Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
City chiropractic registration and history, dated _____________________________
Name ___________________________________________
Are you here to address a specific problem?_______________________________________________
Birth date: _______________________ Age: __________
_______________________________________________
Cel Phone: _____________________________________
Is the condition worsening? YES NO UNKNOWN
Home Phone: ___________________________________
Address:________________________________________
____________________________, _____ ____________
Email: _________________________________________
Employer name __________________________________
How often? _____________________________________
Employment type: _______________________________
Seeking treatment due to a work accident?
Whom may we thank for referring you? _________________
How often/Type____________________________________Likes ____________________________________________
What are you hoping to get out of your massage today? _______________________________________________
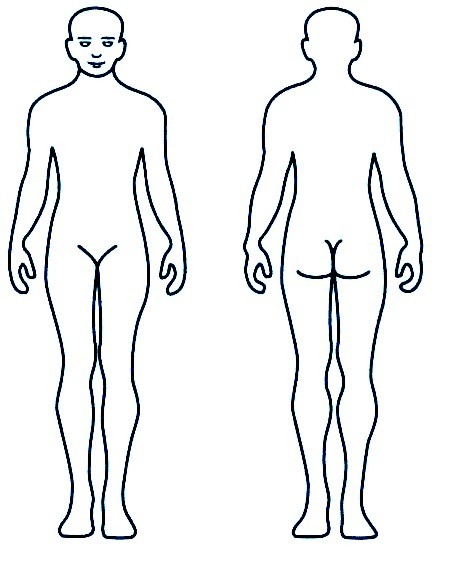
Mark an X on the picture where you'd like work addressed
Injuries/Surgeries you’ve had. These are important and may shed light on current postural issues, even if you don't think they were that bad at the time. Please include fender benders and the like, and injuries in childhood.
Description Date MVA's ___________________________________________________________________ _____________
Sprains/Strains ___________________________________________________________________ _____________
Head Injury ___________________________________________________________________ _____________
Broken Bones ___________________________________________________________________ _____________
Dislocations ___________________________________________________________________ _____________
Surgeries ___________________________________________________________________ _____________
Other ___________________________________________________________________ _____________
Do you have, or have you had in the past, any of the fol owing diseases (please circle):
Cancer, Heart disease, High Blood Pressure, Skin Conditions/Rashes, Diabetes, HIV/AIDS, Herpes, Headaches, Migraines, Kidney/Liver Disease, IBS, Celiac, Seasonal Allergies, Psychiatric conditions.
Other/Details (Date of Onset, Frequency, Diagnosis, Tx/Rx). Please also list any conditions which are chronic or recurring, such as frequent infections or other dysfunction: ____________________________________________________________ _________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Are you currently on any medications, including over the counter pain kil ers or cold medicine? ________________________
Any family History of significant disease?__________________________________________________________________
Are you Pregnant? YES NO UNKNOWN Congrats! When is your due date?______________________
How do you tend to eat? (A huge meal a day/Lots of small meals) ___________________________________________________
Favorite foods? _____________________________________________________________________________________
When you crave junk, do you go for sweets, or salt/fat? ______________________________________________________
Height _____________ Weight ________________ Al ergies ___________________________________________
Vitamins/Supplements ________________________________________________________________________________
Do you fal asleep easily?______________________________ Stay asleep through the night? _______________________
How many hours of sleep on average? _________________ Do you wake feeling rested? ___________________________
How's your water intake? __________________________________________ Do you carry a bottle? _______________
________________________________________________
________________________________________________
IFRIC Interpretation 6 Liabilities arising from Participating in a Specific Market— Waste Electrical and Electronic Equipment References IAS 8 Accounting Policies, Changes in Accounting Estimates and Errors IAS 37 Provisions, Contingent Liabilities and Contingent Assets Background Paragraph 17 of IAS 37 specifies that an obligating event is a past event that leads to a prese
Acta Neurol Scand 2012: 125: 96–104 DOI: 10.1111/j.1600-0404.2011.01499.xThe prevalence and demographicdistribution of treated epilepsy:a community-based study in Tasmania,AustraliaDÕSouza WJ, Quinn SJ, Fryer JL, Taylor BV, Ficker DM, OÕBrien TJ,Pearce N, Cook MJ. The prevalence and demographic distribution oftreated epilepsy: a community-based study in Tasmania, Australia. Acta Neurol Sc
 Name ___________________________________________
Are you here to address a specific problem?_______________________________________________
Birth date: _______________________ Age: __________
_______________________________________________
Cel Phone: _____________________________________
Is the condition worsening? YES NO UNKNOWN
Home Phone: ___________________________________
Address:________________________________________
____________________________, _____ ____________
Email: _________________________________________
Employer name __________________________________
How often? _____________________________________
Employment type: _______________________________
Seeking treatment due to a work accident?
Whom may we thank for referring you? _________________
How often/Type____________________________________Likes ____________________________________________
What are you hoping to get out of your massage today? _______________________________________________
Mark an X on the picture where you'd like work addressed
Injuries/Surgeries you’ve had. These are important and may shed light on current postural issues, even if you don't think they were that bad at the time. Please include fender benders and the like, and injuries in childhood.
Name ___________________________________________
Are you here to address a specific problem?_______________________________________________
Birth date: _______________________ Age: __________
_______________________________________________
Cel Phone: _____________________________________
Is the condition worsening? YES NO UNKNOWN
Home Phone: ___________________________________
Address:________________________________________
____________________________, _____ ____________
Email: _________________________________________
Employer name __________________________________
How often? _____________________________________
Employment type: _______________________________
Seeking treatment due to a work accident?
Whom may we thank for referring you? _________________
How often/Type____________________________________Likes ____________________________________________
What are you hoping to get out of your massage today? _______________________________________________
Mark an X on the picture where you'd like work addressed
Injuries/Surgeries you’ve had. These are important and may shed light on current postural issues, even if you don't think they were that bad at the time. Please include fender benders and the like, and injuries in childhood.