Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Pii: s8756-3282(01)00613-5
A Theoretical Analysis of the Contributions of Remodeling Space, Mineralization, and Bone Balance to Changes in Bone Mineral Density During Alendronate Treatment
1Rehabilitation Research and Development Center, VA Palo Alto Health Care System, Palo Alto, CA, USA2Biomechanical Engineering Division, Mechanical Engineering Department, and 3School of Medicine, Stanford University, Stanford, CA, USAIntroduction In patients with osteoporosis, alendronate treatment causes an increase in bone mineral density (BMD) and a decrease in
Osteoporosis patients treated with alendronate experience in-
fracture incidence. Alendronate acts by changing the bone
creased dual-energy X-ray absorptiometry (DXA)-derived areal
remodeling process. Changes in bone remodeling resulting in
bone mineral density (BMD) and reductions in vertebral fracture
decreased remodeling space, increased bone balance per
incidence of up to 50%.22 The increase in BMD caused by
remodeling cycle, and increased mineralization (ash mass/
alendronate has been attributed to decreased bone turnover,
bone mass) have all been associated with alendronate treat-
increased focal bone balance, and increased degree of mineral-
ment. Understanding the relative contributions of these pa-
ization of the bone tissue (expressed here as the ash fraction, ash
rameters to BMD increases could help predict the utility of
mass/bone mass). Although decreases in bone turnover have
long-term (>10 years) or intermittent treatment strategies,
been described quantitatively, it is not currently known howmuch focal bone balance and ash fraction contribute to BMD
as well as treatment strategies in which another pharmaceu-
increases relative to each other. Understanding the relative im-
tical is administered concurrently. We have developed a
portance of these factors can be important for understanding the
computer simulation of bone remodeling to compare the
changes in bone mechanical properties caused by alendronate. It
contributions of focal bone balance and mineralization on
could also be important for predicting which osteoporosis treat-
BMD by simulating alendronate treatment using a bone
ments would be most effective when combined with alendronate. balance method (decreased remodeling space, increased focal
In this work we summarize the findings of alendronate studies
bone balance, uniform bone mineralization) and a mineral-
and use them, in combination with a computer simulation of bone
ization method (decreased remodeling space, neutral focal
remodeling, to compare the influences of focal bone balance and
bone balance, varying bone mineralization). Although both
ash fraction during alendronate treatment. methods are able to predict BMD increases caused by alen-
Bone remodeling is a focal phenomenon involving groups of
dronate over short periods, our findings suggest that the
osteoclasts and osteoblasts known as basic multicellular units
mineralization method may be more descriptive of long-term
(BMUs). Each BMU resorbs a small portion of bone and, soon
alendronate treatment. This implies that mineralization may
after, forms new bone. Net changes in bone mass can occur when
be a larger contributor to BMD changes caused by alendro-
either the focal bone balance (a measure comparing the bone
nate than the focal bone balance. Based on this finding we
volume formed to that resorbed by each BMU) is modified or the
offer a hypothesis to describe how remodeling space, focal
rate of bone turnover changes (the size or number of BMUs is
bone balance, and mineralization each contribute to alendr-
modified). Alendronate treatment causes a significant decrease in
onate-induced BMD changes. Future analyses with this
bone turnover and a possible increase in the focal bone balance.4
method could be used to identify improved dosing regimens
An increase in the focal bone balance causes more bone volume
and to predict which osteoporosis treatments would best
to be formed at each remodeling site than is resorbed, increasing
complement each other. (Bone 29:511–516; 2001)
the total bone mass. A decrease in bone turnover has two
by Elsevier Science Inc. All rights reserved.
important consequences with regard to bone mass. First, adecrease in bone turnover causes a reduction in the remodeling
Key Words: Alendronate; Osteoporosis; Computer simulation;
space and a corresponding increase in bone volume.15 The
Bisphosphonates; Bone mineral density (BMD).
remodeling space represents the voids and osteoid that appeartemporarily due to the fact that resorption and osteoid formationprecede mineralized bone formation.14 When the rate of boneturnover is decreased fewer of these temporary voids are present,decreasing the size of the remodeling space but increasing thebone volume and bone mass. Address for correspondence and reprints: Christopher J. Hernandez,
The second important consequence of reduced bone turnover
Ph.D., The Mt. Sinai School of Medicine, One Gustave L. Levy Place,
involves the mineralization process in bone. A slower rate of
Box 1188, New York, NY 10029. E-mail: [email protected].
bone turnover allows bone to accumulate more mineral before
being resorbed in a succeeding remodeling cycle, thereby in-
Contributions to BMD changes during alendronate treatment
values are determined parametrically based on comparisons tothe results of clinical studies. The two simulation methods arecompared both by predictive ability (correlation with clinicalresults) and how they predict trends in BMD increases. Materials and Methods A BMU-based Model of Cellular Activity
A computer simulation of BMU activity in cancellous bone isused in this study. The model describes BMU activity in anarbitrary volume of cancellous bone defined by its bone volumefraction (mineralized bone volume/bulk volume). Nine indepen-dent remodeling parameters are used to describe the progressionof BMUs and the resulting resorption and formation of bone (seeAppendix). A feedback diagram illustrates how the model deter-mines changes in bone volume fraction and osteoid volume
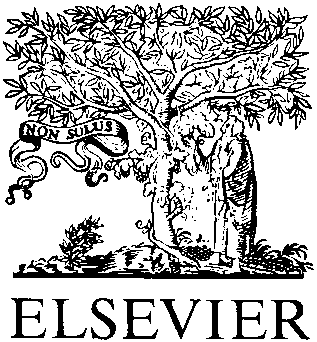
Figure 1. Conceptual illustration of the changes in BMD caused by
fraction (Figure 2). The key remodeling parameters in the BMU
alendronate treatment. The solid line represents the total BMD change
model are those related to bone balance per remodeling cycle,
caused by alendronate, whereas the dashed line represented the BMD
bone turnover, and bone mineralization.11 For this reason we
changes attributed to changes in bone turnover. The difference between
concentrate our analysis on remodeling parameters associated
the two lines represents the BMD increase attributed to focal bone
with focal bone balance (local resorption and formation rates),
balance changes. Variation in the degree of mineralization (ash fraction)
bone turnover (origination frequency), and the secondary miner-
is considered to be part of the bone turnover contribution. Adapted from
We express the focal bone balance as the ratio of bone
volume formed to that resorbed per remodeling site (the bone
creasing the average ash fraction of the bone tissue and the
balance ratio, ⌬BMU.Rt). The bone balance ratio is therefore
overall bone mass. Recently, it has been demonstrated that
dependent on the total volume of bone resorbed and formed at
animals subjected to alendronate treatment have an increased ash
each site (V , V in cubic millimeters per remodeling site):
fraction compared with placebo-treated controls.16 The magni-tude of ash fraction changes occurring in response to decreased
bone turnover is dependent on the length of the secondarymineralization period (P), a variable that has yet to be measured
If the volume resorbed (V ) does not equal the volume formed
(V ) per remodeling site there is a net gain or loss of bone. In the
Previously, Heaney and colleagues illustrated how alendro-
present study changes in focal bone balance are modeled as
nate treatment could be simulated as a decrease in bone turnover
decreases in the volume resorbed per remodeling site (corre-
and an increase in focal bone balance.10 Using their method of
sponding to decreased osteoclast activity). An investigation of
simulating alendronate treatment they were able to attribute part
how these parameters are derived from histology measurements
of the BMD increase to changes caused by bone turnover and
part to modification of the focal bone balance (Figure 1).
Bone turnover is evaluated experimentally using a two-di-
Although their model could predict the BMD changes in a
mensional histologic measurement known as the activation fre-
clinical study it accounted for only small variations in ash
quency (the rate of appearance of a BMU in a two-dimensional
fraction because it used a short (approximately 6 month) second-
section, per day). In this model we use a more physiologic,
ary mineralization period. It is likely that a greater portion of the
three-dimensional descriptive parameter known as the origina-
BMD increase that Heaney and colleagues attribute to bone
tion frequency (number of new BMUs per square millimeter of
turnover and part of the increase attributed to focal bone balance
bone surface/day) to represent the birthrate of new BMUs on the
may actually be caused by increased ash fraction. To study this
cancellous bone surface. Quantitative values for the origination
possibility we propose two methods of simulating alendronate
frequency are calculated using a relationship between activation
treatment: a bone balance method, in which the ash fraction is
frequency and origination frequency that has been derived pre-
maintained constant and alendronate causes a decrease in bone
viously.13 The origination frequency is calculated using param-
turnover and an increase in focal bone balance; and a mineral-
eter values based on those measured in healthy postmenopausal
ization method, in which alendronate treatment is simulated with
a change in bone turnover and a resultant change in ash fraction,
The rate at which mineral accumulates in newly formed bone
leaving the focal bone balance unchanged.
tissue is the final parameter that influences BMD predictions. A
The primary objectives of this study are to compare the bone
volume of osteoid becomes mineralized bone when small min-
balance method and mineralization method with regard to their
eral crystals first appear within spaces between the collagen
ability to predict BMD changes caused by alendronate. To meet
molecules. Over the first few days of mineralization, crystals
this objective we develop a model of the bone remodeling
appear throughout the mineralized bone, taking space that was
process utilizing quantitative histologic measurements of BMU
previously occupied by water. This initial deposition of mineral
activity. The model is implemented in a computer simulation
occurs very quickly and is referred to as the primary mineraliza-
using both the bone balance method and the mineralization
tion phase. After the primary mineralization phase mineral con-
method. Each of these methods utilizes one influential parameter
tinues to accumulate, most likely due to further increases in the
value that has not yet been measured definitively in humans (the
number or size of crystals. During this secondary mineralization
change in focal bone balance caused by alendronate for the bone
phase, mineral is added at an exponentially decreasing rate.17
balance method and the length of the secondary mineralization
Because mineral accumulates by displacing water present in the
period for the mineralization method). The unknown parameter
matrix there is a limit to the amount of mineral that can be
Contributions to BMD changes during alendronate treatment
Figure 2. A diagram of the computational model is presented with remodeling parameters in boxes and model outputs in ovals. Starting at the left, the number of progressing BMUs at a point in time is modified by the number of new BMUs forming (based on the origination frequency) and the number of BMUs that are terminating (based on the BMU lifespan). Each progressing BMU begins a remodeling cycle that continues through a resorption period, reversal period, mineralization lag time, and formation period. The model tracks the BMU population history so that the total number of BMUs that are actively resorbing or forming bone can be identified at any point in time. The sum of all actively resorbing bone is used along with the local resorption rate to determine the volume of bone that is resorbed at any point in time. Likewise, the sum of all actively forming bone or osteoid is used, along with the local formation rate, to determine the volume of bone that is formed and the change in osteoid volume at any point in time. The difference between the volume of bone formed and that resorbed determines the change in bone volume fraction. The change in osteoid volume is used to determine the osteoid volume fraction. The bone volume fraction determines the surface area available for remodeling and therefore influences the number of new BMUs that originate in the next time step.
present in the bone (this would occur if all water was displaced
simulation with a neutral focal bone balance, no initial remod-
by the mineral and is referred to as the theoretical maximum
eling activity (no osteoid), and a bone volume fraction (0.20)
mineralization). We define the secondary mineralization period
typical of cancellous bone in the lumbar vertebrae. After the
(P, years) as the time between the end of the primary mineral-
simulation was initiated, new BMUs originated, and resorption
ization phase and the point at which the mineral content reaches
and formation occurred, removing and replacing bone volume
95% of the theoretical maximum mineralization (where the
and bringing the system to an equilibrium state. The equilibrium
theoretical maximum ash fraction is 0.70; Figure 3). The length
state was used as the initial state from which model parameters
of the secondary mineralization period has been estimated to be
were modified to simulate alendronate treatment. Results are
Ͼ6 months,18 but could last many years.8
expressed in terms of percent change in BMD from the equilib-rium state. Simulations of Alendronate Treatment
Alendronate’s effects on BMU activity were modeled using
both the bone balance method (decreased remodeling space,
All model simulations were performed on a Silicon Graphics O2
increased focal bone balance, and uniform bone mineralization)
workstation (SGI, Mountain View, CA) using functions defined
and the mineralization method (decreased bone remodeling
for use with MATLAB (Mathworks, Natick, MA, USA). An initial
space, neutral focal bone balance, and varying bone mineraliza-
equilibrium state for the model was determined by starting the
tion). Chavassieux et al. showed that the activation frequencydecreases by 87% after 2 years of daily treatment with 10 mg oralalendronate.4 In our model we assume that a similar change inthe origination frequency occurs in each simulation method(since the activation frequency is directly related to the origina-tion frequency13). Comparison of the two methods was per-formed using values for the unknown parameters (secondarymineralization period and focal bone balance) that predict theBMD changes found in clinical studies administering 10 mg/dayof oral alendronate.3,6,21,22 The sum-of-squares for error (SSE)was used to determine how well the model predicts the results ofclinical studies:
Figure 3. Primary and secondary mineralization phases. The secondary
where BMD is the measured change in BMD, and BMD is the
mineralization period is defined as the time required for bone to miner-alize from 70% to 95% of the theoretical maximum ash fraction (a value
predicted change. The SSE and trends in the model predictions
were used to evaluate the two methods.
Contributions to BMD changes during alendronate treatment
Figure 4. The results of initial alendronate simulations using both the bone balance method (left) and the mineralization method (right) are presented. Data from clinical studies of 10 mg/day of oral alendronate treatment in patients with low initial bone mass3,6,21,22 are plotted along with model predictions. For the bone balance method, the bone balance ratio (⌬BMU.Rt) was initially unknown. A bone balance ratio of 2.0 gave good predictions of the clinical results (SSE ϭ 24.65). Bone balance ratio values of 1.0, 1.5, 2.0, and 3.0 corresponded to focal increases in bone volume of 0.0, 2.48e-05, 3.73e-05, and 4.97e-05 mm3 per remodeling site. For the mineralization method, the secondary mineralization period (P) was unknown. A 6 year secondary mineralization period well described the BMD changes found clinically (SSE ϭ 33.01).
parameter values based on histology data. It is therefore limitedby the assumptions upon which those data are based.19 In
Alendronate simulations using the bone balance method pre-
addition, the focal bone balance was assumed to be neutral (the
dicted greater increases in BMD as the bone balance ratio
same amount of bone is formed as is resorbed with each remod-
became larger (Figure 4, left). Predicted BMD increases were
eling cycle) in all of the pretreatment simulations (equilibrium
sensitive to changes in the bone balance ratio, with changes after
states) used in this analysis. Individuals treated with alendronate
10 years predicted to be 12.87% for a bone balance ratio of 2.0,
may have a negative pretreatment focal bone balance (more bone
and 10.12% for a bone balance ratio of 1.5. A bone balance ratio
is resorbed than formed with each cycle). A neutral pretreatment
of 2.0 gave predictions of BMD increases similar to those found
focal bone balance was used in our analysis because a number of
in clinical studies (SSE ϭ 24.65). The bone balance method
placebo groups in alendronate studies3,21,22 have shown small or
predicted that BMD would continue to increase as long as
insignificant decreases in bone mass (most likely due to calcium
alendronate treatment was continued. The change in bone mass
supplementation and placebo effects) and a neutral pretreatment
caused by a reduction in the remodeling space alone is presented
focal bone balance allows the simulations to reflect changes in
in a simulation using the bone balance method with a neutral
bone mass caused by alendronate rather than those caused by
focal bone balance (⌬BMU.Rt ϭ 1.0; Figure 4, left). The
increase in BMD caused by remodeling space after 10 years was
We presented two different methods of simulating alendro-
nate’s effects on bone remodeling. Both methods showed similar
Simulations using the mineralization method showed that
sum-of-squares for error (SSE ϭ 24.65 for the bone balance
longer secondary mineralization periods resulted in greater in-
method, and SSE ϭ 33.01 for the mineralization method),
creases in BMD (Figure 4, right). A secondary mineralization
suggesting that either method could be used to predict BMD
period of 6 years resulted in good predictions of the results from
changes over the treatment periods that have already been stud-
clinical studies of alendronate (SSE ϭ 33.01). The change in
ied (up to 7 years). The two methods gave considerably different
BMD predicted with a 6 year secondary mineralization period
predictions for longer treatment periods. The bone balance
was 11.98% after 10 years, much greater than that predicted
method predicted a steady increase in BMD with alendronate
using a 1 year mineralization period (6.23%). Trends from the
treatment because the focal bone balance caused small increases
mineralization method simulations suggest that the rate of BMD
in bone volume during each remodeling cycle. The mineraliza-
increase was reduced after continued alendronate treatment.
tion method predicted that there is a maximum possible BMDincrease because there were limits on the degree of mineraliza-
Discussion
tion of bone (Figure 3). Although alendronate treatment has notbeen studied for periods of Ͼ7 years, BMD increases caused by
In this work we developed a computational model of bone
alendronate do not appear to be unlimited. In addition, the bone
remodeling and alendronate treatment. The model was designed
balance method required a bone balance ratio of 2.0 to predict the
to determine reasonable values for unknown parameters in the
results of clinical studies. It is unclear whether such high values
bone balance and mineralization methods and determine how
can occur for prolonged periods in humans. For these reasons it
well each model can predict the BMD increases measured clin-
is likely that the mineralization method is a better description of
ically. We found that the bone balance method, using a bone
the effects of alendronate on bone remodeling.
balance ratio of 2.0, and the mineralization method, using a
Our results support the findings of recent studies suggesting
secondary mineralization period of 6 years, can each predict the
that the degree of mineralization contributes more to the BMD
BMD increases observed in clinical studies of daily alendronate
increases caused by alendronate than the focal bone balance.
Chavassieux et al. showed that patients taking alendronate for
The model presented in this work is based on our current
2–3 years do not show significant increases in bone volume
understanding of the process of bone remodeling and uses
fraction,4 a result that would be expected in response to changes
Contributions to BMD changes during alendronate treatment
caused by alendronate may be lost if cellular activity returnsto pretreatment levels. If changes in bone turnover account formost of the increases in bone mass, a patient who discontinuesalendronate treatment may eventually lose most of the bene-fits of treatment. Second, the ash fraction is known to influ-ence bone strength differently than the bone volume fraction(mineralized bone volume/bulk volume).12 Areal BMD mea-surements do not differentiate between increases caused byash fraction and those caused by increased bone volumefraction. Because focal bone balance changes modify the bonevolume fraction, it is possible that BMD increases from ashfraction could change bone strength in a different way than thesame BMD increase caused by focal bone balance. This mayexplain why the decreased rate of fracture after alendronatetreatment (nearly 50% decrease after 3 years) appears to be solarge compared to the observed change in BMD (ϳ6%– 8%after 3 years).22
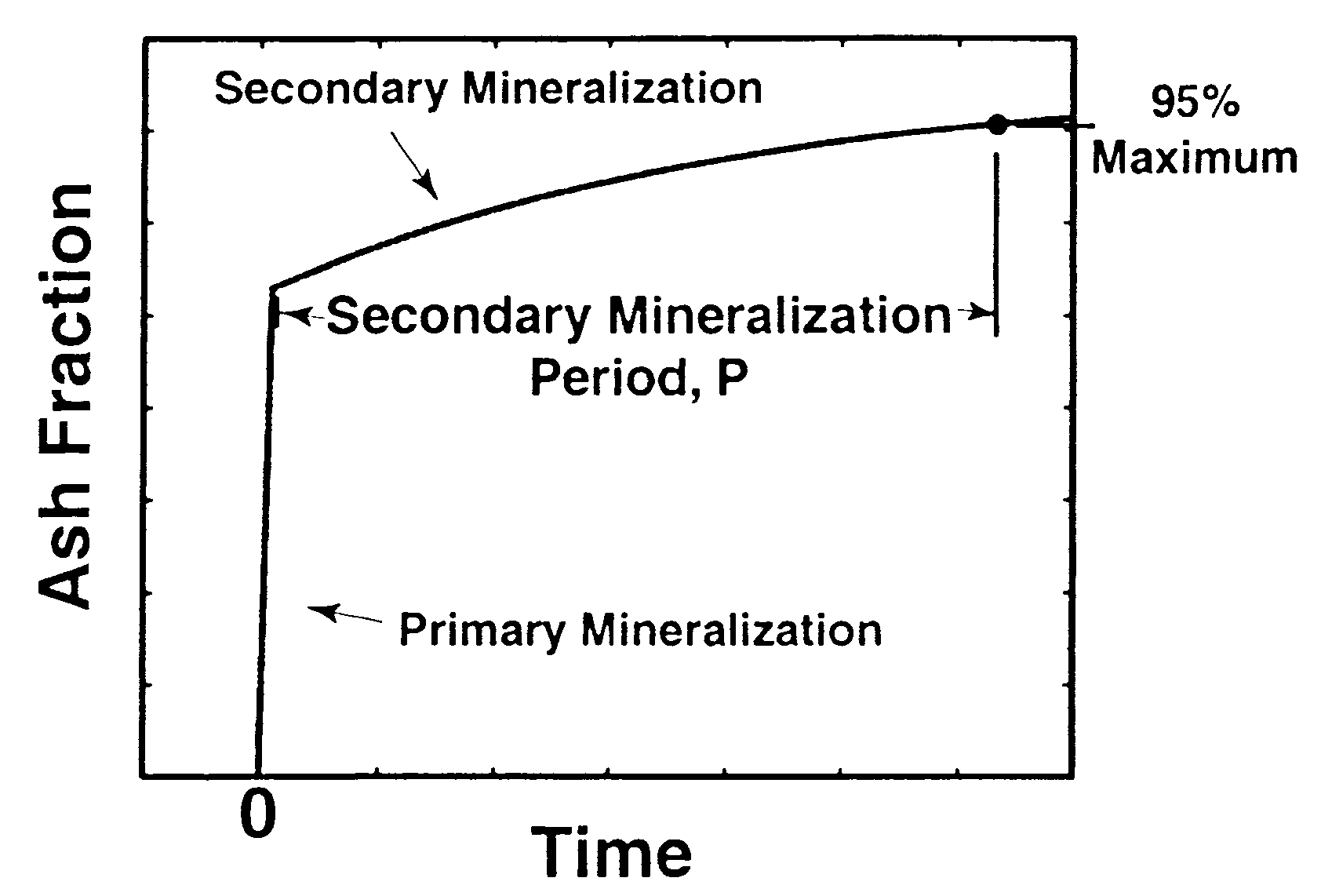
Figure 5. A theoretical description of the relative contributions of
With proper validation the model used in this work could
remodeling space, mineralization, and focal bone balance to BMDincreases during alendronate treatment. The solid line represents the total
predict changes in bone mass caused by a number of different
change in BMD. The dashed line represents the contribution caused by
agents. What we have presented here, however, is a useful tool
changes in the remodeling space alone. The dotted line represents the
for comparing ideas of how alendronate affects bone mass.
BMD changes predicted to be caused by both the remodeling space and
Future simulations based on this model could be used to
mineralization (ash fraction). As depicted, the focal bone balance con-
identify improved dosing regimens and to predict which other
tribution is smaller than the contribution caused by mineralization. It is
osteoporosis treatments (hormone replacement, parathyroid
possible that the BMD contribution caused by focal bone balance isnegligible.
hormone, and exercise) would best complement alendronatetreatment.
in the focal bone balance.16 In addition, the mean wall thicknessof bone formed does not appear to increase in response to
Appendix
alendronate treatment.4,5 If the erosion depth reached during
The BMU-based simulation examined here is adapted from a
resorption also remains unchanged the focal bone balance wouldbe neutral during alendronate treatment. Accurate measurement
model presented previously.11 The model uses nine indepen-
of the erosion depth and the focal bone balance is difficult,
dent parameters to describe BMU geometry and the resorption
however. Trends in the focal bone balance have been observed,
and formation process (Table A1). The volume resorbed and
but it is still unclear whether modification of the focal bone
formed per remodeling site (V , V ), shown in equation (1),
balance truly occurs in response to alendronate.4 A more recent
are related to the local resorption and formation rates (Rs.R,
study of patients taking alendronate2 found the changes in degree
of mineralization to be similar to the changes in BMD. Theinvestigators in this study concluded that changes in the degree
of mineralization may account for a majority of the BMDincrease caused by alendronate. These findings do not rule out
the possibility that focal bone balance is changed in response toalendronate. They do imply that, with regard to alendronate
The variables Rs.P and FP represent the length of time in which
treatment, the influence of focal bone balance on BMD increases
resorption and formation occur during a remodeling cycle (re-
is small compared to the influence of mineralization or the
sorption and formation periods in days) and Rs.R and FR
represent the rate at which bone volume is resorbed or formed
Heaney and colleagues attributed part of the increase in
(local resorption and formation rates in cubic millimeters per day
BMD caused by alendronate to the remodeling space and
per remodeling site). Initial values for the volume resorbed or
another part to the focal bone balance (Figure 1).10 Our
formed per remodeling site (V , V ) are calculated by defining
findings imply that changes in mineralization (ash fraction)
the shape of a BMU in cancellous bone (semiellipsoidal in cross
not only contribute to BMD changes after alendronate treat-
section with major radius equal to half the BMU width and minor
ment, but may explain most of the increase in BMD that was
radius equal to the erosion depth).11 The BMU width (equivalent
attributed to focal bone balance by Heaney et al. We therefore
to the diameter of a cortical BMU, 0.152 mm)1 and erosion depth
suggest that changes in remodeling space, changes in miner-
(for healthy postmenopausal women, 0.049 mm)7 are based on
alization (ash fraction), and increased focal bone balance all
contribute to alendronate-induced BMD increases, with the focal bone balance being the smallest contributor (Figure 5).
The initial values for the local formation and resorption rates
Changes in bone turnover are responsible for the changes in
are calculated from equations (A1) and (A2). Changes in the
remodeling space and ash fraction presented here, making
local formation and resorption rates by the same factor represent
bone turnover the single most important aspect of BMU
changes in the BMU shape (width or depth). Changes in local
activity that is modified by alendronate treatment. The impor-
formation and resorption rates by different factors result in
tance of bone turnover has two consequences with regard to
changes in the focal bone balance. This method of representing
alendronate treatment. First, changes in bone mass caused by
the focal bone balance allow us to differentiate between modi-
bone turnover are the result of a reduction in remodeling
fications in focal bone balance caused by changes in resorption
activity,9 implying that most of the benefits in bone mass
and those caused by changes in formation.
Contributions to BMD changes during alendronate treatment
Table A1. Independent parameters of basic multicellular unit (BMU) bone remodeling
Volume of bone resorbed per remodeling site per unit time
Volume of bone formed per remodeling site per unit time
Time during which resorption occurs at a remodeling site
Time between osteoclast and osteoblast activity
Time between osteoid formation and the start of mineralization
Time during which formation occurs at a remodeling site
Time required for bone to mineralize from 70% to 95%
aInitial value calculated using histology data. bValue based on histologic data for healthy postmenopausal women.7cValue based on estimates by Parfitt et al.20dEstimated values ranging from 6 months18 to many years.8
logic and metabolic influences on bone adaptation. J Rehabil Res Devel
Acknowledgments: This work was supported by the Department of
Veterans Affairs (A2424P) and a Dissertation Fellowship from the Ford
12. Hernandez, C. J., Beaupre´, G. S., Keller, T. S., and Carter, D. R. The influence
of bone volume fraction and ash fraction on bone strength and modulus. TransOrthopaed Res Soc 29:74 –78; 2001.
13. Jaworski, Z. F. G. Parameters and indices of bone resorption. Meunier, P. J.,
References
Ed. Bone histomorphometry, Second International Workshop. Lyon, France:Armour Montague; 1976.
1. Agerbaek, M. O., Eriksen, E. F., Kragstrup, J., Mosekilde, L., and Melsen,
14. Jaworski, Z. F. G. Parameters and indices of bone resorption. In: Bone
F. A. Reconstruction of the remodelling cycle in normal human cortical iliac
Histomorphometry, Second International Workshop, Lyon, France; 1976.
bone. Bone Miner 12:101–112; 1991.
15. Martin, R. B. On the significance of remodeling space and activation rate
2. Boivin, G. Y., Chavassieux, P. M., Santora, A. C., Yates, J., and Meunier, P. J.
changes in bone remodeling. Bone 12:391– 400; 1991.
Alendronate increases bone strength by increasing the mean degree of miner-
16. Meunier, P. J. and Boivin, G. Bone mineral density reflects bone mass but also
alization of bone tissue in osteoporotic women. Bone 27:687– 694; 2000.
the degree of mineralization of bone: Therapeutic implications. Bone 21:373–
3. Bone, H. G., Greenspan, S. L., McKeever, C., Bell, N., Davidson, M., Downs,
R. W., Emkey, R., Meunier, P. J., Miller, S. S., Mulloy, A. L., Recker, R. R.,
17. Parfitt, A. M. The physiologic and clinical significance of bone histomorpho-
Weiss, S. R., Heyden, N., Musliner, T., Suryawanshi, S., Yates, A. J., and
metric data. In: Recker, R. R., Ed. Bone Histomorphometry: Techniques and
Lombardi, A. Alendronate and estrogen effects in postmenopausal women with
Interpretation. Boca Raton: CRC; 1983; 143–224.
low bone mineral density. Alendronate/Estrogen study group. J Clin Endocri-
18. Parfitt, A. M. Bone remodeling and bone loss: Understanding the pathophys-
iology of osteoporosis. Clin Obstet Gynecol 30:789 – 811; 1987.
4. Chavassieux, P. M., Arlot, M. E., Reda, C., Wei, L., Yates, A. J., and Meunier,
19. Parfitt, A. M., Drezner, M. K., Glorieux, F. H., Kanis, J. A., Malluche, H., Meunier,
P. J. Histomorphometric assessment of the long-term effects of alendronate on
P. J., Ott, S. M., and Recker, R. R. Bone histomorphometry: Standardization of
bone quality and remodeling in patients with osteoporosis. J Clin Invest
nomenclature, symbols, and units. Report of the ASBMR Histomorphometry
Nomenclature Committee. J Bone Miner Res 2:595– 610; 1987.
5. Chavassieux, P. M., Arlot, M. E., Roux, J. P., Portero, N., Daifotis, A., Yates,
20. Parfitt, A. M., Mundy, G. R., Roodman, G. D., Hughes, D. E., and Boyce, B. F.
A. J., Hamdy, N. A., Malice, M. P., Freedholm, D., and Meunier, P. J. Effects
A new model for the regulation of bone resorption, with particular reference to
of alendronate on bone quality and remodeling in glucocorticoid-induced
the effects of bisphosphonates. J Bone Miner Res 11:150 –159; 1996.
osteoporosis: A histomorphometric analysis of transiliac biopsies. J Bone
21. Pols, H. A., Felsenberg, D., Hanley, D. A., Stepa´n, J., Mun˜oz-Torres, M.,
Wilkin, T. J., Qin-sheng, G., Galich, A. M., Vandormael, K., Yates, A. J., and
6. Chesnut, C. H., III, McClung, M. R., Ensrud, K. E., Bell, N. H., Genant, H. K.,
Stych, B. Multinational, placebo-controlled, randomized trial of the effects of
Harris, S. T., Singer, F. R., Stock, J. L., Yood, R. A., Delmas, P. D., et al.
alendronate on bone density and fracture risk in postmenopausal women with
Alendronate treatment of the postmenopausal osteoporotic woman: Effect of
low bone mass: Results of the FOSIT study. Foxamax International Trial Study
multiple dosages on bone mass and bone remodeling. Am J Med 99:144 –152;
Group. Osteopor Int 9:461– 468; 1999.
22. Tonino, R. P., Meunier, P. J., Emkey, R., Rodriguez-Portales, J. A., Menkes, C.,
7. Eriksen, E. F., Hodgson, S. F., Eastell, R., Cedel, S. L., O’Fallon, W. M., and
Wasnich, R. D., Bone, H. G., Santora, A. C., Wu, M., Desai, R., and Ross, P. D.
Riggs, B. L. Cancellous bone remodeling in type I (postmenopausal) osteopo-
Skeletal benefits of alendronate: 7-year treatment of postmenopausal osteoporotic
rosis: Quantitative assessment of rates of formation, resorption, and bone loss
women. J Clin Endocrinol Metabo 85:3109 –3115; 2000.
at tissue and cellular levels. J Bone Miner Res 5:311–319; 1990.
8. Frost, H. M. Bone Remodeling Dynamics. Springfield, IL: Thomas; 1963. 9. Heaney, R. P. The bone-remodeling transient: Implications for the interpretation of
clinical studies of bone mass change. J Bone Miner Res 9:1515–1523; 1994.
10. Heaney, R. P., Yates, A. J., and Santora, A. C., Jr. Bisphosphonate effects and
the bone remodeling transient. J Bone Miner Res 12:1143–1151; 1997.
11. Hernandez, C. J., Beaupre´, G. S., and Carter, D. R. A model of mechanobio-
A graph consists of a set of objects called Description vertices and a list of pairs of vertices, called edges . tures, with vertex A represented by a dotThe edge joining A to A is called a loop ,labelled A and each edge AB representedand the graph is called a loop multigraph . by a curve joining A and B . A general graph is one with possible loopsdata or relationshi
WHAT REGULATE THE GROWTH REGULATORS ? Logos Publisher, Kiev, 1998. ISBN 966-581-101-0Edited by B. A. Kurchii Institute if Plant Physiology and Genetics, 31/17 Vasylkivska Str. 03022 Kiev, UkraineDecember, 1998202 pages, illustratedPrice: $50.00Monograph is published in Russian (30%) and in English (70%). The papers presented in this book deal with the relationships between the structure of a
 A Theoretical Analysis of the Contributions of Remodeling
A Theoretical Analysis of the Contributions of Remodeling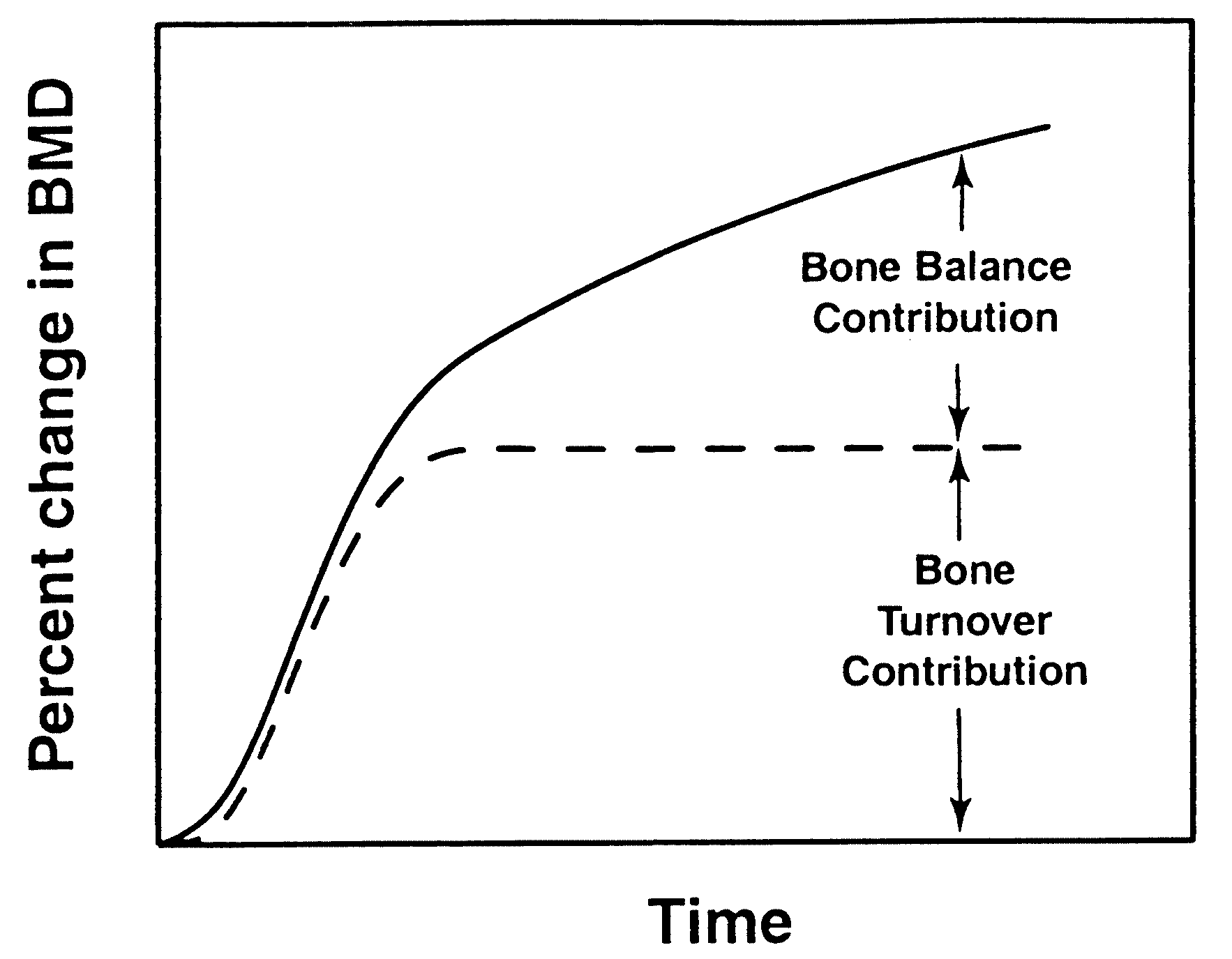 Contributions to BMD changes during alendronate treatment
values are determined parametrically based on comparisons tothe results of clinical studies. The two simulation methods arecompared both by predictive ability (correlation with clinicalresults) and how they predict trends in BMD increases.
Contributions to BMD changes during alendronate treatment
values are determined parametrically based on comparisons tothe results of clinical studies. The two simulation methods arecompared both by predictive ability (correlation with clinicalresults) and how they predict trends in BMD increases.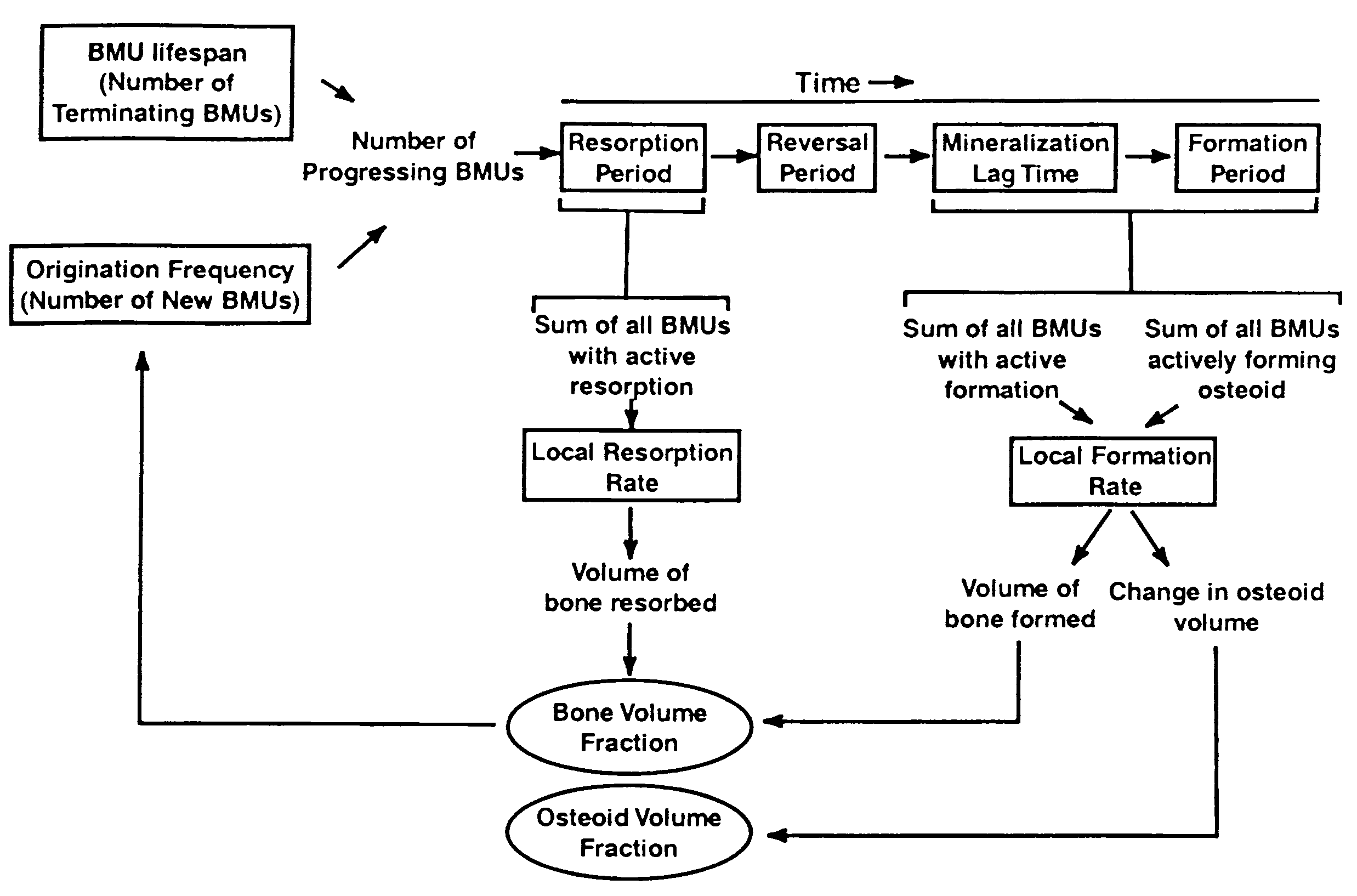
 Contributions to BMD changes during alendronate treatment
Figure 2. A diagram of the computational model is presented with remodeling parameters in boxes and model outputs in ovals. Starting at the left, the
Contributions to BMD changes during alendronate treatment
Figure 2. A diagram of the computational model is presented with remodeling parameters in boxes and model outputs in ovals. Starting at the left, the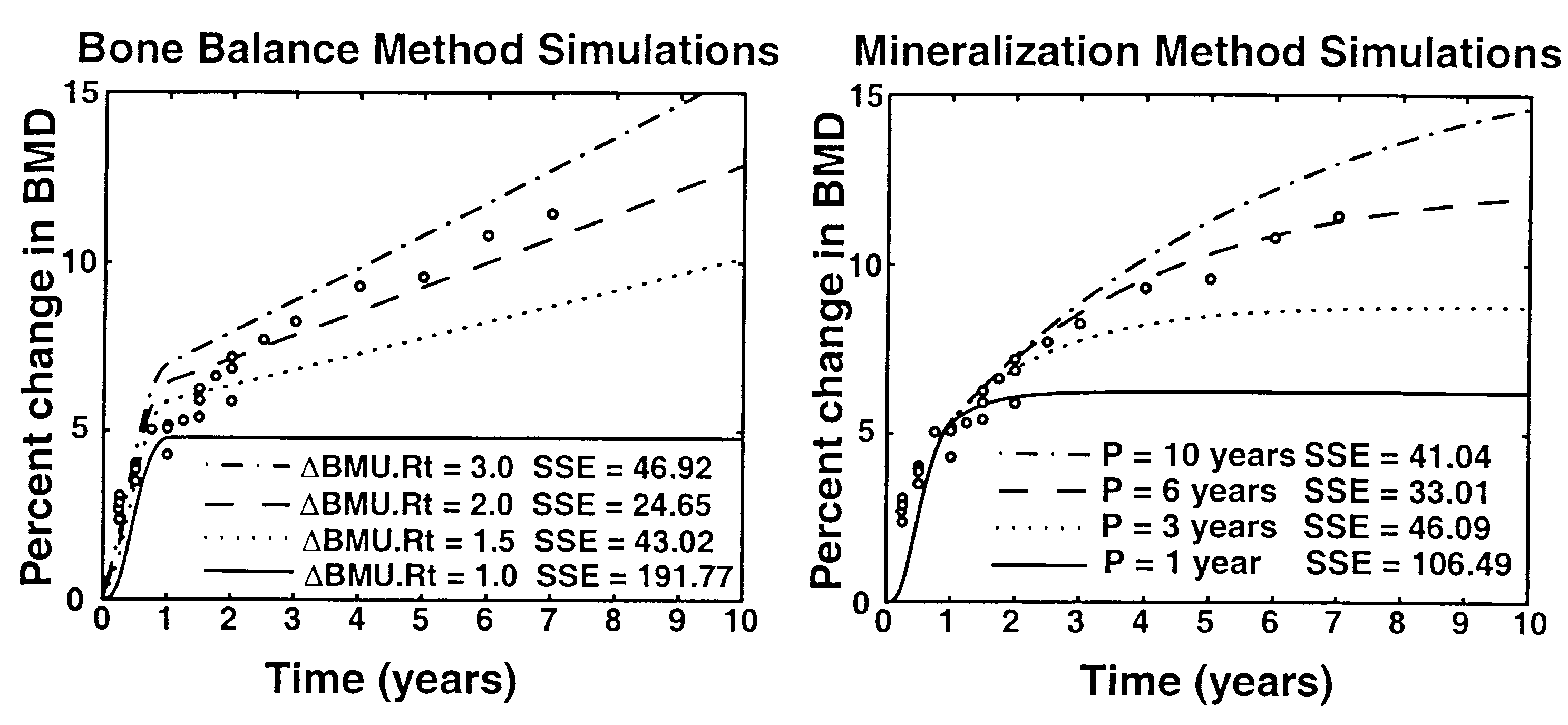 Contributions to BMD changes during alendronate treatment
Figure 4. The results of initial alendronate simulations using both the bone balance method (left) and the mineralization method (right) are presented.
Contributions to BMD changes during alendronate treatment
Figure 4. The results of initial alendronate simulations using both the bone balance method (left) and the mineralization method (right) are presented.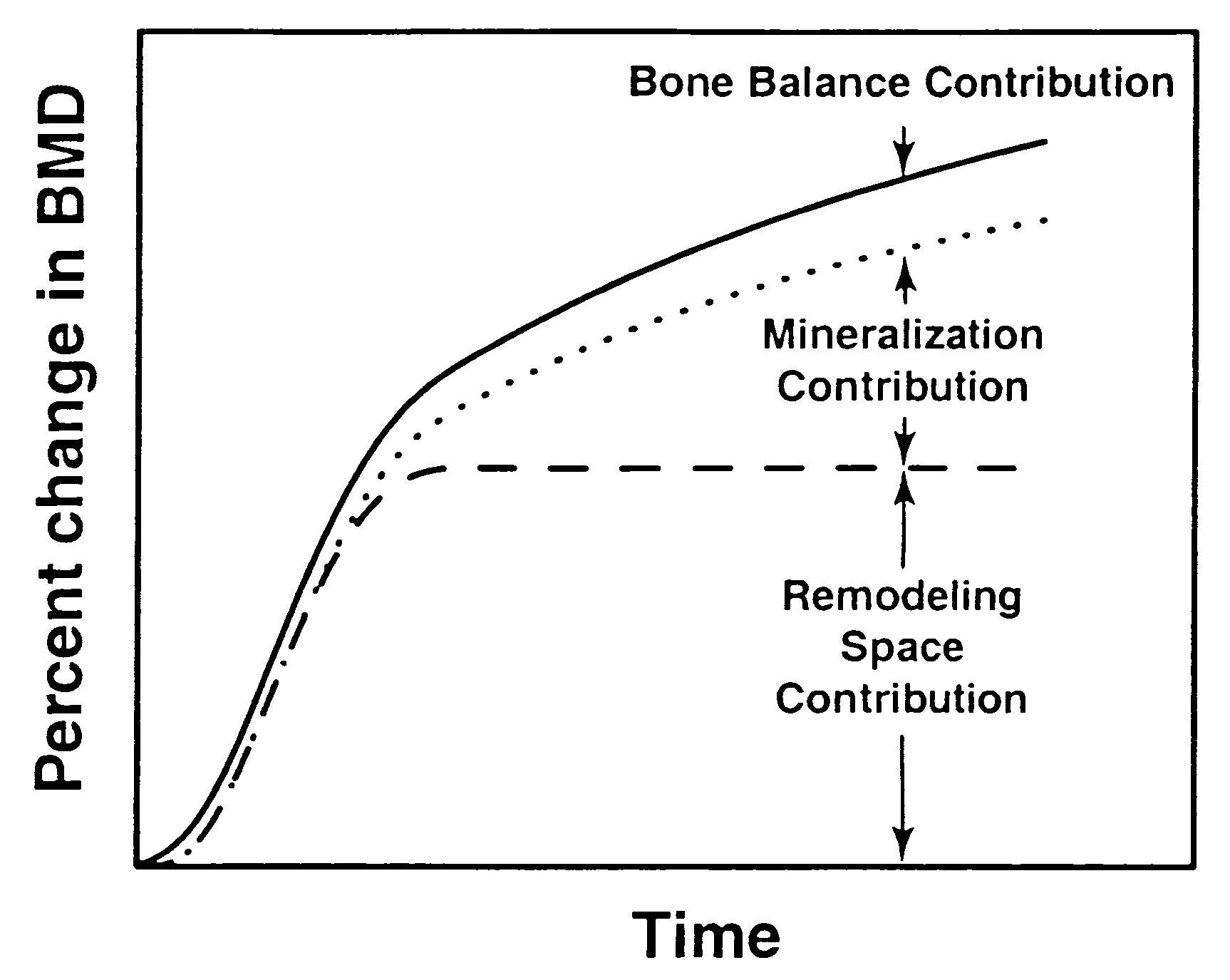 Contributions to BMD changes during alendronate treatment
caused by alendronate may be lost if cellular activity returnsto pretreatment levels. If changes in bone turnover account formost of the increases in bone mass, a patient who discontinuesalendronate treatment may eventually lose most of the bene-fits of treatment. Second, the ash fraction is known to influ-ence bone strength differently than the bone volume fraction(mineralized bone volume/bulk volume).12 Areal BMD mea-surements do not differentiate between increases caused byash fraction and those caused by increased bone volumefraction. Because focal bone balance changes modify the bonevolume fraction, it is possible that BMD increases from ashfraction could change bone strength in a different way than thesame BMD increase caused by focal bone balance. This mayexplain why the decreased rate of fracture after alendronatetreatment (nearly 50% decrease after 3 years) appears to be solarge compared to the observed change in BMD (ϳ6%– 8%after 3 years).22
Figure 5. A theoretical description of the relative contributions of
Contributions to BMD changes during alendronate treatment
caused by alendronate may be lost if cellular activity returnsto pretreatment levels. If changes in bone turnover account formost of the increases in bone mass, a patient who discontinuesalendronate treatment may eventually lose most of the bene-fits of treatment. Second, the ash fraction is known to influ-ence bone strength differently than the bone volume fraction(mineralized bone volume/bulk volume).12 Areal BMD mea-surements do not differentiate between increases caused byash fraction and those caused by increased bone volumefraction. Because focal bone balance changes modify the bonevolume fraction, it is possible that BMD increases from ashfraction could change bone strength in a different way than thesame BMD increase caused by focal bone balance. This mayexplain why the decreased rate of fracture after alendronatetreatment (nearly 50% decrease after 3 years) appears to be solarge compared to the observed change in BMD (ϳ6%– 8%after 3 years).22
Figure 5. A theoretical description of the relative contributions of