Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
019_mulvey_az
Neurocritical CareCopyright 2004 Humana Press Inc. All rights of any nature whatsoever are reserved. ISSN 1541-6933/04/3:XXX–XXX
Translational Research Multimodality Monitoring in Severe Traumatic Brain Injury The Role of Brain Tissue Oxygenation Monitoring Jamin M. Mulvey,1*, Nicholas W.C. Dorsch,2 Yugan Mudaliar,1 and Erhard W Lang,2
1Department of Intensive Care, University of Sydney,Westmead Hospital,Westmead Australia, and2Department of Neurosurgery University of Sydney,Westmead Hospital,Westmead Australia
Abstract
Traumatic brain injury (TBI) is a major cause of morbidity and mortalitywith widespread social, personal, and financial implications for those whosurvive. TBI is caused by four main events: motor vehicle accidents, sport-ing injuries, falls, and assaults. Similarly to international statistics, annu-al incidence reports for TBI in Australia are between 100 and 288 per 100,000. Regardless of the cause of TBI, molecular and cellular derangements occurthat can lead to neuronal cell death. Axonal transport disruption, ionic dis-ruption, reduced energy formation, glutamate excitotoxicity, and free rad-ical formation all contribute to the complex pathophysiological process ofTBI-related neuronal death. Targeted pharmacological therapy has not
*Correspondence and
proved beneficial in improving patient outcome, and monitoring and main-
reprint requests to:
tenance of various physiological parameters is the mainstay of current
therapy. Parameters monitored include arterial blood pressure, blood gases,
intracranial pressure, cerebral perfusion pressure, cerebral blood flow, and
brain tissue oxygenation. Currently, indirect brain oximetry is used for
cerebral oxygenation determination, which provides some information
regarding global oxygenation levels. Direct brain tissue oxygenation (ptiO2),
a newly developed oximetry technique, has shown promising results for
the early detection of cerebral ischaemia. ptiO2 monitoring provides a safe,
easy, and sensitive method of regional brain oximetry, providing a greaterunderstanding of neurophysiological derangements and the potential forcorrecting abnormal oxygenation earlier, thus improving patient outcome. This article reviews the current status of bedside monitoring for patientswith TBI and considers whether ptiO
2 ___________________________________________________________________________________Mulvey et al.Key Words: Brain tissue partial pressure of oxy-
Literature was identified through Medline and
gen; intracranial pressure; cerebral blood flow
PubMed searches using the key words autoreg-
velocity; monitoring; severe head injury; cerebral
ulation, brain tissue oxygen tension pressure,
ischaemia; transcranial Doppler ultrasound;
cerebral blood flow velocity, cerebrovascular
perfusion, Licox, severe head injury, and tran-scranial Doppler ultrasound (TCD). A reference
Introduction
library distributed by GMS (Kiel-Mielkendorf,Germany) and the senior author’s library was
Injury to the brain causes significant mor-
bidity and mortality through various mecha-nisms. Traumatic brain injury (TBI), regardless
Mechanisms of Cellular Injury:
of the cause, has profound personal, social, and
Primary and Secondary Injuries
financial implications to those directly and indi-rectly involved. TBI can be classified as mild,
Research over the past 20–30 years has elicit-
moderate, or severe. Severe TBI, which is the
ed much information on the mechanisms lead-
main focus of this review, is clinically defined
ing to neuronal cell death. It has been shown
as any head injury that results in a postresusci-
that in both human and animal tissues, regard-
tation Glasgow Coma Scale of 8 or less on admis-
less of the precipitating factors (i.e., traumatic,
sion or during the ensuing 48 hours (1). Studies
ischaemic, hypoglycaemic), the basic mecha-
of hospital admissions report that over 80% of
nisms underlying neuronal degeneration and
TBI admissions are for mild-to-moderate injury,
eventual death share similar cellular and molec-
whereas severe TBI accounts for 5–15% (2–4).
The overall mortality of patients with severe TBI
The processes that contribute to neuronal Fig 1
who survive to reach hospital is between 25 and
damage after injury can be classified into two
main groups: the primary injury and the sec-
ondary injury (17–19). Direct brain injury, or the
and secondary injury allows intensive care
primary injury, results from both the direct
physicians and neurosurgeons to target thera-
impact to the brain and the changing forces
py (8). Monitoring devices are used to detect
involved from the sudden deceleration at the
disturbances of physiological parameters with-
moment of impact. Large forces occur from
in the brain. Based on data obtained by multi-
acceleration, deceleration and rotation of the
brain inside the cranium. Shearing forces occur
measures may be used to correct abnormal val-
between tissue planes of varying densities
ues and potentially decrease patient morbidity
(20–22). This leads to immediate primary injury
and mortality. Because current neuroprotective
at the moment of trauma. The traumatic forces,
pharmacotherapy has not proven beneficial
as well as causing immediate structural dam-
(9–11), more emphasis is being placed on mon-
age to the neurons, cause secondary disruptions
itoring systemic and brain levels of physiolog-
in membrane stability, intra-axonal cytoskele-
ical parameters as well as substrate availability
tal function, and axonal transport mechanisms
(12–16). It is hypothesized that as monitoring
(20). Data from experimental models of TBI have
devices improve and by maintaining substrate
shown that postevent impairment of antero-
availability within the normal physiological
grade axoplasmic transport occurs, leading to
range, the extent of secondary injuries will be
local axonal swelling (23–25). With disorgani-
reduced and patient outcome will improve.
zation of microtubules and neurofilaments, con-
The purpose of this article is to review the
tinuation of this process leads to axonal
current status of bedside monitoring in the man-
disconnection, degradation, and distal degen-
agement of patients with TBI and evaluate the
role of direct brain tissue oxygenation moni-
Many aspects of the primary injury are imme-
toring (ptiO2) in the intensive care setting.
diate and irreversible, but it seems likely that a
Neurocritical Care ♦ Volume 1, 2004Monitoring Modalities in Traumatic Brain Injury _____________________________________________________3Fig. 1. A schematic diagram representing the molecular events implicated in secondary neuronal injury caused by ischemia. Regardless of the pathological etiology, the sequences of events are intimately related and lead to neuronal death.
continuum exists between the primary injury
flow. The aerobic metabolism of glucose includes
and the development of the secondary injury
the initial step of glycolysis, the tricarboxylic
(8). Although currently elusive, treatment aimed
acid cycle, and the electron transport chain.
Glucose is metabolized in the presence of oxy-
injury, or even the earlier cessation of the pro-
gen to produce a higher ATP yield than occurs
gression of the primary injury, may influence
under hypoxic conditions. For an in-depth
the management and outcomes of TBI (10,11).
review of this topic, see ref. 26.
Secondary injury after insult is correlated to
In an ischemic insult, loss of blood flow leads
impaired cerebral metabolism, hypoxia, and
to decreased availability of oxygen and glucose.
ischemia, and a complex series of events ensue.
Anaerobic metabolism is a largely inefficient
Although a detailed outline of these processes
form of energy production, and as a result, rapid
are beyond the scope of this article, a brief syn-
energy failure follows with decreased produc-
opsis of the mechanisms involved are present-
tion of ATP (27). With decreasing levels of ATP,
ed, including mechanisms that may be clinically
the physiological ionic homeostasis of the neu-
monitored in the intensive care unit (ICU).
ron is lost. Changes in the intracellular concen-tration of sodium, potassium, and calcium occur,
Cerebral Metabolism
leading to cellular injury and death. With pro-
Oxygen delivery is paramount to the normal
gressive switching to anaerobic metabolism, lac-
metabolism of neurons. It is used in a variety of
tate production rises sharply, as demonstrated
reactions within different cellular components
by the lactate/pyruvate ratio (28–31). Increased
to ultimately generate energy in the form of
lactate concentration and, therefore, tissue pH
adenosine 5’-triphosphate (ATP) by aerobic glu-
have been shown to correlate with a poor out-
cose metabolism. Aerobic metabolism is the
major source of energy formation in the brain,
and neuronal survival relies on an adequate sup-
ply of oxygen and glucose by cerebral blood
deranged as a result of ischemic events, and
Neurocritical Care ♦ Volume 1, 20044 ___________________________________________________________________________________Mulvey et al.
regional hypo- and hypermetabolism are known
mental studies (47,48). This effect was not repli-
to occur (36). Depressed cerebral activity, mito-
cated in TBI clinical trials using the calcium chan-
autoregulatory capacity of metabolic activity
significant improvement in outcome (16,49,50).
and substrate delivery have been strongly impli-
Glutamate Excitotoxicity Mitochondrial Dysfunction
during cerebral ischemia. Glutamate, an exci-
Mitochondria, which house the machinery for
tatory neurotransmitter, is released in larger
aerobic energy production, play an important
quantities during cerebral ischemia than dur-
role in aerobic metabolism. Mitochondrial dys-
ing normal physiological conditions and leads
function has been implicated in the impaired
to opening of glutamate receptors and further
activation of ion channels. Of particular signif-
episodes, including those resulting from TBI
icance is the sodium/calcium antiporter ion
(39,40). Although not completely understood,
channel, which leads to an acute increase of both
the contribution of mitochondria to cerebral
cations intracellularly (51). The N-methyl-D-
ischemic damage includes the impairment of
aspartate (NMDA) and a-amino-3-hydroxy-5-
ATP production, changes in mitochondrial per-
meability, and the release of factors that con-
glutamate receptors have been linked to the
tribute to cell death (41). The most widely
influx of calcium. The NMDA receptor directly
accepted hypothesis regarding mitochondrial
opens a calcium channel, allowing a rapid influx
dysfunction relates to the mitochondrial per-
of the calcium ion. The activated AMPA recep-
meability transition (MPT) (42,43). MPT occurs
tor opens a sodium channel allowing rapid
as a result of the abnormal opening of protein
influx of the sodium ion. Both ions, which are
channels between the inner and outer mito-
increased uncontrollably in ischemia, lead to the
chondrial membrane secondary to ischemia.
physiological derangements previously out-
This results in mitochondrial swelling, mem-
lined. Increased intracellular calcium concen-
brane depolarization, loss of oxidative phos-
trations also stimulate glutamate release from
phorylation, and the release of proapoptotic
presynaptic vesicles, further potentiating the
proteins (44). The ischemic induction of mito-
pathological process (52). Although it would
chondrial dysfunction is a potential target for
seem plausible that interventions targeting the
neuroprotective interventions and is currently
glutamate excitotoxic cascade would improve
outcomes in patients with TBI, clinical trialsusing the NMDA antagonist selfotel showed no
Calcium-Induced Cellular Damage
significant improvement in the outcome of TBI
Loss of calcium homeostasis, with calcium
entry into injured neurons, has long been asso-
Free Radical Formation
ciated with the process of delayed cell death(45,46). Calcium is physiologically important
Reperfusion injury caused by the production
because it acts as a messenger to regulate the
of free radicals has been theorized to contribute
activity of lipolytic enzymes, proteolytic
to secondary injury and delayed cell death.
enzymes, protein kinases, protein phosphatases,
Oxygen free radicals are formed by the reper-
and gene activation/expression. During insults
fusion-initiated metabolism of free fatty acids
such as ischemia or TBI, intracellular calcium
and arachidonic acid. The increased free radi-
increases uncontrollably and induces abnormal
cal formation leads to increased lipid peroxi-
cellular machinery leading to neuronal death.
dation, protein oxidation, and DNA damage
Calcium antagonism has shown its utility as a
(57). The integrity of the cellular lipid membrane
neuroprotective agent in preclinical experi-
is compromised, which leads to failure of ionic
Neurocritical Care ♦ Volume 1, 2004Monitoring Modalities in Traumatic Brain Injury _____________________________________________________5
partitioning and general cellular functioning,
known. With the high incidence of autoregula-
contributing to cell death. Clinical trials target-
tion dysfunction during TBI, global oxygena-
ing the various pathological pathways described
tion measurements may be in the normal range
above have been investigated (58–63). Trials
and not reflect abnormal regional differences.
using pegorgotein, tirilazad, or triamcinolone
Probes can be used to measure regional val-
have shown no significant improvement in over-
ues of brain tissue oxygen tension, carbon diox-
all morbidity or mortality in patients with TBI
ide tension, and hydrogen ion concentrations
(70,72–74). These multiparametric sensors areplaced adjacent to the ICP monitoring catheter
The Utility of Combined Monitoring
in the brain tissue via a modified skull bolt. Two
Overview
types of commercially available ptiO2 probes
currently exist: Licox® and Neurotrend®. The
venting or reducing secondary injury. Following
Licox probe (GMS, Kiel-Mielkendorf, Germany)
the poor results seen in pharmacotherapy clin-
uses a polarographic cell in which oxygen dif-
ical trials, current therapies focus on providing
fuses from the tissue through a polyethylene
an environment in which the body’s own cel-
wall of the catheter into its inner electrolyte
lular restorative processes are promoted.
chamber (Fig. 2A,B). Oxygen is transformed at
Systemic physiological parameters, including
the electrode, where it determines a current that
blood pressure, blood sugar level, electrolytes,
reflects the tissue partial pressure of oxygen.
and partial pressure of arterial dioxide (PaO
The oxygen-sensitive sampling area of the
polarographic gold cathode is approx 14 mm2.
addition, specific cerebral parameters are equal-
ly important in neurologic intensive care.
MA) uses optical sensors where dye, embedded
The neurological monitoring modalities cur-
in a plastic matrix, is connected to a fibreoptic
rently available can be classified into three types:
cable. Depending on the gas concentration and
pressure, flow, and oxygenation. Monitoring
pH of the surrounding tissues, the dye alters its
modalities include intracranial pressure (ICP)
properties, changing light transmission and
monitoring, TCD, and jugular venous oximetry
reflecting tissue partial pressure of oxygen. The
Neurotrend probe is comprised of four sensors
2). A new modality, which is still largely
used as an experimental modality, is ptiO
and is able to measure ptiO2, ptiCO2, pH, and
define ptiO2 as (32,66,71). The physiological data gathered by
temperature. The sampling area of the Au: Pls
using these monitoring modalities may allow
Neurotrend probe is approximately 2 mm2.
greater understanding of the complex sequence
ptiO2 probes generally are placed in the right
of events that influence the final outcome in TBI.
frontal lobe white matter in diffuse brain injury,
ICP and cerebral perfusion pressure (CPP) are
or on the affected side in a hemispheric injury,
the most important monitoring parameters on
and remain in situ for as long as ICP measure-
which therapeutic interventions are instituted.
ments are required (69,75). ptiO2 probes are read-
However, both reveal little in terms of cerebral
ily identified on computed tomography (CT)
scanning (Fig. 3). This allows for correct place-ment and the accurate detection of oxygenation
Invasive Cerebral Tissue Oxygen
in either normal or pericontusional brain. Monitoring
Currently available monitoring methods of
cerebral oxygenation and cerebral blood flow
models (76). Studies have shown that in TBI,
detect a “global” measurement. The data
ptiO2 values in patients with normal ICP and
obtained imply that the brain acts as a homog-
CPP are between 25 and 30 mmHg (77,78). The
enous structure; however, the heterogeneity of
critical threshold for ischemic damage and a
brain activity and substrate utilization is well-
poorer outcome has been proposed at ptiO2 val-
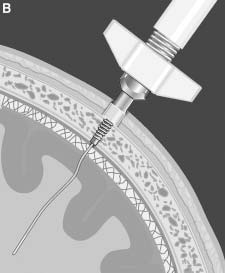
Neurocritical Care ♦ Volume 1, 20046 ___________________________________________________________________________________Mulvey et al.Fig. 2. (A) A schematic diagram of the Licox polarographic oxygenation probe.The numbered components of the diagram are: (1) polyethylene tube diffusion membrane; (2) polarographic gold cathode; (3) polarographic sil- ver anode; (4) cell filled with electrolyte; and (5) cerebral tissue. (B) A schematic diagram of the Licox probe illustrating placement via a cranial bolt into the cerebral tissues. Placement is similar to ICP monitoring and is often used through the same bolt.
ues of 10–15 mmHg (69,77,79,81). Critical thresh-
microenvironment, with low velocities show-
old is not the only factor that is important in
ing the highest variability in terms of oxygena-
terms of outcome; the duration spent below that
tion differences (83). At times, the disparity
between the different probe types can be appre-
The metabolic heterogeneity of different tis-
ciated, because sampling areas are quite differ-
sue types is well-known. It is important to fac-
tor the heterogeneous nature of the brain when
compensated for by a sufficiently large sensor
interpreting oximetry data. Experiments on rats
have demonstrated the differing ptiO2 within
Comparative Studies
the cortex depending on the depth of probeplacement (82). It was proposed that the differ-
ing base levels related to the metabolism, micro-
Cerebral blood flow is physiologically regu-
circulation, and overall microstructure of each
lated by several factors, including pressure of
environment. Furthermore, depending on the
blood flow, the pressures within the cranial
probe’s relationship to the arterial microvessels,
vault, and vascular autoregulatory processes.
a gradient within the tissues can exist with oxy-
Following TBI, alterations in ICP and CPP are
gen levels decreasing from artery to venous cir-
commonplace. A few studies have investigated
culation. The microenvironment is influenced
the association between CPP, ICP, and ptiO2. A
by the cerebral blood flow velocity of each
prospective study of 23 patients with TBI inves-
Neurocritical Care ♦ Volume 1, 2004Monitoring Modalities in Traumatic Brain Injury _____________________________________________________7
associated with higher ptiO2. This suggests thatthe critical threshold of CPP is 60 mmHg andthat ptiO2 is more sensitive than SjvO2 to changesin CPP. In contrast, Hartl et al. (85) report thattreatment of ICP with mannitol was not asso-ciated with improvements in ptiO2. However,it should be noted that in this study, ICP wastreated before it was severely raised (23 ± 1mmHg), and initial CPP before treatment was68 ± 2 mmHg.
Focal ischemic tissue may at times have nor-
mal CPP but decreased ptiO2. In a prospectivestudy of nine patients who demonstrated acutefocal lesions on CT scan and/or single photonemission computed tomography (SPECT) fromeither subarachnoid hemorrhage (SAH), TBI, ormeningioma, changes in ptiO2 were investigat-ed in relation to increased MAP and CPP (86). ptiO2 increased from 24 ± 13 mmHg to 31 ± 13 Au: Pls
mmHg in a positive linear fashion when CPP define MAPincreased from initial values of 77 ± 9 mmHg to96 ± 11 mmHg (r2 = 0.74). However, in somepatients with an initial ptiO2 below 20 mmHg,CPP was considered to be already within thenormal range. These data suggest that althoughCPP values above 60 mmHg are usually asso-
Fig. 3. A computer tomography image demonstrating
the position of a Licox oxygenation probe in the frontal
cortex of a patient with TBI. Oxygenation probes are
always accurate enough to assess brain tissue
readily identifiable on scanning modalities, illustrating
the position relative to contusional tissue and regions
form a major focus of current treatment inpatients with TBI. Although severe alterations
tigated the effects of aggressive treatment of CPP
of ICP and CPP are correlated with poor out-
when below 60 mmHg. Dopamine infusion was
come, studies suggest that other methods of
always associated with an increase in ptiO2 (66).
monitoring would provide additional, and at
Intervention led to significant elevations of CPP
times more sensitive, information regarding
from 32 ± 2 to 67 ± 4 mmHg and of ptiO2 from
cerebral blood flow and substrate availability.
13 ± 2 to 19 ± 3 mmHg. When initial CPP exceed-
Changes in ptiO2 are often detected concurrently
ed 60 mmHg, further CPP elevation did not sig-
with changes in CPP, but ptiO2 can be low (or
nificantly improve ptiO2, suggesting a plateau
even within the hypoxic range) even with nor-
phase of oxygenation. Another prospective
mal values of CPP (86). Arecent study has shown
study , comparing different methods of oxy-
that in 18 of 26 patients after aneurysmal SAH
genation monitoring in 17 patients with TBI
or severe TBI who had a unilateral decompres-
showed that decreases in CPP below 60 mmHg
sion hemicraniectomy for extensive cerebral
were significantly correlated with decreases in
oedema, pathological monitoring trends always
ptiO2 (84). Furthermore, changes in SjvO2 were
proceeded clinical deterioration (87). In 9 of 20
not significant when correlated with decreased
patients with SAH, decreases in ptiO2 occurred
CPP, and CPP values above 60 mmHg were not
several hours before neurological deterioration
Neurocritical Care ♦ Volume 1, 20048 ___________________________________________________________________________________Mulvey et al.
or ICP increase. This was not always the case
to CBF monitoring would provide increased
for patients with TBI. It is plausible that multi-
accuracy in interpreting CBF values.
modal monitoring of ICP, CPP, and ptiO2 could
Although investigators have reported on the
improve the sensitivity of detection of decreased
validity of cerebrovascular autoregulation
cerebral blood flow and substrate availability.
assessment and its prognostic relationship to
Therefore, early treatment interventions should
outcome, particularly related to CPP and CBFV,
increase the viability of injured and noninjured
few have compared the correlation between
neuronal tissue, thereby improving patient out-
autoregulation (88–90). It appears thatCBF/CBFV and ptiO
but during autoregulatory dysfunction and
Various investigators have studied the cor-
relation between CBF and ptiO2, particularly in
would at times provide misleading information
the initial periods of TBI when derangements
regarding potential ischemic episodes. A recent
in both CBF and ptiO2 are often at their great-
publication by of one the present authors study-
est. In considering these two clinical variables,
ing autoregulatory function of ptiO2 in 14
it is important to remember that ptiO2 reflects
patients with TBI, demonstrated a plateau phase
regional values, whereas CBF, depending on the
for the CPP–ptiO2 relationship similar to the
modality used, may reflect either macro- or
autoregulatory plateau seen in the relationship
between CPP and CBFV (71). When autoregu-
Doppenburg et al. investigated the correla-
lation was impaired, ptiO2 increased in a linear
tions between CBF (Xenon computed tomogra-
fashion with increases in CPP. If autoregulation
phy technique) and ptiO2 in 25 patients with TBI
remained intact, then increases in CPP had min-
and described a significant linear relationship
imal effect on ptiO2. It was concluded that
between the two modalities (r = 0.74, p = 0.0001)
manipulation of CPP was only of potential ben-
(32). Patients with increased CBF showed high-
efit in increasing brain oxygenation if autoreg-
er ptiO2, whereas those with decreased CBF had
ulatory mechanisms were dysfunctional.
a lower ptiO2, below 26 mmHg. All patients in
Furthermore, they suggested that continuous
this study with ptiO2 below 25 mmHg either
ptiO2 monitoring would provide more sensitive
information on the integrity of autoregulation
Dings et al. investigated the relationship
after TBI, directing accurate therapy.
between ptiO2, CBF velocity (CBFV), and CO2
Cerebral oxygen reactivity/autoregulation
reactivityin 17 patients with TBI (78). Low mean
has been assessed in patients with TBI by chang-
values for both ptiO2 and CBFV were seen on
ing the fractional inspired oxygen concentration
the day of injury (7.7 ± 2.6 mmHg and 60.5 ±
(FiO2) (33,91). The ability to increase ptiO is par-
32.0 cm/second, respectively). Both variables
ticularly useful in conditions where normal
increased, and by day 4 ptiO2 was 31.5 ± 10.0
autoregulatory function is impaired. By increas-
mmHg and CBFV was 87.9 ± 21.0 cm/second.
ing FiO2 from 35 to 100%, ptiO2 is able to be
The authors concluded that although ptiO2 and
increase to supranormal levels, allowing for aer-
obic metabolism. It has been proposed that FiO2
increased further, suggesting vasospasm and
manipulation can improve oxygenation better
uncoupling of flow and metabolism. To further
than CPP manipulation; however, patients with
support these findings, they discovered that at
a high oxygen reactivity (indicating a signifi-
times during increased CBFV, both CPP and
cant disturbance in autoregulation) have a poor-
ptiO2 were seen to decrease, indicating uncou-
pling or dysfunction of autoregulation. Thissuggests that ptiO2 monitoring as an adjuvant
Neurocritical Care ♦ Volume 1, 2004Monitoring Modalities in Traumatic Brain Injury _____________________________________________________9
stability was improved. Gopinath et al. also
global brain tissue oxygenation monitoring of
ately after insertion; however, values usually
patients with TBI since the early 1980s (92–94).
stabilized within 60 minutes (67). van den Brink
et al. reported low sensitivity drift (0 ± 6%) and
being used to detect ischemic episodes in
negligible zero drift in ptiO2 (68). All authors
patients with TBI (67,69,70,62,80,85). ptiO
ures direct regional oxygen tension levels, and
was a reliable method of detecting brain tissue
investigators have compared the utility of ptiO
ischemia over a prolonged period of time and
try, it is important to consider (a) calibration, (b)
The efficiency and quality of information
the time of good-quality data (TGQD), and (c)
gathered by the different methods of oximetry
can be quantified and compared. One methodis through the function of TGQD, expressed by
the equation: TGQD (%) = 100 – [time of arte-
The initial calibration of any monitoring
facts (minute) × 100/total monitoring time
device is crucial to obtaining accurate and reli-
able data. Based on the manufacturer’s recom-
In an investigation comparing ptiO2 and SjvO2
mendations, ptiO2 catheters are calibrated
monitoring in 15 patients with TBI and altered
before insertion and after withdrawal from the
CPP, TGQD and the total duration of monitor-
brain tissue; no intramonitoring calibration is
ing differed greatly between the two oximetry
possible. Two calibration parameters have been
methods (77). The median duration of moni-
described for ptiO2 catheters: sensitivity cali-
toring reported was 9 days (range: 5–12) for
bration and zero drift (68,70,77). Sensitivity cal-
ptiO2 and 4 days (range: 3–7) for SjvO2. TGQD
ibration is defined as the difference in measured
was reported at 95% (2491 hours total) and 43%
oxygen tension when room oxygen is measured,
(607 hours) for ptiO2 and SjvO2, respectively.
and zero drift is the difference in an oxygen-free
This difference in the SjvO2 arm was attributed
solution. Calibration of SjvO2 is based on co-
to poor light intensity in the system, repetitive
calibrations, and dislocations. Meixensberger et
every 10–12 hours for the duration of its usage.
al. reported similar disparities of TGQD between
ptiO2 and SjvO2 monitoring (96). This prospec-
have minimal drift during continuous moni-
tive study of 45 patients with TBI reported
toring. In a prospective study of 15 patients with
TGQD for ptiO2 and SjvO2 at 95 and 40–50%,
TBI comparing ptiO2 and SjvO2 monitoring,
respectively. Only five patients were monitored
ptiO2 monitoring showed low variability (3.7%
with SjvO2 for comparison because of increas-
sensitivity drift) and greater reliability over time
ing technical difficulties and poor reliability. (77). SjvO2 monitoring required a total of 170
Similar problems for SjvO2 have been reported
calibrations over 7 days, with 55% of calibra-
tions showing an increased drift (>5%) when
Dings et al. have also studied the reliability
compared with co-oximetry. In a study by Dings
of ptiO2 (70). Investigating the technical and
et al. reporting on the stability and complica-
diagnostic reliability of ptiO2 monitoring, 118
tions of ptiO2 monitoring in 70 patients with
catheter probes were used in 101 patients with
either TBI or SAH, 54 Licox catheters showed a
TBI. The TGQD was 99.2%, with artifacts relat-
drift of –6.2 ± 11.9% (95). Sensitivity drift was
ed to transport, positioning of the patient, and
greatest in situ during the first 4 days, after which
displacement of the catheter or the bolt. Dings
Neurocritical Care ♦ Volume 1, 200410 __________________________________________________________________________________Mulvey et al.
et al. concluded that ptiO2 was a safe and reli-
The technique of ptiO2 probe placement is
able technique for monitoring cerebral oxy-
almost identical to ICP monitor placement. Thus,
it seems plausible that ptiO2 probe could be
However, not all studies have found ptiO2 to
inserted by practitioners other than neurosur-
be superior to SjvO2 in the detection of critical
geons. Aretrospective study looking at the com-
ischemic episodes. A prospective study com-
plication rates of ICP probe insertion by
paring the utility of the methods in 65 patients
neurosurgeons, general surgical registrars, and
with TBI concluded that both modalities should
intensivists found no significant difference in
be used in conjunction and that neither identi-
complication rates between the different groups
fies all episodes of cerebral ischemia (67). Of 65
(98). They concluded that the use of non-neu-
patients, 7 were unable to have ptiO2 data col-
rosurgeons for the placement of probes could
lected because of technical difficulties. Of those
provide the prompt and early monitoring of
monitored, no significant difference was found
high-risk patients. We propose that it would be
in the TGQD, with values of 90 and 88% for SjvO2
safe practice to utilize non-neurosurgeons for
and ptiO2 monitoring, respectively (p = 0.524).
ptiO2 probe insertion; however, a neurosurgeon
Decreases in oxygenation were detected simul-
should be on standby if complications occur.
taneously in 90% of episodes; however, only 66%
Complication rates for SjvO2 monitoring are
of these episodes saw both modalities below
similarly low. Gopinath et al. reported zero com-
plications related to SjvO2 monitoring in 58patients (67). Kiening et al. reported dislodge-
ment as a main complication but did not quan-
Oximetry is an invasive procedure and car-
tify the rate (77). In a prospective study of 44
ries a potential for complications related to inser-
patients admitted to ICU for TBI, SAH, or stroke
tion and continuous monitoring. For routine
and requiring SjvO2 monitoring, complication
ICU purposes, probes are inserted via single or
rates were below 5% and were clinically insignif-
multiple lumen bolts if other monitoring modal-
ities are combined. Depending on the hospital’spolicies, bolts can be inserted in the ICU. In oper-
Brain Oxygenation and Outcome
ative cases, probes can be inserted directly dur-
No randomized control trials have been con-
ducted to demonstrate improved outcome with
In studies to date, complication rates for both
one monitoring modality over another. ICP mon-
ptiO2 and SjvO2 are low. Numerous studies
itoring has become routine practice in the neuro-
using ptiO2 have reported complication rates
ICU worldwide, although it has never been
below 3% (67,70,95). These complications
subjected to randomized controlled trials.
involved secondary hematoma formation, none
Uncontrolled intracranial hypertension is neg-
of which required treatment. The insertion trau-
atively correlated with outcome (100–102). It
ma can cause microhemorrhages and an odema
also seems plausible that reduced brain oxy-
zone around the probe tract (97). This has min-
genation would be correlated with a poorer out-
imal effect on measurements and does not com-
promise accuracy. Complications were related
Regardless of the lack of controlled trial data,
to technical issues such as the accidental removal
current clinical trials investigating the utility of
of the catheter during transport, broken catheter
ptiO2 suggest that prolonged periods of hypox-
cables, or unidentified technical problems. These
ia correlate with a poor outcome. van Santbrink
technical problems were reduced with experi-
et al. studied the utility of ptiO2 in 22 patients
ence, and larger studies have reported zero com-
with TBI and showed that hypoxic periods in
plication rates for the insertion of ptiO2 catheters
the acute posttraumatic phase was common (69).
More than 80% of patients showed prolonged
Neurocritical Care ♦ Volume 1, 2004Monitoring Modalities in Traumatic Brain Injury ____________________________________________________11
hypoxic periods less than 20 mmHg in the first
improved significantly over the past 30 years,
24 hours postinjury. In five patients, ptiO2 fell
mortality is still alarmingly high in those who
below 5 mmHg within the first 24 hours, and
survive to hospital. Because the pharmacologi-
four of those were either dead or partial vege-
cal management of TBI is currently poor and
tative state at 6 months. In the patients who had
still under extensive research, the integration
monitoring within the acute phase without a
and management of physiological variables
ptiO2 drop below 5 mmHg, 15 had good out-
remain the mainstay of current therapy.
come measures, and only 1 died or was vegeta-
tive at 6 months. ptiO2 was found to be strongly
attention and has generated regular interna-
tional meetings. Although it has become a rou-
Kiening et al. have also demonstrated poor
tine monitoring tool in several neurosurgical
outcome with reduced brain oxygenation in TBI
and neurological ICUs, it is still considered
(66). In 16 patients followed for 6 months postin-
experimental in other centers. Based on the data
jury, the number of ischemic episodes was asso-
available, it has been shown to provide a safe,
ciated with outcome. An ischemic episode was
easy-to-use, and accurate method of cerebral
defined as a ptiO2 less than 10mmHg for longer
oximetry determination. It can provide addi-
than 15 minutes. In the first week postinjury, the
tional, sensitive information regarding brain
numbers of ischemic episodes were always asso-
oxygen availability, autoregulation, and brain
ciated with a poorer outcome on the Glasgow
perfusion in patients with TBI. Compared to
Outcome Scale (GOS). Interestingly, absence of
other oximetry methods, ptiO2 has minimal
episodic hypoxia did not ensure a favorable out-
complications, increased accuracy, and greater
come. Bardt et al. also demonstrated poor out-
in situ monitoring time. ptiO2 often provides
come with prolonged ischemic episodes (81). In
more sensitive information than current moni-
35 patients with TBI, analysis of data showed
toring methods regarding regional CBF, CPP,
significant differences in outcome measures
ICP, and oxygen availability. Indeed, some cur-
rent therapeutic interventions used to manipu-
than 30 minutes. In patients with less than 30
minutes of hypoxia during the monitoring peri-
oxygenation may, in fact, cause hypoxia. Brain
od, GOS analysis at discharge demonstrated that
tissue oxygenation monitoring has the poten-
80% were either vegetative or severely disabled,
tial to detect early ischemic injury before alter-
20% had a favorable outcome, and no patients
ations in other variables occur and may improve
died acutely. In this same group, GOS at 6
months showed that 72.8% had a favorable out-come, 18.2% were vegetative or severely dis-
References
abled, and 9% died. In contrast, in patients with
1. Teasdale G, Jennett B. Assessment of coma and all refer-
more than 30 minutes of hypoxia, 48% died
impaired consciousness. Apractical scale. Lancet ences,
acutely and 52% had an unfavorable GOS at dis-
charge. In those discharged, GOS at 6 months
2. Hillier SL, Hiller JE, Metzer J. Epidemiology of first 6
showed that 55.6% had died, 22.2% were severe-
traumatic brain injury in South Australia. Brain but et al.
ly disabled, and 22.2% had a favorable outcome.
Bardt et al. concluded that even short periods
3. Jennett B. Epidemiology of head injury. J Neurol if there
of hypoxia adversely affected outcome and that
Neurosurg Psychiatry 1996;60:362–369.
functional recovery is possible in the prolonged
4. Sorensen SB, Kraus JF. Occurrence, severity and
outcomes of brain injury. J Head Trauma Rehab1991;6:1–10. Conclusions
5. Murray GD, Teasdale GM, Braakman R, et al.
The European Brain Injury Consortium survey
TBI is a major cause of morbidity and mor-
of head injuries. Acta Neurochir 1999;141:
tality worldwide. Although management has
Neurocritical Care ♦ Volume 1, 200412 __________________________________________________________________________________Mulvey et al.
6. Lang EW, Pitts LH, Damron SL, Rutledge R.
20. Povlishock JT, Christman CW. The pathobiolo-
Outcome after severe head injury: an analysis of
gy of traumatically induced axonal injury in ani-
prediction based upon comparison of neural net-
mals and humans: a review of current thoughts.
work versus logistic regression analysis. Neurol
21. Jennett B, Teasdale G. Structural Pathology. In:
7. Marshall L, Gautille T, Klauber M, et al. The out-
Jennett B, Teasdale G, eds. Management of Head
come of severe closed head injury. J Neurosurg
Injuries. Vol. 20. Philadelphia: F.A. Davis
8. Reilly PL. Brain injury: the pathophysiology of
22. Maxwell WL, Watt C, Graham DI, Gennarelli TA.
the first hours. ‘Talk and die revisited’. J Clin
Ultrastructural evidence of axonal shearing as a
result of lateral acceleration of the head in non-
9. Faden AI. Neuroprotection and traumatic brain
injury: the search continues. Arch Neurol 2001;
23. Erb DE, Povlishock JT. Axonal damage in severe
10. Clausen T, Bullock R. Medical treatment and neu-
traumatic brain injury: an experimental study in
roprotection in traumatic brain injury. Curr
cat. Acta Neuropathol 1988;76:347–358.
24. Maxwell WL, Irvine A, Graham DI, et al. Focal
11. Maas AI. Neuroprotective agents in traumatic
axonal injury: the early axonal response to
brain injury. Expert Opin Investig Drugs 2001;
stretch. J Neurocytol 1991;20:157–164.
25. Povlishock JT, Becker DP, Cheng CLY, Vaughan
12. Narayan RK, Michel ME, Ansell B, et al. Clinical
GW. Axonal change in minor head injury. J
trials in head injury. J Neurotrauma 2002; 19:503-
Neuropath Exp Neurol 1983;42:225–242.
26. Zauner A, Daugherty WP, Bullock MR, Warner
13. Morris GF, Bullock R, Marshall SB, Marmarou
DS. Brain oxygenation and energy metabolism:
A, Maas AIR, Marshall LF. Failure of the com-
Part I-biological function and pathophysiology.
petitive N-methyl-d-aspartate antagonist Selfotel
(CGS 19755) in the treatment of severe head
27. Siesjo BK. Cerebral circulation and metabolism.
injury: results of two phase III clinical trials. The
Selfotel Investigators. J Neurosurg 1999;91:737–743.
28. Zauner A, Clausen T, Alves OL, et al. Cerebral
metabolism after fluid-percussion injury and
14. Marshall LF, Maas A, Marshall S, et al. A multi-
centre trial on the efficacy of using tirilazad mesy-
late in cases of head injury. J Neurosurg 1998;89:519–525.
29. Valadka AB, Goodman JC, Gopinath SP, Uzura
15. Miller JD, Marshall LF. Are steroids useful in the
M, Robertson CS. Comparison of brain tissue
treatment of head-injured patients? Surg Neurol
oxygen tension to microdialysis-based measures
of cerebral ischemia in fatally head-injuredhumans. J Neurotrauma 1998;15:509–519.
16. Maas AI, Steyerberg EW, Murray GD, et al. Why
have recent trials of neuroprotective agents in
30. Rehncrona S, Rosen I, Siesjo BK. Brain lactic aci-
head injury failed to show convincing efficacy?
dosis and ischemic cell damage. I. Biochemistry
A pragmatic analysis and theoretical considera-
and neurophysiology. J Cereb Blood Flow Metab
tions. Neurosurgery 1999;44:1286–1298.
17. Graham DI, Adams JH, Doyle D. Ischaemic brain
31. Pulsinelli WA, Levy D, Duffy TE. Regional cere-
damage in fatal non-missile head injuries. J
bral blood flow and glucose metabolism fol-
lowing transient forebrain ischemia. Ann Neurol
18. Chesnut RM, Marshall LF, Klauber MR, et al. The
role of secondary brain injury in determining
32. Doppenberg EMR, Zauner A, Bullock MR, Ward
outcome from severe head injury. J Trauma
JD, Fatouros PP, Young HF. Correlations between
brain tissue oxygen tension, carbon dioxide, pH,
19. Chesnut RM. Secondary brain insults after head
and cerebral blood flow—a better way of moni-
injury: clinical perspectives. New Horiz 1995
toring the severely injured brain? Surg Neurol
Neurocritical Care ♦ Volume 1, 2004Monitoring Modalities in Traumatic Brain Injury ____________________________________________________13
33. Menzel M, Doppenberg E, Zauner A, Soukup J,
46. Siesjo BK, Bengtsson F. Calcium fluxes, calcium
Reinert M, Bullock R. Increased inspired oxygen
antagonists, and calcium-related pathology in
concentration as a factor in improved brain tis-
brain ischemia, and spreading depression: a uni-
sue oxygenation and tissue lactate levels after
fying hypothesis. J Cereb Blood Flow Metab 1989;
severe human head injury. J Neurosurg 1999;
47. Kazda S, Garthoff B, Krause HP, Schlossmann K.
34. Menzel M, Doppenberg EM, Zauner A, et al.
Cerebrovascular effects of the calcium antago-
Cerebral oxygenation in patients after severe
nistic dihydropyridine derivative nimodipine in
head injury: monitoring and effects of arterial
animal experiments. Arzneimittelforschung
hyperoxia on cerebral blood flow, metabolism
and intracranial pressure. J Neurosurg Anesthe-
48. Archer DP, Pappius HM. Effects of two dihy-
dropyridine calcium channel blockers on cere-
35. Voldby B, Enevoldsen EM, Jensen FT.
bral metabolism and blood flow in traumatized
Cerebrovascular reactivity in patients with rup-
rat brain. Neurochem Pathol 1986;5:117–130.
tured intracranial aneurysms. J Neurosurg
49. Teasdale G, Bailey I, Bell A, et al. A randomized
trial of nimodipine in severe head injury: HIT I.
36. Ritter AM, Robertson CS. Cerebral metabolism.
British/Finnish Co-operative Head Injury Trial
Neurosurg Clin N Am 1994;5:633–645.
Group. J Neurotrauma 1992;9:S545–S550.
37. Sutton RL, Hovda DA, Adelson PD, Benzel EC,
50. Harders A, Kakarieka A, Braakman R. Traumatic
Becker DP. Metabolic changes following cortical
subarachnoid hemorrhage and its treatment with
contusion: relationship to edema and morpho-
nimodipine. German tSAH study group. J Neuro-
logical changes. Acta Neurochir (suppl) 1994;
51. Choi DW. Ionic dependance of glutamate neu-
38. Mulvey JM, Renshaw GMC. Brainstem neuronal
rotoxicity. J Neurosci 1987;7:369–379.
oxidative hypometabolism in response to hypox-
52. White BC, Sullivan JM, DeGracia DJ, et al. Brain
ic pre-conditioning in the epaulette shark
ischemia and reperfusion: molecular mecha-
(Hemiscyllium ocellatum). Neurosci Lett 2000
nisms of neuronal injury. J Neurol Sci 2000;
39. Bouma GJ, Muizelaar JP, Choi SC, Newlon PG,
53. McCulloch J, Ozyurt E, Park CK, Nehls DG,
Young HF. Cerebral circulation and metabolism
Teasdale GM, Graham DI. Glutamate receptor
in severe traumatic brain injury: the elusive role
antagonists in experimental focal cerebral
of ischemia. J Neurosurg 1991;75:685–693.
ischaemia. Acta Neurochir Suppl (Wien) 1993;
40. Xiong Y, Peterson PL, Lee CP. Alterations in cere-
bral energy metabolism induced by traumatic
54. Park CK, Nehls DG, Graham DI, Teasdale GM,
brain injury. Neurol Res 2001;23:129–138.
McCulloch J. Focal cerebral ischaemia in the cat:
41. Sims NR, Anderson MF. Mitochondrial contri-
treatment with the glutamate antagonist MK-801
butions to tissue damage in stroke. Neurochem
after induction of ischaemia. J Cereb Blood Flow
42. Cromptom M. The mitochondrial permeability
55. Panter SS, Faden AI. Pretreatment with NMDA
transition pore and its role in cell death. Biochem
antagonists limits release of excitatory amino
acids following traumatic brain injury. Neurosci
43. Blomgren K, Zhu C, Hallin U, Hagberg H.
Mitochondria and ischemic reperfusion damage
56. Tsuchida E, Rice M, Bullock R. The neuropro-
in the adult and in the developing brain. Biochem
tective effect of the forebrain-selective NMDA
antagonist CP101,606 upon focal ischemic brain
44. Neumar RW. Molecular mechanisms of ischemic
damage caused by acute subdural hematoma in
the rat. J Neurotrauma 1997;14:409–417.
57. Siesjo BK. Basic mechanisms of traumatic brain
45. Goldberg MP, Choi DW. Combined oxygen and
damage. Ann Emerg Med 1993;22:959–969.
glucose deprivation in cortical cell culture: cal-
58. Smith SL, Andrus PK, Gleason DD, Hall ED.
Infant rat model of the shaken baby syndrome:
mechanisms of neuronal injury. J Neurosci 1993;
preliminary characterization and evidence for
the role of free radicals in cortical hemorrhaging
Neurocritical Care ♦ Volume 1, 200414 __________________________________________________________________________________Mulvey et al.
71. Lang EW, Czosnyka M, Mehdorn HM. Tissue
oxygen reactivity and cerebral autoregulation
59. Clark WM, Hazel JS, Coull BM. Lazaroids. CNS
after severe traumatic brain injury. Crit Care Med
72. Gupta AK, Hutchinson P, Al-Rawi P, et al.
60. Wienkers LC, Steenwyk RC, Mizsak SA, Pearson
Measuring brain tissue oxygenation compared
PG. In vitro metabolism of tirilazad mesylate in
with jugular venous oxygen saturation for mon-
itoring cerebral oxygenation after traumatic
cytochrome P4502C11 and delta 4-5 alpha-reduc-
brain injury. Anesthesia and Analgesia 1999;
tase. Drug Metab Dispos 1995;23:383–392.
61. Smith SL, Andrus PK, Zhang JR, Hall ED. Direct
73. Zauner A, Bullock R, Di X, Young HF. Brain oxy-
measurement of hydroxyl radicals, lipid perox-
gen, CO2, pH and temperature monitoring: eval-
idation, and blood-brain barrier disruption fol-
uation in the feline brain. Neurosurgery 1995
lowing unilateral cortical impact head injury in
the rat. J Neurotrauma 1994;11:393–404.
74. Zauner A, Doppenberg EMR, Woodward JJ.
62. Hall ED, Andrus PK, Yonkers PA. Brain hydrox-
Multiparametric continuous monitoring of brain
yl radical generation in acute experimental head
metabolism and substrate delivery in neurosur-
injury. J Neurochem 1993;60:588–594.
gical patients. Neurol Res 1997;19:265–273.
63. Sanada T, Nakamura T, Nishimura MC, Isayama
75. Meixensberger J, Baunach S, Amschler J, Dings
K, Pitts LH. Effect of U74006F on neurologic func-
J, Roosen K. Influence of body position on tis-
tion and brain edema after fluid percussion injury
in rats. J Neurotrauma 1993;10:65–71.
intracranial pressure in patients with acute brain
64. Grumme T, Baethmann A, Kolodziejczyk D, et
injury. Neurol Res 1997;19:249–253.
al. Treatment of patients with severe head injury
76. Maas AIR, Fleckenstein W, de Jong DA.
by triamcinolone: a prospective, controlled mul-
Monitoring cerebral oxygenation: experimental
ticenter clinical trial of 396 cases. Res Exp Med
studies and preliminary clinical results of con-
tinuous monitoring of cerebrospinal fluid and
65. Young B, Runge JW, Harrington T, et al. Effects
brain tissue oxygen tension. Acta Neurochir
of pegorgotein on neurologic outcome of patients
with severe head injury. A multicenter, random-
77. Kiening KL, Unterberg AW, Bardt TF, Schneider
ized controlled trial. JAMA 1996;276:538–543.
GH, Lanksch WR. Monitoring of cerebral oxy-
66. Kiening KL, Hartl R, Unterberg AW, Schneider
genation in patients with severe head injuries:
itoring in comatose patients: implications for
uration. J Neurosurg 1996;85:751–757.
therapy. J Neurol Res 1997;19:233–240.
78. Dings J, Meixensberger J, Amschler J, Hamelbeck
67. Gopinath SP, Valadka AB, Uzura M, Robertson
B, Roosen K. Brain tissue pO2 in relation to cere-
CS. Comparison of jugular venous oxygen sat-
bral perfusion pressure, TCD-findings and TCD-
2 reactivity after severe head injury. Acta
bral ischemia after head injury. Crit Care Med
79. Dings J, Jager A, Meixensberger J, Roosen K. Brain
68. van den Brink WA, van Santbrink H, Steyerberg
tissue pO2 after severe head injury. Neurol Res
WW, et al. Brain oxygen tension in severe head
injury. Neurosurgery 2000;46:868–878.
80. Valadka AB, Gopinath SP, Contant CF, Uzura M,
69. van Santbrink H, Maas A, Avezaat C. Continuous
Robertson CS. Relationship of brain tissue pO2
monitoring of partial pressure of brain tissue
to outcome after severe head injury. Crit Care
oxygen in patients with severe head injury.
81. Bardt TF, Unterberg AW, Hartl R, Kiening KL,
70. Dings J, Meixensberger J, Jager A, Roosen K.
Scheider GH, Lanksch WR. Monitoring of brain
Clinical experience with 118 brain tissue oxygen
tissue pO2 in traumatic brain injury: effect of
partial pressure catheter probes. Neurosurgery
cerebral hypoxia on outcome. Acta Neurochir
Neurocritical Care ♦ Volume 1, 2004Monitoring Modalities in Traumatic Brain Injury ____________________________________________________15
82. Baumgartl H, Lubbers DW. Microcoaxial needle
gen during CO2 and O2 reactivity tests in severe-
sensors for polarographic measurements of local
ly head-injured patients. Acta Neurochir (Wien)
O2 in the cellular range of living tissue. In:
Gnaiger E, Forstner H, eds. Polarographic
92. Robertson CS, Narayan RK, Contant CF, et al.
Oxygen Sensors. New York: Springer Verlag,
Clinical experience with a continuous monitor
of intracranial compliance. J Neurosurg 1989;71:
83. Lubbers DW, Baumgartl H. Heterogeneities and
profiles of oxygen pressure in brain and kidney
93. Cruz J, Miner ME, Allen SJ, Alves WM, T.A. G.
as examples of pO2 distribution in the living tis-
Continuous monitoring of cerebral oxygenation
sue. Kidney International 1997;51:372–380.
in acute brain injury: assessment of cerebral
84. Sarrafzadeh AS, Unterberg AW, Keining KL,
hemodynamic reserve. Neurosurgery 1991;29:
Bardt T, Schneider GH, Lanksch WR. Monitoring
of cerebral oxygenation in traumatic brain
94. Cruz J, Raps EC, Hoffstad OJ, Jaggi JL, Gennarelli
injured patients. In: Bauer BL, Kuhn TJ, eds.
TA. Cerebral oxygenation monitoring. Crit Care
Severe Head Injuries. Berlin: Springer Verlag,
95. Dings J, Meixensberger J, Roosen K. Brain tissue
85. Hartl R, Bardt T, Keining KL, Sarrafzadeh AS,
pO2 monitoring: catheter stability and compli-
Schneider GH, Unterberg AW. Mannitol decreas-
cations. Neurol Res 1997;19:241–245.
es ICP but does not improve brain tissue pO2 in
96. Meixensberger J, Jager A, Dings J, Baunach S,
severely head-injured patients with intracranial
Roosen K. Quality and therapeutic advances in
hypertension. Acta Neurochir 1997;70(suppl):
multimodality neuromonitoring following head
injury. In: Bauer BL, Kuhn TJ, eds. Severe Head
86. Stocchetti N, Chieregato A, De Marchi M, Croci
Injuries. Berlin: Springer Verlag, 1997:109–120.
M, Benti R, Grimoldi N. High cerebral perfusion
97. van den Brink WA, Haitsma IK, Avezaat CJ,
pressure improves low values of local brain tis-
sue O2 tension (ptiO2) in focal lesions. Acta
Neurochir 1998; 71(suppl):162–165.
histopathological study in the rat. J Neurotrauma
87. Strege RJ, Lang EW, Stark AM, et al. Cerebral
edema leading to decompressive craniectomy:
98. Kaups KL, Parks SN, Morris CL. Intracranial
An assessment of the preceding clinical and neu-
pressure monitor placement by midlevel practi-
romonitoring trends. Neurol Res 2003:accepted.
tioners. J Trauma 1998;45:884–886.
88. Czosnyka M, Smielewski P, Kirkpatrick P, Menon
99. Coplin WM, O’Keefe GE, Grady MS, et al.
DK, Pickard JD. Monitoring of cerebral autoreg-
Thrombotic, infectious, and procedural compli-
cations of the jugular bulb catheter in the inten-
sive care unit. Neurosurg 1997;41:101–109.
89. Bouma G, Muizelaar J. Cerebral blood flow, cere-
100.Lang EW, Chesnut RM. Intracranial pressure.
bral blood volume, and cerebrovascular reac-
Monitoring and management. Neurosurg Clin
tivity after severe head injury. J Neurotrauma
90. Lang E, Mehdorn H, Dorsch N, Czosnyka M.
101.Narayan RK, Kishore PR, Becker DP, et al.
Intracranial pressure: to monitor or not to mon-
autoregulation: a validation study. J Neurol
itor? Areview of our experience with severe head
Neuros Psychiatry 2002;72:583–586.
injury. J Neurosurg 1992;56:650–659.
91. Fandino J, Stocker R, Prokop S, Imhof HG.
102.Zink BJ. Traumatic brain injury outcome: con-
Correlation between jugular bulb oxygen satu-
ration and partial pressure of brain tissue oxy-
Neurocritical Care ♦ Volume 1, 2004
e suitable for long term oxygenation monitoring
was placed in an ischemic but salvageable part of the
below 10 mmHg for longer than 10 min was always associ
could be performed for twice the duration of SjvO
Neither modality detected all ischemic episodes
Both modalities would compliment each other
Similar duration of monitoring between ptiO
equent episodes of hypoxia associated with a poor
esholds seen in 50% cases on day 1 posttrauma
>20 mmHg, mannitol infusion significantly changed
No significant change was detected with ptiO
18 __________________________________________________________________________________Mulvey et al.
Traumatic brain injurySubarachnoid hemorrhageStrokeTumor
Neurocritical Care ♦ Volume 1, 2004
a cura del dr. Alfonso Siani - Istituto di Scienze dell’Alimentazione, CNR Il Progetto IDEFICS Imparare a vivere in modo salutare. Sviluppo di una strategia d’intervento europea. Il progetto IDEFICS (Identificazione e pre- sanitarie, quindi, dovranno confrontarsi saranno raccolte attraverso questionari venzione degli effetti indotti dal a dieta e con l’aumento del e patologie lega
MEMORANDUM Minutes of the meeting of 21 November, 2005 M. Benotti D. Paquette S. Robbins K. Roberts W. Spitz S. Terracciano The minutes of the last meeting were not available. The USGS Albany Office is planning a USGD/DEC “Summit” in Troy. Although the exact date has not been set, representatives from the LI offices of the DEC and the USGD might want to attend since funding priori

 Neurocritical CareCopyright 2004 Humana Press Inc. All rights of any nature whatsoever are reserved.
Neurocritical CareCopyright 2004 Humana Press Inc. All rights of any nature whatsoever are reserved.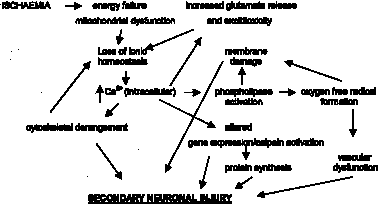 Monitoring Modalities in Traumatic Brain Injury _____________________________________________________3
Fig. 1. A schematic diagram representing the molecular events implicated in secondary neuronal injury caused
Monitoring Modalities in Traumatic Brain Injury _____________________________________________________3
Fig. 1. A schematic diagram representing the molecular events implicated in secondary neuronal injury caused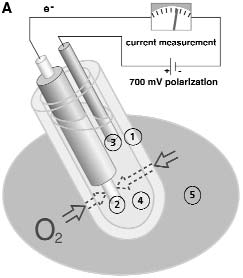
 6 ___________________________________________________________________________________Mulvey et al.
Fig. 2. (A) A schematic diagram of the Licox polarographic oxygenation probe.The numbered components of
6 ___________________________________________________________________________________Mulvey et al.
Fig. 2. (A) A schematic diagram of the Licox polarographic oxygenation probe.The numbered components of Monitoring Modalities in Traumatic Brain Injury _____________________________________________________7
associated with higher ptiO2. This suggests thatthe critical threshold of CPP is 60 mmHg andthat ptiO2 is more sensitive than SjvO2 to changesin CPP. In contrast, Hartl et al. (85) report thattreatment of ICP with mannitol was not asso-ciated with improvements in ptiO2. However,it should be noted that in this study, ICP wastreated before it was severely raised (23 ± 1mmHg), and initial CPP before treatment was68 ± 2 mmHg.
Monitoring Modalities in Traumatic Brain Injury _____________________________________________________7
associated with higher ptiO2. This suggests thatthe critical threshold of CPP is 60 mmHg andthat ptiO2 is more sensitive than SjvO2 to changesin CPP. In contrast, Hartl et al. (85) report thattreatment of ICP with mannitol was not asso-ciated with improvements in ptiO2. However,it should be noted that in this study, ICP wastreated before it was severely raised (23 ± 1mmHg), and initial CPP before treatment was68 ± 2 mmHg.