Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Wellcenteredmedicine.com
Initial History and Physical Exam
Is there an alternate contact if we cannot reach you?
Information About Your PainPlease describe your pain problem: What do you think is causing your pain? What does your family think is causing your pain? Do you think anyone is to blame for your pain? q Yes q No If so, who? Do you think surgery will be necessary? q Yes q NoIs there an event that you associate with the onset of pain? q Yes q No If so, what? How long have you had this pain? q < 6 months q 6 months – 1 year q 1 – 2 years q > 2 years
For each of the symptoms listed below, please “bubble in” your level of pain over the last month using a 10-point scale:
Pelvic pain lasting hours or days after intercourse
What would be an acceptable level of pain?
October 2007, The International Pelvic Pain SocietyThis document may be freely reproduced and distributed as long as this copyright notice remains intactDemographic InformationAre you (check all that apply):
What kind of work are you trained for? What type of work are you doing?
Health HabitsDo you get regular exercise? q Yes q No
What is your diet like? What is your caffeine intake (number per day, include coffee, tea, soft drinks, etc.)? q 0 q 1–3 q 4–6 q >6
How many cigarettes do you smoke per day?
Have you ever felt the need to cut down on your drinking? q Yes q NoHave you ever felt annoyed by criticism of your drinking? q Yes q NoHave you ever felt guilty about your drinking, or about something you said or did while you were drinking? q Yes q NoHave you ever taken a morning “eye-opener” drink? q Yes q No
What is your use of recreational drugs? q Never used q Used in past, but not now q Presently using q Choose not to answer
Have you ever received treatment for substance abuse? q Yes q No
Coping MechanismsWho are the people you talk to concerning your pain, or during stressful times?
How does your partner deal with your pain?
q Contact with clothing q Coughing/sneezing
Of all of the problems or stresses in your life, how does your pain compare in importance?
2007, The International Pelvic Pain Society
How old were you when your menses started?
Are you still having menstrual periods? q Yes q No
Answer the following only if you are still having menstrual periods:
Does pain start the day flow starts? q Yes q No
Starts days before flow starts: q Yes q No
Do you pass any clots in menstrual flow? q Yes q No
BladderDo you experience any of the following:
Loss of urine when coughing, sneezing, or laughing? q Yes q NoFrequent urination? q Yes q NoNeed to urinate with little warning? q Yes q NoDifficulty passing urine? q Yes q NoFrequent bladder infections? q Yes q NoFrequency of nighttime urination: q 0–1 q 2 or more
Frequency of daytime urination: q 8 or less q 9–15 q >16
Do you still feel full after urination? q Yes q No
Is there discomfort or pain associated with a change in the consistency of the stool (i.e., softer or harder) ? q Yes q NoWould you say that at least one-fourth (_) of the occasions or days in the last 3 months you have had any of the following
(Check all that apply)q Fewer than three bowel movements a week (0–2 bowel movements)q More than three bowel movements a day (4 or more bowel movements)q Hard or lumpy stoolsq Loose or watery stoolsq Straining during a bowel movementq Urgency – having to rush to the bathroom for a bowel movementq Feeling of incomplete emptying after a bowel movementq Passing mucus (white material) during a bowel movementq Abdominal fullness, bloating, or swelling
1 The Functional Gastrointestinal Disorders, Drossman, et al. Chapter 4, “Functional Bowel Disorders and Functional Abdominal
Gastrointestinal/EatingDo you have nausea?
Have you ever had an eating disorder such as anorexia or bulimia? q Yes q No
2007, The International Pelvic Pain SocietyShort-Form McGillThe words below describe average pain. Place a check mark (ü) in the column which represents thedegree to which you feel that type of pain. Please limit yourself to a description of the pain in yourpelvic area only. Type None (0) Mild (1) Moderate (2) Severe (3) Melzack, R: The Short-Form McGill Pain Questionnaire, Pain 30:191–197, 1987
Which statement(s) below best describes how you cope with the pain? Check all that apply
q I count numbers in my head or run a song through my mind
q I tell myself to be brave and carry on despite the pain
q I just think of it as some other sensation, such as numbness
q I tell myself that it really doesn’t hurt
q I worry all the time about whether it will end
q I do something active, like household chores or projects
SF-36In general, would you say your health is:
Compared to one year ago, how would you rate your health in general now?
The following items are about activities you mightdo during a typical day. Does your health now limityou in these activities? If so, how much?
Vigorous activities, such as running, lifting heavy
object, participating in strenuous sports
Moderate activities, such as moving a table,
pushing a vacuum cleaner, bowling, or playing golf
2007, The International Pelvic Pain Society
During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities because of yourphysical health?
Cut down the amount of time you spent on your work or other activities ¡ Yes
Accomplish less than you would like ¡ Yes
Were limited in the kind of work or other activities ¡ Yes
Had difficulty performing the work or other activities (for example, it took extra effort) ¡ Yes
During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities because of anyemotional problems (such as feeling depressed or anxious)?
Cut down the amount of time you spent on work or other activities ¡ Yes
Accomplished less than you would like ¡ Yes
Didn’t do work or other activities as carefully as usual ¡ Yes
During the past 4 weeks, to what extent has your physical health or emotional problems interfered with your normal social activitieswith family, friend, neighbors, or groups?
How much bodily pain have you had during the past 4 weeks?
During the past 4 weeks, how much did pain interfere with your normal work (including both work outside the home and housework)?
These questions are about how you feeland how things have been with youduring the past 4 weeks. For eachquestion, please give the one answer thatcomes closest to the way you have beenfeeling. How much of the time duringthe past 4 weeks:
During the past 4 weeks, how much of the time has your physical health or emotional problems interfered with your social activities(like visiting with friends, relatives, etc.?
¡ Some of the time ¡ A little of the time ¡ None of the time
How TRUE or FALSE is each of the followingstatements for you?
I seem to get sick a little easier than other people
2007, The International Pelvic Pain SocietyPersonal HistoryWhat would you like to tell us about your pain that we have not asked? Comments:
What types of treatments have you tried in the past for this pain?
q Acupuncture q Homeopathic medicine q Physical
What physicians or health care providers have evaluated or treated you for chronic pelvic pain? Include all healthcare professionals,whether they were physicians or not. Do you have any objections to me contacting these healthcare providers? q Yes q No
Physician/Provider City, State
Please list all surgical procedures you’ve had (related to this pain): Year Procedure Surgeon
Please list all other surgical procedures:
Year Procedure Year Procedure
Please list pain medications you’ve taken for your pain condition in the past 6 months, and the physicians who prescribed them (useseparate page if necessary):
Medication Physician Did it help?
q Yes q Noq Yes q Noq Yes q Noq Yes q Noq Yes q Noq Yes q Noq Yes q No
q I have written more medications on a separate page
2007, The International Pelvic Pain Society
Have you ever been hospitalized for anything besides surgery or childbirth? q Yes q No
Have you had major accidents such as falls or back injury? q Yes q NoHave you ever been treated for depression? q Yes q No Treatments: q Medication q Hospitalization q Psychotherapy
How many pregnancies have you had? Resulting in (#): Full 9 month
Any complications during pregnancy, labor, delivery, or post partum period?
Place an “X” at the point of your most intense pain. Shade in all other painful areas. 2007, The International Pelvic Pain SocietySexual and Physical Abuse HistoryHave you ever been the victim of emotional abuse? This can include being humiliated or insulted. q Yes q No q No answer
Circle an answer for both as a child and as an adult.
Fast-gradient Microbore Column-Switching LC-MS/MS for the QuantitativeG. Hopfgartner, C. Husser, M. Zell, Department of Non-Clinical Drug Safety,F. Hoffmann-La Roche Ltd, Pharmaceuticals Division, CH-4070 Basel, SwitzerlandProceedings 48th ASMS Conference on Mass Spectrometry and Allied Topics, Long Beach, CA, USA, 2000 Introduction The examination of pharmacokinetic properties of drugs in dis
BIZTONSÁGI ADATLAP A 453/2010 EK, a 1907/2006 EK (REACH) és a 1272/2008 EK rendeletek (CLP-GHS) szerint. 1. SZAKASZ: AZ ANYAG/KEVERÉK ÉS A VÁLLALAT/VÁLLALKOZÁS AZONOSÍTÁSA 1.1. Term ékazonosító 1.2. Az anyag vagy keverék m egfelelő azonosított felhasználása, illetve ellenjavalt felhasználása Élelmiszeripar,gyógyászat,fájdalomcsillapítóazonosítot felhaszná
 Initial History and Physical Exam
Initial History and Physical Exam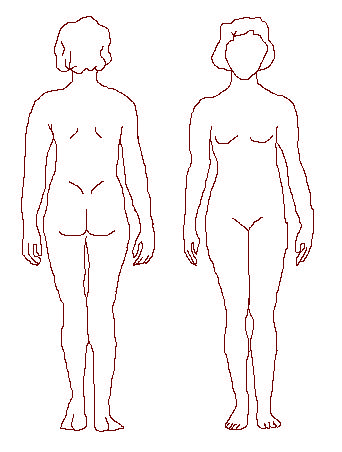 Have you ever been hospitalized for anything besides surgery or childbirth? q Yes q No
Have you had major accidents such as falls or back injury? q Yes q NoHave you ever been treated for depression? q Yes q No Treatments: q Medication q Hospitalization q Psychotherapy
How many pregnancies have you had? Resulting in (#): Full 9 month
Any complications during pregnancy, labor, delivery, or post partum period?
Place an “X” at the point of your most intense pain.
Have you ever been hospitalized for anything besides surgery or childbirth? q Yes q No
Have you had major accidents such as falls or back injury? q Yes q NoHave you ever been treated for depression? q Yes q No Treatments: q Medication q Hospitalization q Psychotherapy
How many pregnancies have you had? Resulting in (#): Full 9 month
Any complications during pregnancy, labor, delivery, or post partum period?
Place an “X” at the point of your most intense pain.