Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Influenza
Infectious Disease Epidemiology Section Office of Public Health, Louisiana Dept of Health & Hospitals 800-256-2748 (24 hr number) – (504) 568-5005 www.oph.dhh.state.la.us Malaria is caused by an intracellular protozoa of the genus Plasmodium. The 4 species that cause human malaria are Epidemiology
Malaria is transmitted by the bite of an infected female Anopheles mosquito or through direct inoculation of infected red blood cells, i.e., congenital malaria, transfusion malaria, and malaria from contaminated needles. The life cycle of malaria is complex and certain aspects differ according to the Plasmodium species in- volved. • The infective stages of plasmodia called sporozoites are injected during feeding from the salivary
glands of the infected mosquito into the blood stream through subcutaneous capillaries. • Human Pre-erythrocytic Phase (Before the red blood cell): Sporozoites enter the liver cells, where they
multiply asexually. There the nucleus undergoes repeated division, forming thousands of uninucleate merozoites. There is no inflammatory reaction in the surrounding liver tissue. After 6 to 16 days from the time of infection, the hepatic cell containing the tissue schizonts ruptures and the merozoites enter the circulation. • Human Exo-erythrocytic Phase (Outside the red blood cell):
P. falciparum and P. malariae schizonts all rupture at about the same time, and none persist in the
liver. The only “exo” erythrocytic phase for these 2 species occur before the invasion of RBC. There is NO continuous cycle in the liver.
P. vivax and P. ovale have a continuous exoerythrocytic cycle: Some parasites that remain dormant in
the liver (hypnozoites) for weeks, months, or even years before developing and resulting in relapses of erythrocytic infection. All 4 species of malaria can cause chronic infections with fever occurring more than once. • Human Erythrocytic Phase (in the red blood cell).
Merozoites released from tissue schizonts invade erythrocytes. • RBC Asexual Stages.
The youngest stages in the RBC are small, rounded trophozoites, known as ring forms. During develop-ment, they use the hemoglobin, leaving as the product of digestion an iron-containing pigment, hematin or hemozoin, which can be seen in the cytoplasm of the parasite as dark granules. They grow in the red blood cell and when nuclear division occurs the parasite is called a schizont. This asexual multiplication is the erythrocytic schizogony. The infected erythrocytes rupture, liberating merozoites, which must in-vade new red cells. The erythrocytic cycle of schizogony is repeated over and over again. The periodicity of schizogony differs according to species. • RBC Sexual Stages:
Louisiana Office of Public Health – Infectious Disease Epidemiology Section- Infectious Disease Control Manual
From 3 to 15 days after the onset of symptoms, subpopulations of merozoites differentiate into sexual forms, gametocytes, i.e., female macrogametocytes and male microgametocytes. The duration of game-tocytogony is assumed to be 4 days in P. vivax infections and 10 or more days in P.falciparum infections. • Vector phase
When feeding on an infected human, the female Anopheles ingests gametocytes, which develop in the gut of the mosquito. The nucleus of the male gametocyte divides and forms long, thread-like flagellum which break free and produce microgametes. These fertilize the female macrogamete to produce a zygote. The zygote gets wedged in the outer surface of the stomach and rounds up into a oocyst. An infected Anopheles may have 10 to several 100 oocysts. The oocyst enlarges and the nucleus divides then forms finger-like processes, which become fusiform sporozoites. The oocyst ruptures, liberating thousands of motile sporozoites which migrate to the salivary glands. The female mosquito is now infective. Sporogony varies from 8 to 35 days, depending on external temperature and on the malaria species. Epidemiologic classification of cases
Autochthonous malaria is contracted locally. Malaria is indigenous when naturally present in an area or
Imported malaria is acquired outside a given area, Secondary cases are those derived from imported cases and are referred to as introduced malaria, Malaria acquired by blood transfusions, sharing of needles, intentional inoculation, or accidental labora-
tory infections is known as induced malaria,
Cases with insufficient information to classify are cryptic.
Imported Malaria: Increase in international air travel has resulted in importation of malaria and other dis-eases to nonendemic areas. Regions where malaria has been eradicated are at continuing risk of imported cases. Patients often arrive during the incubation period and may not become ill until reaching home. De-lays in diagnosis, misdiagnosis, and inappropriate treatment may occur, resulting in excessive morbidity and mortality. Physicians and public health officials must remain aware of the possibility of imported ma-larial infections The incubation period varies according to species: is usually 12 to 18 days for P.vivax or P.ovale, slightly shorter for P.falciparum.Clinical Description
Clinical symptoms and signs of malaria are associated with the release of merozoites, malarial pigment, and debris into the circulation following rupture of infected erythrocytes. Semi-immune patients are less likely to develop severe manifestations and complications when they become infected. Some patients have vague prodromal symptoms before parasites can be detected in the blood. These manifestations, i.e., malaise, myalgia, headache, anorexia, and slight fever, may persist for 2 or 3 days before an acute paroxysm begins. In the initial phase of illness, the fever can be erratic or continuous. If the infection continues for 3 to 4 days, a synchronous cycle may develop with afternoon temperature ele- vations approximately every 48 hours, the classic benign tertian periodicity. The fever can be as high as 40°C (104°F) and the patient often feels much worse with falciparum malaria.
The typical paroxysm has an abrupt onset with a feeling of coldness and a chill. The teeth chatter, and the patient covers himself. Within 30 to 60 minutes, the patient feels hot and has profuse sweating, usually a headache, malaise, and myalgia, along with a varying degree of other symptoms, e.g., nausea, vomiting, flushed face, dry and burning skin, and convulsions. Temperatures of 40°C to 41°C (104°F to 106°F) are
usual in primary falciparum infections, whereas with the other 3 species of plasmodia fever peaks are usually lower 39°C to 40 °C). The hot stage lasts from 2 to 6 hours. The sweating stage, in which the pa-
tient's temperature falls rapidly, lasts 2 to 3 hours. The entire paroxysm, which often begins in the early afternoon, averages 9 to 10 hours. Between paroxysms, the patient may feel well.
Louisiana Office of Public Health – Infectious Disease Epidemiology Section- Infectious Disease Control Manual
P.falciparum causes the most severe form of malarial infection. It may kill up to 25% of nonimmune adults within 2 weeks of a primary attack unless appropriate treatment is given. All 4 species of malaria can cause chronic infections with fever occurring more than once. Recru-descences occur for P. falciparum and P. malariae which have no persistent exoerythrocytic phase, so recurrent parasitemia is due to proliferation of persistent erythrocytic forms and is known as recrudes-cence. For P.vivax and P.ovale, relapses are due to persistence of parasitic forms in the liver. Congenital malaria is rare, and its occurrence is associated with low immunity in the mother. Therefore, most cases of congenital malaria appear in areas where the prevalence of malaria is low or involve non-immune mothers. Passive transfer of antibody across the placenta helps to protect neonates for the first 6 to 12 months of life. Malaria is an important cause of abortions, stillbirths, and low birth weight, as well as neonatal and infant mortality. Complications include: • Splenic Rupture
• Cerebral Malaria is a frequent cause of mortality, especially in children and nonimmune adults. It
usually develops slowly over several days but may occur early in the illness. A severe headache appears. The patient becomes increasingly drowsy and confused and, if not treated rapidly, becomes delirious and then comatose. Hallucinations occur, and the patient may appear drunk. In-patients with cerebral malaria, very high fever, i.e., 41° to 42°C (106° to 108°F), can occur. The skin is often flushed and dry, as in heat
stroke. Hyperpyrexia requires immediate treatment to reduce the fever. • Hemolytic Anemia can be severe in patients with high parasitemias ( 5%) and in non-immune individu-
als. Sudden intravascular hemolysis can lead to acute renal failure. • Renal Failure: Mild proteinuria, azotemia, and oliguria occur frequently in heavy P. falciparum infec-
tions. Acute renal failure often complicates severe falciparum infections with high parasitemia, and marked hemolysis in an acute tubular necrosis results from renal anoxia, a reduced renal blood flow, and deposition of hemoglobin in the renal tubules. Anuria is a poor prognostic sign, requiring peritoneal di-alysis or hemodialysis. • Blackwater Fever: Severe hemolysis, hemoglobinuria, and renal failure make up the clinical triad of
"blackwater fever." Treatment
The choice of malaria chemotherapy is based on the infecting species, possible drug resistance, and the severity of disease. Severe malaria is defined as a parasitemia greater than 5%, signs of central nervous system or other end-organ involvement, shock, acidosis, and/or hypoglycemia. Patients with severe ma- laria require intensive care and parenteral treatment until the parasite density falls below 1% and they are able to tolerate oral therapy. Exchange transfusion may be warranted when parasitemia exceeds 10%. Treatment of Chloroquine-Susceptible Plasmodium vivax, Plasmodium ovale, Plasmodium malariae, and Plasmodium falciparum Chloroquine-susceptible infections may be treated orally using a total dose of 25 mg chloroquine base/kg given over 3 days. Patients unable to take oral medications may be treated initially with parenteral chloroquine, and then switched to oral chloroquine when they are able to take oral medications. Even for persons with central nervous system involvement, there are no advantages of quinine (or other antimalar- ial agents) over chloroquine for infections due to chloroquine-susceptible parasites. Halofantrine is con- traindicated in pregnant or lactating women. Because of its arrhythmogenic potential,] intravenous chloro- quine must be given as a carefully controlled infusion to avoid a large bolus in the heart. Pruritus is an important side effect of chloroquine (and halofantrine) and is particularly common in sub-Saharan Africa, although its pathogenesis is unclear.
Louisiana Office of Public Health – Infectious Disease Epidemiology Section- Infectious Disease Control Manual
Treatment of Chloroquine-Resistant Plasmodium falciparum Persons able to take oral medications may be treated with quinine, mefloquine, halofantrine,] or pyrimethamine sulfadoxine, assuming that they did not receive the same drug for chemoprophylaxis. Be- cause most parasites resistant to mefloquine are also resistant to halofantrine, halofantrine should not be used to treat persons who acquire P. falciparum infection while receiving mefloquine chemoprophylaxis. Halofantrine can result in prolongation of the QT interval and ventricular arrhythmias in susceptible per- sons receiving higher than recommended doses as well as in those with recent or concurrent mefloquine therapy, QT prolongation, or thiamine deficiency. Because fatalities have occurred with halofantrine, al- ternative drugs are preferred when possible. Halofantrine is contraindicated in pregnant or lactating women. Because resistance to pyrimethamine sulfadoxine is common in areas with chloroquine resis- tance, persons given pyrimethamine sulfadoxine should be watched carefully to ensure that the drug is effective. Although quinine may often produce side effects, it is effective in vivo against all strains of P. falciparum studied thus far. Because quinidine is two- to threefold more active than quinine, because its serum and plasma levels can be measured in most American hospitals, and because parenteral quinine is no longer available in the United States, quinidine is preferable to quinine for parenteral use in the United States. Artemisinin derivatives such as artemether are effective in children with P. falciparum infection; they may clear parasitemia and coma more rapidly than does quinine. A controlled study in Thailand has suggested that intravenous artesunate followed by mefloquine is more effective than either artesunate or mefloquine alone and may prevent the late recrudescences typically observed with artesunate alone. Addi- tional controlled studies suggest that artemisinin suppositories may clear P. falciparum parasitemia as rapidly as intravenous artesunate,] and that artemether is as effective as quinine for severe and cerebral malaria.] Because artemisinin treatment is frequently associated with late recrudescences,] additional drugs such as mefloquine, tetracycline, or pyrimethamine sulfadoxine are often given after the initial treatment with artemisinin to prevent recrudescence 3 to 4 weeks later. Anecdotal reports of embryo toxicity in rats and mice and pathologic evidence of neurotoxicity in dogs suggest that artemisinin derivatives should not be given to pregnant women and should be used with caution until these issues have been resolved. Note that comparative studies of artemether and quinine have not found an increase in neurotoxicity with arte- mether.] As with quinine, there is no evidence of high-level resistance to artemisinin or its derivatives. Treatment of Chloroquine-Resistant Plasmodium vivax Thus far, all persons with chloroquine-resistant P. vivax infection have responded to treatment with oral mefloquine or halofantrine. Laboratory Tests Blood Smears Definitive diagnosis of malaria depends on microscopic demonstration of parasites in the peripheral blood film. For detection of organisms, the thick blood film is superior because it concentrates the red blood cells by a factor of 20 to 40 times. A thick film will yield 3 to 4 times as many positive findings as a thin smear and will reveal plasmodia in virtually all active clinical cases. Identification of species in the thick film is difficult because the red cells are lysed in the staining procedure and there is alteration of the morphologic features of the parasites. For positive identification of species, a thin blood film is often necessary. Thick and thin films can be made on the same slide. In doubtful cases, it may be necessary to repeat the thick blood smears every 4 to 6 hours until the diagnosis is made. Timing: Symptoms may precede detectable parasitemia by 1 to 2 days. Timing of blood smears is less important than obtaining several smears daily in order to make the diagnosis. Quantitation of parasitemia is useful in following the response to therapy. Blood smears should be stained with Giemsa stain. Leishman's stain and Wright's stain can also be used but are not as good. Rapid staining may be done with Field's stain, although this stain is less permanent.
Louisiana Office of Public Health – Infectious Disease Epidemiology Section- Infectious Disease Control Manual
The most important initial distinction to make is whether P. falciparum is present, because this parasite is frequently life threatening. Species identification may require expert opinion; many physicians are not sufficiently experienced in morphologic differentiation. P.falciparum is suggested by criteria such as small ring size, banana-shaped gametocytes, multiple parasites in a single erythrocyte, parasitemia greater than 2% of the red blood cells, and predominance of rings with few trophozoites and no schizonts. The presence of granular brownish pigment in monocytes or leukocytes should alert physicians to malaria even in the absence of demonstrated parasitemia. Parasites may also be demonstrated in a bone marrow specimen, but this is rarely required. Antibodies, demonstrable by IFA will appear after the first week of infection but may persist for years and is of limited use in diagnosis since it cannot differentiate between current and past infection. They are not useful for the diagnosis of acute illness. Surveillance
Malaria a condition reportable within one business day of the diagnosis. Case Definition
Clinical description Signs and symptoms are variable; however, most patients experience fever. In addition to fever, common symptoms include headache, back pain, chills, sweats, myalgia, nausea, vomiting, rarely diarrhea and cough. Untreated Plasmodium falciparum infection can lead to coma, renal failure, pulmonary edema, and death. The diagnosis of malaria should be considered for any person who has these symptoms and who has traveled to an area in which malaria is endemic. Asymptomatic parasitemia can occur among persons who have been long-term residents of areas in which malaria is endemic. Laboratory criteria for diagnosis: Demonstration of malaria parasites in blood films Case classification Confirmed: an episode of microscopically confirmed malaria parasitemia in any person (symptomatic or asymptomatic) diagnosed in the United States, regardless of whether the person experienced previous epi- sodes of malaria while outside the country. Comment A subsequent attack experienced by the same person but caused by a different Plasmodium species is counted as an additional case. A subsequent attack experienced by the same person and caused by the same species in the United States may indicate a relapsing infection or treatment failure caused by drug resistance. Cases also are classified according to the following World Health Organization categories: Indigenous: malaria acquired by mosquito transmission in an area where malaria is a regular occurrence Introduced: malaria acquired by mosquito transmission from an imported case in an area where malaria is not a regular occurrence Imported: malaria acquired outside a specific area (e.g., the United States and its territories) Induced: malaria acquired through artificial means (e.g., blood transfusion, common syringes, or malario- therapy)
Louisiana Office of Public Health – Infectious Disease Epidemiology Section- Infectious Disease Control Manual
Relapsing: renewed manifestation (i.e., of clinical symptoms and/or parasitemia) of malarial infection that is separated from previous manifestations of the same infection by an interval greater than any interval resulting from the normal periodicity of the paroxysms Cryptic: an isolated case of malaria that cannot be epidemiologically linked to additional cases Investigation The purpose of investigation is to confirm suspected cases and identify species, to document recent travel history, to identify other travellers who may have been exposed and classify the case according to epidemiologic origin. Upon receipt of a report of a malaria case, contact the physician and/or hospital to confirm the diagnosis. Verify the species of malaria. Investigate the source of exposure, i.e. recent travel history, blood transfusion, foreign residence,, etc., and document history of malaria chemoprophylaxis. Identify any other individuals at risk, (i.e., fellow travelers or blood bank, etc.) If a history of needle sharing is obtained from the patient, investigate and refer all persons who shared the equipment for treatment. If the malaria is a transfusion-induced case, all donors must be located and their blood examined for malarial parasites and for antimalarial antibodies. Those individuals that are parasite-positive donors should be referred for treatment. Hospital precaution and isolation: Standard precautions Malaria Prevention For Travelers
P.falciparum malaria is a life threatening disease for all persons infected but especially for those who have been recently infected and have no immunity to it. Every year, some 10,000 US travelers are in- fected during their travel and become sick when returning home. About one hundred die although preven- tion was possible. Globally, about 2 billion people are at risk of malaria, 270 million are infected and 1 million die from malaria each year. 1-Inform the traveler about the degree of risk of malaria infection: To advise travelers on malaria risk and prophylaxis it is necessary to know the distribution of malaria worldwide (see map). There are 4 zones of malaria risk. Prophylaxis has to be adapted to the area: • Malaria free areas: Western and Eastern Europe, USA, Canada, former USSR, northern Asia (Korea,
Japan), Australia, North Pacific Islands, most South Pacific Islands (from New Caledonia to Easter Is-lands). • Low risk malaria, Plasmodium vivax and P. malariae, no chloroquine resistant Plasmodium falciparum
(CRPF) or no P.falciparum: SW Saudi Arabia, Egypt and most of the Middle East, Iran, China, Peru and Bolivia. Malaria transmission is seasonal and low. There is no risk in urban and in high altitude areas. • Low risk malaria but some CRPF: Southern part of the Arabian peninsula, Afghanistan, Pakistan, most
of India and Philippines. • High risk malaria and CRPF: Intertropical Africa, Amazon basin, the Indochinese peninsula, Indonesia,
New Guinea, Solomon Islands and Vanuatu.
Louisiana Office of Public Health – Infectious Disease Epidemiology Section- Infectious Disease Control Manual
Malaria Endemic Areas (see page one for explanation of numbers)
Low risk, no chloroquine resistant Plasmodium falciparum
Low risk, some chloroquine resistant Plasmodium falciparum
High risk, chloroquine resistant Plasmodium falciparum
2-Recommend precautions against mosquito bites. This advice is as important as the prophylactic treat-ment. • Avoid going out at night or wear long sleeve shirts and long trousers and avoid dark colors which at-
tract mosquitoes. • Apply insect repellent (with NN diethyl-m-toluamide -DEET- or dimethyl phtalate). Follow the instruc-
tions on the bottle. Do not exceed the dose particularly in children. • Spend nights in well maintained buildings with screened doors and windows. If the building is not in-
sect-proof sleep under a mosquito net. Make sure that the net is not torn and that no mosquitoes are trapped inside. Tuck the net under the mattress. Insecticide sprays, electric insecticide dispenser with py-rethroid tablets and pyrethroid mosquito coil are useful but do not replace a good mosquito net. 3-Prophylactic treatment: The decision is based on the risk of malaria in the country AND the area traveled. Travelers who spend a short stop over in a major city with sightseeing in the city are at very low risk and often prophylaxis is not recommended. Travelers who take trips to rural areas, particularly if they spend some nights in rural areas should take some prophylaxis. Prophylactic treatment should start a week before departure (loading dose and to check for any immediate serious side effects). Patients should understand that prophylactic treatment DOES NOT prevent infec-tion, it only suppresses disease. It must be taken for the whole time the traveler is in the malarious area and continued for no less than 4 weeks (some recommend up to 8 weeks) after return to a malaria free area. They must seek prompt medical attention if they become ill.
Louisiana Office of Public Health – Infectious Disease Epidemiology Section- Infectious Disease Control Manual
Prophylaxis recommendation according to malaria risk (see enclosed map)
Malaria risk Areas traveled Prophylaxis
Chloroquine or Chloroquine/Proguanil (*)
4 High, CRPF
Mefloquine or Chloroquine/Proguanil or Doxycycline
(*) If proguanil is not available, use mefloquine instead of chloroquine/proguanil 4-Stand-by treatment for travelers taking long trips (safaris, hiking trips) to rural areas during which prompt medical help will not be available. The treatment should be completed and prophylaxis resumed 7 days after the first dose of stand-by treatment. The traveler must understand that stand-by treatment is only a temporary measure and that medical advice should be sought after self-treatment. Make sure that the traveler understands not to use the same dose in children. 5-Advise the traveler to seek immediate treatment in case of fever.
The traveler must understand that malaria can kill if treatment is delayed (this is probably the most impor-tant message that the traveler should leave with). Any symptoms, even mild symptoms appearing one week or more after entry in a malaria endemic area and up to 2 months after return could be due to ma-laria: Headache, muscular ache (particularly back ache), sensation of fatigue or weakness, fever, nausea, vomiting or loose stools and cough could be the early signs of malaria. Prompt medical advice should be sought. Beware of physicians who rule out malaria without taking a blood smear (finger stick and applica-tion of a drop of blood on the slide). Be aware that at the early stages of malaria, a blood smear may be negative, and that if symptoms persist a repeat blood smear is necessary. The patient should always state that he/she has traveled through a malarious area when seeking medical attention. Most malaria deaths among travelers have occurred because the traveler delayed seeking medical atten-tion, or did not mention the history of travel in a malarious area, or the physician ignored that important clue, or the physician was falsely reassured by an early negative blood smear or the physician was misled by a false negative blood smear (early low density parasitemia are often missed if the lab does not per-form a thick smear examination). When the diagnosis of malaria becomes obvious it may be too late for antimalarials to prevent the fatal outcome.
Louisiana Office of Public Health – Infectious Disease Epidemiology Section- Infectious Disease Control Manual
Malaria prophylaxis and stand-by treatment
600mg 3 times/day = 1800 mg/day for 7 days =10 mg/kg *3/day
500mg 3 times at 6 hours interval 8mg/kg *3 /12hrs
Chloroquine dose recommendations are expressed in mg of base chloroquine. Some manufacturers list both base and total chloroquine phosphate on their label. A 500mg tablet of chloroquine phosphate is the equivalent of 300 mg of chloroquine base. Make sure the base dosage is well understood. In some foreign countries (Francophone Africa specially), the recommendations are for twice this dosage. This is accept-able and poses no risk to the traveler. DO NOT leave chloroquine within reach of small children, although the drug has been proven by 40 years of experience to be extremely safe at the antimalarial doses, it is very toxic (cardiac toxicity) if an overdose is taken. This drug has been used since the late 1940s and was the main drug for prophylaxis for several decades. Recently, its prophylactic effectiveness among travelers to East Africa was found to be only 10%. Minor adverse reactions, including nausea, vomiting, abdominal pain, anorexia, dizziness, and headache, occur infrequently. Seizures and mania have been reported with chloroquine prophylaxis. Pruritus is a com-mon complication of chloroquine use in African blacks. The drug can be used during pregnancy. Proguanil has to be taken daily, weekly doses are NOT effective because of the short half life of the drug. Sulfadoxine-pyrimethamine (Fansidar) should not be used in infants less than 2 months (immature glu-curonide forming enzyme system), patients with history of allergy to sulfonamides, G6PD deficient pa-tients. Mefloquine is not recommended in children <2 years of age. Common side effects include dizziness, headaches, visual and gastro-intestinal disturbances. If serious CNS symptoms develop (confusion, severe headaches) the prophylaxis must be stopped. Do not recommend for patients with history of convulsions, mental disorders or cardiac patients (quinine-like effect). Mefloquine side effects have been overstated in the early literature; a recent study of tolerability have shown that mefloquine was well tolerated. Mefloquine has been used for prophylaxis since 1986 by about 12 million travelers. The drug has a long half-life (21 days) and is highly effective in preventing P. falciparum and P. vivax malaria: the prophylac-
Louisiana Office of Public Health – Infectious Disease Epidemiology Section- Infectious Disease Control Manual
tic effectiveness of 250 mg of mefloquine weekly was more than 90% in East and West Africa and 100% in Irian Jaya. Anecdotal reports, especially in the United Kingdom, have raised public concern about the tolerance of mefloquine prophylaxis, ie, whether it causes neuropsychiatric events. Adverse reactions are not uncom- mon when the drug is used for treatment. However, when the drug is used for prophylaxis, it has rarely been associated with serious neuropsychiatric problems. The incidence of schizophrenic or schizophreni- form and bipolar affective disorders and seizures was 0.54 per 1,000 person/years among 52,981 Euro- pean travelers. Of interest, the background incidence of these disorders in the general US population is 16-fold higher than these rates among users of mefloquine, suggesting that these disorders are unlikely to be caused by mefloquine. Data from 13 prospective cohort studies (including 6 randomized, double-blinded, placebo-controlled tri- als with 528 users of mefloquine) and 7 comparative studies (N=55,130) have failed to show important differences between adverse events among users of mefloquine, other antimalarial drugs, or placebo. This observation applies to gastrointestinal as well as to various, often subjective neuropsychological symptoms, such as insomnia, fatigue, dizziness, anxiety, anorexia, confusion, and mood changes. Impor- tantly, several studies have assessed subjective complaints by objective standardized measurements. Such tests evaluating sleep and wake cycles, symptoms and moods, and psychomotor function, including use of flight simulators and driving tests, also have not detected adverse effects of mefloquine. Regarding restrictions on use of mefloquine, there is no evidence to justify precautions for its use in indi- viduals taking -blockers or calcium channel blockers to control hypertension. Restricting use of meflo- quine among persons engaged in tasks requiring fine coordination, such as pilots or drivers, does not ap- pear to be necessary. Pregnancy need not to preclude use of mefloquine: use of mefloquine during the second and third trimesters did not adversely affect the outcome of pregnancy, and the frequencies of spontaneous abortions and congenital malformations in 1133 women exposed to mefloquine during the first trimester were within the expected background rates. Quinine has a short half life and should be used only for treatment and administered in 3 doses /day. Pa- tients and some physicians are concerned by the number of tablets to take (6 /day). Lower doses are not recommended. Doxycycline is a photosensitizer and patient should be advised to apply sunscreen. Do not prescribe for pregnant women or children. In supervised studies, the protective efficacy of doxycycline ranged from 87% to 98% against P. falciparum and P. vivax in Thailand and 93% in Kenya. In contrast, its effectiveness was 64% in unsupervised studies in Thailand. Among US troops in Somalia, the attack rate of P falciparum ma- laria was 5-fold higher among users of doxycycline then among users of mefloquine. Doxycycline has a short half-life (16 hours), and its low prophylactic effectiveness in these settings has been attributed to poor compliance with the daily dosing. Another problem is that it should not be taken by pregnant women or by children younger than 8 years. Reported adverse effects include nausea, Candida vaginitis, esophagitis, gastrointestinal problems, and photosensitivity. Halofantrine is not available everywhere. Malaria in a pregnant woman increases the risk of maternal death, neonatal death, miscarriage and still birth. Chloroquine and proguanil are safe prophylactic drugs. Mefloquine is not recommended before the 4th month of pregnancy. Doxycycline is not recommended. Women of childbearing age should avoid get- ting pregnant while on doxycycline (up to a week after stopping) or while on mefloquine (up to 3 months after stopping). This measure is precautionary, no harmful effects have been demonstrated after inadver- tent use of mefloquine in pregnant women.
Louisiana Office of Public Health – Infectious Disease Epidemiology Section- Infectious Disease Control Manual
MODERNIZACJA KATASTRU JAKO PROCES WZBOGACANIA ZBIORÓW INFORMACJI O PRZESTRZENI . POLSKIE TOWARZYSTWO INFORMACJI PRZESTRZENNEJROCZNIKI GEOMATYKI 2009 m TOM VII m ZESZYT 5(35)MODERNISATION OF CADASTRE AS AN ENLARGEMENTFOR IMPLEMENTATION OF THE INSPIRE DIRECTIVETadeusz Koka1, El¿bieta Kamierczak-Koka21 Katedra Geodezji, Kartografii rodowiska i Geometrii Wykelnej,Wydzia³ Budownictw
NATIONAL POISONS INFORMATION SERVICE RECOMMENDATIONS FOR STOCKING BY ACUTE HOSPITALS OF ANTIDOTES AND OTHER DRUGS USED IN THE TREATMENT OF POISONING Updated - June 2006 This document lists the antidotes and other medicines that the National Poisons Information Service (NPIS) may recommend in the treatment of poisoning and provides recommendations for acute hospitals on arrangements f
 Infectious Disease Epidemiology Section
Infectious Disease Epidemiology Section 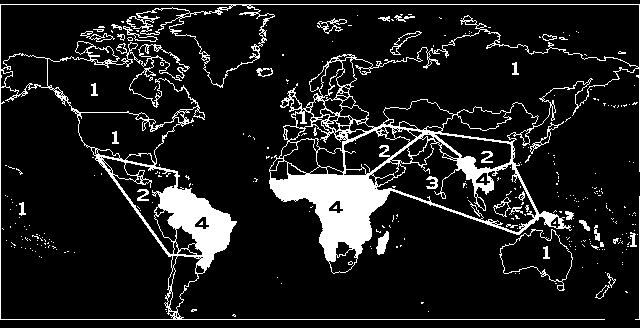 Malaria Endemic Areas (see page one for explanation of numbers)
Malaria Endemic Areas (see page one for explanation of numbers)