuterol sulfate should be used with caution in patients with convulsive disorders, hyperthyroidism, or diabetes mellitus and in patients who are unusually responsive to sympathomimetic amines. Beta-adrenergic agents may also produce significant hypokalemia in some patients (possibly through intracellular shunting) which has the potential to produce adverse cardiovascular effects. The decrease in serum potassium is usually transient, not requiring supplementation.
3. Use in Hepatic or Renal Disease: COMBIVENT Inhalation Aerosol has not been studied in patients with hepatic or renal insufficiency. It should be used with caution in those patient populations.
Information for Patients
Patients should be cautioned to avoid spraying the aerosol into their eyes and be advised that this may result in precipitation or worsening of narrow-angle glaucoma, mydriasis, increased intraocular pressure, acute eye pain or discomfort, temporary blurring of vision, visual halos or colored images in association with red eyes from conjunctival and corneal congestion. Patients should also be advised that should any combination of these symptoms develop, they should consult their physician immediately.
The action of COMBIVENT Inhalation Aerosol should last 4-5 hours or longer. COMBIVENT Inhalation Aerosol should not be used more frequently than recommended. Do not increase the dose or frequency of COMBIVENT Inhalation Aerosol without consulting your physician. If you find that treatment with COMBIVENT Inhalation Aerosol becomes less effective for symptomatic relief, your symptoms become worse, and/or you need to use the product more frequently than usual, medical attention should be sought immediately. While you are taking COMBIVENT Inhalation Aerosol, other inhaled drugs should be taken only as directed by your physician. If you are pregnant or nursing, contact your physician about use of COMBIVENT Inhalation Aerosol. Appropriate use of
Combivent® (ipratropium bromide and albuterol sulfate) Inhalation Aerosol includes an understanding of the way it should be administered (see Patient’s Instructions for Use). Drug Interactions
COMBIVENT Inhalation Aerosol has been used concomitantly with other drugs, including sympathomimetic bronchodilators, methylxanthines, and oral and inhaled steroids, commonly used in the treatment of chronic obstructive pulmonary disease. With the exception of albuterol, there are no formal studies fully evaluating the interaction effects of COMBIVENT Inhalation Aerosol and these drugs with respect to effectiveness.
Anticholinergic agents: Although ipratropium bromide is minimally absorbed into the systemic circulation, there is some potential for an additive interaction with concomitantly used anticholinergic medications. Caution is therefore advised in the co-administration of COMBIVENT Inhalation Aerosol with other anticholinergic-containing drugs.
Beta-adrenergic agents: Caution is advised in the co-administration of COMBIVENT Inhalation Aerosol and other sympathomimetic agents due to the increased risk of adverse cardiovascular effects.
Beta-receptor blocking agents and albuterol inhibit the effect of each other. Beta-receptor blocking agents should be used with caution in patients with hyperreactive airways.
Diuretics: The ECG changes and/or hypokalemia which may result from the administration of non-potassium sparing diuretics (such as loop or thiazide diuretics) can be acutely worsened by beta-agonists, especially when the recommended dose of the beta-agonist is exceeded. Although the clinical significance of these effects is not known, caution is advised in the co-administration of beta-agonist-containing drugs, such as COMBIVENT Inhalation Aerosol, with non-potassium sparing diuretics.
Monoamine oxidase inhibitors or tricyclic antidepressants: COMBIVENT Inhalation Aerosol should be administered with extreme caution to patients being treated with monoamine oxidase inhibitors or tricyclic antidepressants or within two weeks of discontinuation of such agents because the action of albuterol on the cardiovascular system may be potentiated.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Two-year oral carcinogenicity studies in rats and mice have revealed no carcinogenic activity at doses up to 6 mg/kg. This dose corresponds in rats and mice to approximately 230 and 110 times the maximum recommended daily inhalation dose of ipratropium bromide in adults, respectively, on a mg/m2 basis. Results of various mutagenicity studies (Ames test, mouse dominant lethal test, mouse micronucleus test and chromosome aberration of bone marrow in Chinese hamsters) were negative.
Fertility of male or female rats at oral doses up to 50 mg/kg (approximately 1,900 times the maximum recommended daily inhalation dose in adults on a mg/m2 basis) was unaffected by
ipratropium bromide administration. At an oral dose of 500 mg/kg (approximately 19,000 times the maximum recommended daily inhalation dose in adults on a mg/m2 basis), ipratropium bromide produced a decrease in the conception rate.
Like other agents in its class, albuterol caused a significant dose-related increase in the incidence of benign leiomyomas of the mesovarium in a two-year study in the rat at dietary doses of 2, 10 and 50 mg/kg (approximately 15, 65 and 330 times the maximum recommended daily inhalation dose in adults on a mg/m2 basis). In another study this effect was blocked by the co-administration of propranolol. The relevance of these findings to humans is not known. An 18-month study in mice at dietary doses up to 500 mg/kg (approximately 1,600 times the maximum recommended daily inhalation dose in adults on a mg/m2 basis) and a 99-week study in hamsters at oral doses up to 50 mg/kg (approximately 220 times the maximum recommended daily inhalation dose in adults on a mg/m2 basis) revealed no evidence of tumorigenicity. Studies with albuterol revealed no evidence of mutagenesis.
Reproduction studies in rats with albuterol sulfate revealed no evidence of impaired fertility.
Pregnancy Teratogenic Effects: Pregnancy Category C.
There are no adequate and well-controlled studies of Combivent® (ipratropium bromide and albuterol sulfate) Inhalation Aerosol, ipratropium bromide or albuterol sulfate, in pregnant women. Animal reproduction studies have not been conducted with COMBIVENT Inhalation Aerosol. However, albuterol sulfate has been shown to be teratogenic in mice. COMBIVENT Inhalation Aerosol should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Oral reproduction studies were performed at doses of 10 mg/kg in mice, 1,000 mg/kg in rats and 125 mg/kg in rabbits. These doses correspond in each species, respectively, to approximately 190, 38,000, and 9,400 times the maximum recommended daily inhalation dose in adults on a mg/m2 basis. Inhalation reproduction studies were conducted in rats and rabbits at doses of 1.5 and 1.8 mg/kg (approximately 55 and 140 times the maximum recommended daily inhalation dose in adults on a mg/m2 basis). These studies demonstrated no evidence of teratogenic effects as a result of ipratropium bromide. At oral doses 90 mg/kg and above in rats (approximately 3,400 times the maximum recommended daily inhalation dose in adults on a mg/m2 basis) embryotoxicity was observed as increased resorption. This effect is not considered relevant to human use due to the large doses at which it was observed and the difference in route of administration.
Albuterol has been shown to be teratogenic in mice. A reproduction study in CD-1 mice given albuterol subcutaneously (0.025, 0.25 and 2.5 mg/kg) showed cleft palate formation in 5 of 111 (4.5%) fetuses at 0.25 mg/kg (equivalent to the maximum recommended daily inhalation dose in adults on a mg/m2 basis) and in 10 of 108 (9.3%) fetuses at 2.5 mg/kg (approximately 8 times the maximum recommended daily inhalation dose in adults on a mg/m2 basis). None was observed at 0.025 mg/kg (less than the maximum recommended daily inhalation dose in adults). Cleft palate also occurred in 22 of 72 (30.5%) fetuses treated with 2.5 mg/kg isoproterenol (positive control). A reproduction study with oral albuterol in Stride Dutch rabbits revealed cranioschisis in 7 of 19 (37%) fetuses at 50 mg/kg (approximately 660 times the maximum recommended daily inhalation dose in adults on a mg/m2 basis).
Labor and Delivery
Because of the potential for beta-agonist interference with uterine contractility, use of Combivent® (ipratropium bromide and albuterol sulfate) Inhalation Aerosol for the treatment of COPD during labor should be restricted to those patients in whom the benefits clearly outweigh the risk.
Nursing Mothers
It is not known whether the components of COMBIVENT Inhalation Aerosol are excreted in human milk.
Although lipid-insoluble quaternary cations pass into breast milk, it is unlikely that the active component, ipratropium bromide, would reach the infant to an important extent, especially when taken by aerosol. However, because many drugs are excreted in human milk, caution should be exercised when COMBIVENT Inhalation Aerosol is administered to a nursing mother.
Because of the potential for tumorigenicity shown for albuterol in animal studies, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use
Safety and effectiveness in the pediatric population have not been established.
ADVERSE REACTIONS
Adverse reaction information concerning Combivent® (ipratropium bromide and albuterol sulfate) Inhalation Aerosol is derived from two 12-week controlled clinical trials (N=358 for COMBIVENT Inhalation Aerosol) as seen in Table 1.
All Adverse Events (in percentages), from Two Large Double-blind, Parallel, 12-Week Studies of Patients with COPD* COMBIVENT Ipratropium Albuterol Sulfate Ipratropium Bromide 206 mcg QID 36 mcg/Albuterol 36 mcg QID 206 mcg QID Body as a Whole-General Disorders Gastrointestinal System Disorders Respiratory System Disorders (Lower) Respiratory System Disorders (Upper)
*All adverse events, regardless of drug relationship, reported by two percent or more patients in one or more treatment group in the 12-week controlled clinical trials.
Additional adverse reactions, reported in less than two percent of the patients in the COMBIVENT Inhalation Aerosol treatment group include edema, fatigue, hypertension, dizziness, nervousness, paresthesia, tremor, dysphonia, insomnia, diarrhea, dry mouth, dyspepsia, vomiting, arrhythmia, palpitation, tachycardia, arthralgia, angina, increased sputum, taste perversion, and urinary tract infection/dysuria.
Allergic-type reactions such as skin rash, angioedema of tongue, lips and face, urticaria (including giant urticaria), laryngospasm and anaphylactic reaction have been reported with
Combivent® (ipratropium bromide and albuterol sulfate) Inhalation Aerosol, with positive rechallenge in some cases. Many of these patients had a history of allergies to other drugs and/or foods including soybean (see CONTRAINDICATIONS). Post-Marketing Experience
In a 5-year placebo-controlled trial, hospitalizations for supraventricular tachycardia and/or atrial fibrillation occurred with an incidence rate of 0.5% in COPD patients receiving Atrovent® (ipratropium bromide) Inhalation Aerosol CFC.
Additional side effects identified from the published literature and/or post-marketing surveillance on the use of ipratropium bromide-containing products (singly or in combination with albuterol), include: urinary retention, mydriasis, bronchospasm (including paradoxical bronchospasm), cases of precipitation or worsening of narrow-angle glaucoma, acute eye pain, blurred vision, ocular irritation, nasal congestion, drying of secretions, mucosal ulcers, irritation from aerosol, wheezing, exacerbation of COPD symptoms, hoarseness, palpitations, heartburn, drowsiness, CNS stimulation, coordination difficulty, flushing, alopecia, itching, hypotension, edema, gastrointestinal distress (diarrhea, nausea, vomiting), constipation, hypokalemia, mental disorder, hyperhidrosis, muscle spasms, muscular weakness, myalgia, and asthenia.
OVERDOSAGE
The effects of overdosage are expected to be related primarily to albuterol sulfate. Acute overdosage with ipratropium bromide by inhalation is unlikely since ipratropium bromide is not well absorbed systemically after aerosol or oral administration. Oral median lethal doses of ipratropium bromide were greater than 1001 mg/kg in mice (approximately 19,000 times the maximum recommended daily inhalation dose in adults on a mg/m2 basis); 1663 mg/kg in rats (approximately 62,000 times the maximum recommended daily inhalation dose in adults
on a mg/m basis); and 400 mg/kg in dogs (approximately 50,000 times the maximum recommended daily inhalation dose in adults, on a mg/m2 basis). Whereas the oral median lethal dose of albuterol sulfate in mice and rats was greater than 2,000 mg/kg (approximately 6,600 and 13,000 times the maximum recommended daily inhalation dose, respectively, in
adults on a mg/m basis), the inhalational median lethal dose could not be determined. Manifestations of overdosage with albuterol may include anginal pain, hypertension, hypokalemia, tachycardia with rates up to 200 beats per minute and exaggeration of the pharmacologic effects listed in ADVERSE REACTIONS. As with all sympathomimetic aerosol medications, cardiac arrest and even death may be associated with abuse. Dialysis is not appropriate treatment for overdosage of albuterol as an inhalation aerosol; the judicious use of a cardiovascular beta-receptor blocker, such as metoprolol tartrate may be indicated. DOSAGE AND ADMINISTRATION
The dose of COMBIVENT® Inhalation Aerosol is two inhalations four times a day. Patients may take additional inhalations as required; however, the total number of inhalations should not exceed 12 in 24 hours. Safety and efficacy of additional doses of COMBIVENT Inhalation Aerosol beyond 12 puffs/24 hours have not been studied. Also, safety and
efficacy of extra doses of ipratropium or albuterol in addition to the recommended doses of Combivent® (ipratropium bromide and albuterol sulfate) Inhalation Aerosol have not been studied. It is recommended to “test-spray” three times before using for the first time and in cases where the aerosol has not been used for more than 24 hours. Avoid spraying into eyes. HOW SUPPLIED
COMBIVENT Inhalation Aerosol is supplied as a metered-dose inhaler with a white mouthpiece that has a clear, colorless sleeve and an orange protective cap. The COMBIVENT Inhalation Aerosol canister is to be used only with the COMBIVENT Inhalation Aerosol mouthpiece and not with other mouthpieces. This mouthpiece should not be used with other aerosol medications. Each actuation meters 21 mcg of ipratropium bromide and 120 mcg of albuterol sulfate from the valve and delivers 18 mcg of ipratropium bromide and 103 mcg of albuterol sulfate (equivalent to 90 mcg albuterol base) from the mouthpiece.
Each 14.7 gram canister provides sufficient medication for 200 actuations (NDC 0597-0013-14).
Warning: The canister should be discarded after the labeled number of actuations has been used. The correct amount of medication in each actuation cannot be assured after this point, even though the canister is not completely empty. Store at 25°C (77°F); excursions permitted to 15°-30°C (59°-86°F) [see USP Controlled Room Temperature]. For best results, store the canister at room temperature before use. Avoid excessive humidity. Shake the canister vigorously for at least 10 seconds before use. Address medical inquiries to: http://us.boehringer-ingelheim.com, (800) 542-6257 or (800) 459-9906 TTY. Note: The indented statement below is required by the Federal government’s Clean Air Act for all products containing or manufactured with chlorofluorocarbons (CFCs): Warning: Contains trichloromonofluoromethane (CFC-11), dichlorodifluoromethane (CFC-12) and dichlorotetrafluoroethane (CFC-114), substances which harm public health and the environment by destroying ozone in the upper atmosphere.
A notice similar to the above Warning has been placed in the information for the patient of this product under the Environmental Protection Agency’s (EPA’s) regulations. The patient’s warning states that the patient should consult his or her physician if there are any questions about alternatives. Contents Under Pressure: Do not puncture. Do not use or store near heat or open flame. Exposure to temperatures above 120°F may cause bursting. Never throw the inhaler into a fire or incinerator.
Boehringer Ingelheim Pharmaceuticals, Inc. Ridgefield, CT 06877 USA Ipratropium bromide licensed from: Boehringer Ingelheim International GmbH Copyright 2008 Boehringer Ingelheim Pharmaceuticals, Inc. ALL RIGHTS RESERVED U.S. Patent No. 5,603,918 Rev: November 2008 IT9011FK0408 10004145/04
Patient’s Instructions for Use
Combivent®
(ipratropium bromide and albuterol sulfate) Inhalation Aerosol Read complete instructions carefully before using
Use COMBIVENT Inhalation Aerosol exactly as prescribed by your doctor. Do not change your dose or how often you use COMBIVENT Inhalation Aerosol without talking with your doctor. Talk to your doctor if you have questions about your medical condition or your treatment. Tell your doctor about all of the medicines you take. COMBIVENT Inhalation Aerosol and some other medicines may interact with each other. Do not use other inhaled medicines with COMBIVENT Inhalation Aerosol unless prescribed by your doctor. 1. Insert metal canister into clear end of mouthpiece (see Figure 1). Make sure the
canister is fully and firmly inserted into the mouthpiece. The COMBIVENT Inhalation Aerosol canister is to be used only with the COMBIVENT Inhalation Aerosol mouthpiece. This mouthpiece should not be used with other inhaled medicines.
2. Remove orange protective dust cap. If the cap is not on the mouthpiece, make sure
there is nothing in the mouthpiece before use. For best results, the canister should be at room temperature before use.
3. Shake and Test Spray.Perform this step before using for the first time, and whenever the aerosol has not been used for more than 24 hours; otherwise, proceed directly to Step 4.
After vigorously shaking the canister for at least 10 seconds (see step 4 for instructions on shaking), “test-spray” into the air 3 times. Avoid spraying in eyes. 4. Shake the canister vigorously for at least 10 seconds. Hold canister as illustrated in IMPORTANT:Vigorous shaking for at least 10 seconds before each spray is very important for proper product performance. For best results, perform Steps 5-6 within 30 seconds of shaking the canister. 5. Breathe out (exhale) deeply through your mouth. Holding the canister upright as
shown in Figure 3, between your thumb and finger(s), put the mouthpiece in your mouth and close your lips. Keep your eyes closed so that no medicine will be sprayed into your eyes. Combivent® (ipratropium bromide and albuterol sulfate) Inhalation Aerosol can cause blurry vision, narrow-angle glaucoma or worsening of this condition or eye pain if the medicine is sprayed into your eyes.
6. Breathe in (inhale) slowly through your mouth and at the same time spray the product into your mouth.
To spray the product, firmly press once on the canister against the mouthpiece as shown in Figure 4. Keep breathing in deeply. 7. Hold your breath for 10 seconds, remove the mouthpiece from your mouth and breathe out slowly, as in Figure 5. 8. Wait approximately 2 minutes, shake the inhaler vigorously for at least 10 seconds again (as described in Step 4), and repeat Steps 5-7. 9. Replace the orange protective dust cap after use. 10. Keep the mouthpiece clean. Wash with hot water. If soap is used, rinse thoroughly
with plain water. Dry thoroughly before use. When dry, replace cap on the mouthpiece when not using the drug product.
11. Keep track of the number of sprays used and discard after 200 sprays. Even though
the canister is not empty, you cannot be sure of the amount of medicine in each spray after 200 sprays.
12. If your prescribed dose does not provide relief or your breathing symptoms become worse, get medical help right away. Note: The indented statement below is required by the Federal government’s Clean Air Act for all products containing or manufactured with chlorofluorocarbons (CFCs):
This product contains trichloromonofluoromethane (CFC-11), dichlorodifluoromethane (CFC-12) and dichlorotetrafluoroethane (CFC-114), substances which harm the environment by destroying ozone in the upper atmosphere.
The contents of Combivent® (ipratropium bromide and albuterol sulfate) Inhalation Aerosol are under pressure. Do not puncture the canister. Do not use or store near heat or open flame. Exposure to temperatures above 120°F may cause bursting. Never throw the container into a fire or incinerator. Keep COMBIVENT Inhalation Aerosol out of reach of children. Avoid spraying in eyes.
Address medical inquiries to: http://us.boehringer-ingelheim.com, (800) 542-6257 or (800) 459-9906 TTY.
Store at 25°C (77°F); excursions permitted to 15°-30°C (59°-86°F) [see USP Controlled Room Temperature]. For best results, store the canister at room temperature before use. Avoid excessive humidity. Distributed by: Boehringer Ingelheim Pharmaceuticals, Inc. Ridgefield, CT 06877 USA Ipratropium bromide licensed from: Boehringer Ingelheim International GmbH Copyright 2008 Boehringer Ingelheim Pharmaceuticals, Inc. ,ALL RIGHTS RESERVED U.S. Patent No. 5,603,918 Rev: November 2008 IT9011FK0408 10004145/04
MATERIAL SAFETY DATA SHEET Date of Issue: September 2, 2004 1. IDENTIFICATION OF THE MATERIAL AND SUPPLIER Product name Ziram Granuflo Fungicide Other names Product codes and pack sizes Chemical group Recommended use Formulation Supplier Bayer CropScience Pty Ltd ABN 87 000 226 022 Telephone Facsimile Emergency Telephone Number 180
STANSW Young Scientist Awards 2012 Winners Awards Ceremony: University of Western Sydney, Bankstown Campus Friday, 26 October 2012 Keynote Address: Dr Anne Musser, Palaeontologist, Australian Museum Models and Inventions MAJOR AWARD WINNERS YEARS 3-6 James De Mellow, Eastwood Public School, The G phone Macinley Butson, Mt Keira Demonstration School, A spoon full of medi
 Percent Change in Adjusted Meana FEV1 from Test-Day Baseline - Endpoint Analysis
Percent Change in Adjusted Meana FEV1 from Test-Day Baseline - Endpoint Analysis 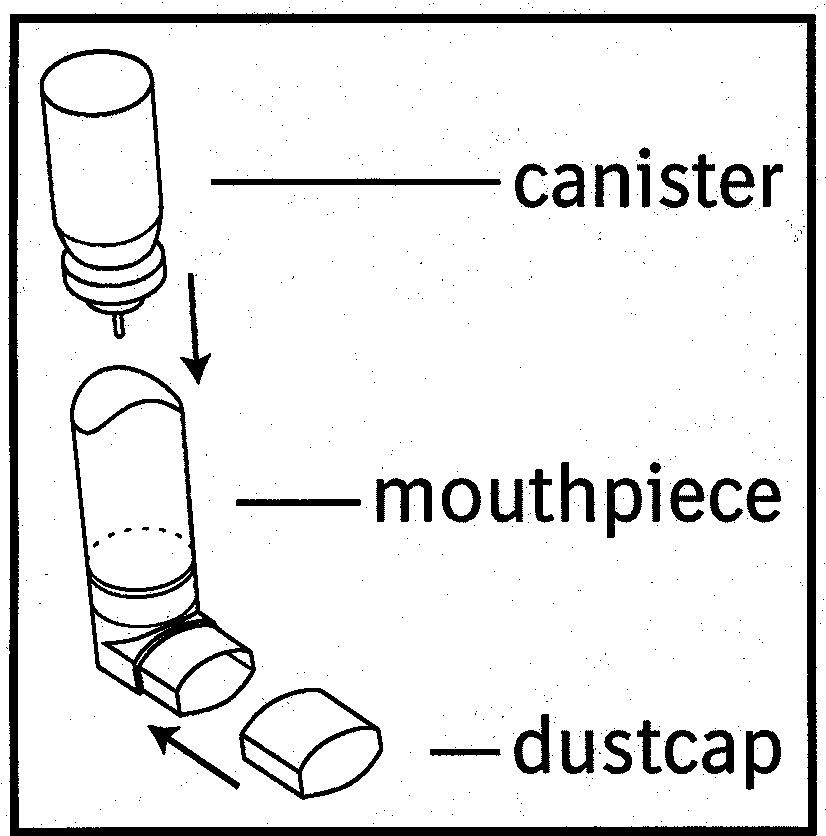 Patient’s Instructions for Use
Patient’s Instructions for Use 

 4. Shake the canister vigorously for at least 10 seconds. Hold canister as illustrated in
4. Shake the canister vigorously for at least 10 seconds. Hold canister as illustrated in  7. Hold your breath for 10 seconds, remove the mouthpiece from your mouth and
7. Hold your breath for 10 seconds, remove the mouthpiece from your mouth and