Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Microsoft powerpoint - hypertriglyceridaemia-05v2.ppt
Case Report: Massive Hypertriglyceridaemia
Graham RD Jones1, Alan Ting2, Kathy Samaras2, Don Chisholm2, David Segara3
Departments of Chemical Pathology1, Endocrinology2 and Surgery3, St Vincent’s Hospital, Sydney. 2 years prior Hospital Admission admission Day 0 Day 1 Day 2 Day 3 Day 4 Day 7 admission Total Cholesterol
Presented to Emergency Department with abdominal
Triglycerides HDL Cholesterol
Recent marked increase in ethanol consumption. LDL Cholesterol *
Noted on phlebotomy to have “milky” blood.
Family history of early cardiac mortality and
Table. Blood results prior to, during and after admission. Day 0 is day of admission. Admission blood results Admission blood samples highlighted in brown.
After routine centrifugation, serum was noted to be
Progress Discussion / Conclusions
Total cholesterol measured at 56 mmol/L and triglycerides at 237 mmol/L on diluted sample.
Treated with standard pancreatitis treatment.
This case of hypertriglyceridaemia is the most elevated in
our experience, although a triglyceride concentration of
Routine centrifugation for lipaemic samples not
270 mmol/L has been reported elsewhere (1). A number
effective (20 minutes at 10,000 x g).
Laboratory instructed to “keep spinning until clear
Sample preparation for routine biochemical analyses
with a microfuge was achieved, however several hours
Centrifugation for several hours required to produce
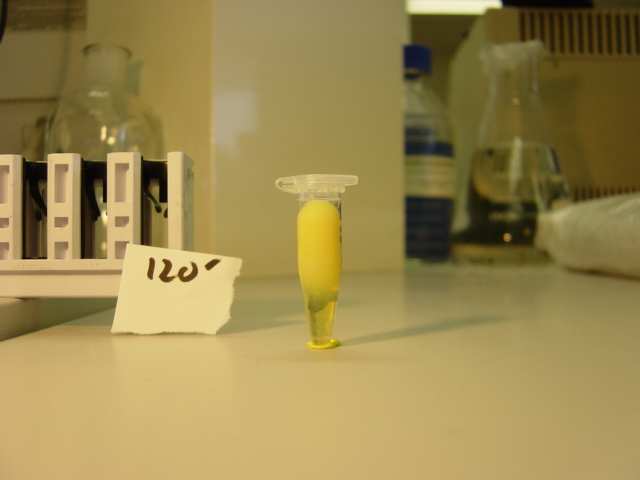
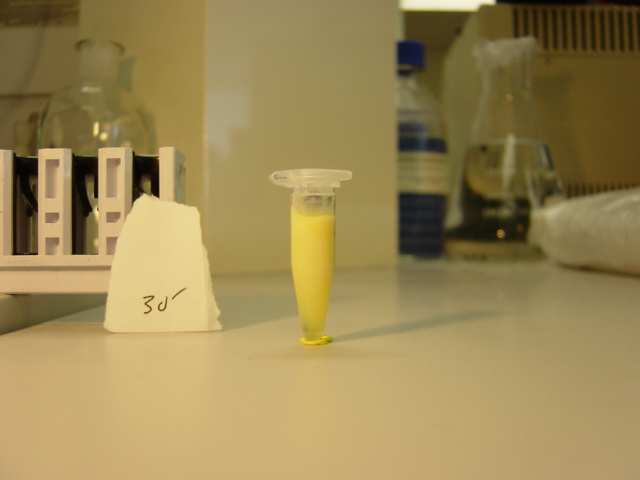
sufficient clear infranate for analysis (photos 2 - 5)
• Amylase and lipase increased (see table). • Triglycerides reduced to 170 mmol/L.
The initial molar ratio of triglycerides to cholesterol of
Initial blood results consistent with mild pancreatitis,
• Insulin and dextrose commenced (after 2nd blood
approximately 4:1 is consistent with chylomicron and
alcoholic hepatitis and massive hypertriglyceridaemia
VLDL remnants persisting due to lack of clearance by
Pancreatitis and fatty liver confirmed by imaging.
Cessation of food and ethanol lead to a rapid fall in
• Resolution of abdominal pain and pancreatic enzymes
serum triglycerides later augmented by insulin therapy. This rapid fall suggests a prominent role for ethanol in
• Identification of high LDL cholesterol concentration
Initial Serum
inhibition of clearance pathways in this case.
after resolution of gross hypertriglyceridaemia on day
Plasmapheresis was considered given the worsening
• Near complete resolution of lipid abnormalities on
pancreatitis and massive triglyceride concentration, but
30 minutes 60 minutes
conservative management was successful. centrifugation
During the convalescence a markedly elevated LDL
Progress Chart
cholesterol was seen, giving a “Familial Hypercholesterolaemia” pattern which later resolved to give a normal lipid profile. This has been reported
The cause of the hyperlipidaemia remains unresolved.
The patient was not diabetic. Genetic tests have not
120 minutes 180 minutes Acknowledgement / Reference
I thank the staff of the St Vincent’s Hospital Chemical
Pathology laboratory for their careful attention in the
handling of samples from this patient.
(1) Orth M, Luley C. Diagnostic pitfalls during therapy
for extreme hypertriglyceridaemia. Eur J Clin Chem
Photographs 1 to 5. Admission serum sample. 1 – after Figure 1. Graph of serum lipids and pancreatitis markers. routine centrifugation (10 minutes at 3000 x g). 2 to 5 – after centrifugation for the times shown at 10,000 x g. The thick blue line indicates the period of insulin infusion.
AACB Annual Scientific Meeting, Sydney, 2005
Annual Influenza Vaccine Consent Form-FLU SHOT and NASAL SPRAY Section 1: Information about Child to Receive Vaccine (please print) STUDENT’S NAME (Last) STUDENT’S DATE OF BIRTH month_________ day________ year __________ PARENT/LEGAL GUARDIAN’S NAME (Last) STUDENT’S AGE STUDENT’S GENDER PARENT/GUARDIAN DAYTIME PHONE NUMBER: SCHOOL NAME Section
Traveller’s Diarrhea This fact sheet provides basic information only. It must not take the place of medical advice, diagnosis or treatment. Always talk to a healthcare professional about any health concerns you have, and before you make any changes to your diet, lifestyle or treatment. What is traveller's diarrhea? Traveller's diarrhea is frequent, loose, or watery bowel movements resulti




 Case Report:
Case Report: