Microsoft word - eu-smpc nuvaring ra 0550 eu s2 _ref 1.0_ english .doc
NUVARING NAME OF THE MEDICINAL PRODUCT NuvaRing® 2. QUALITATIVE QUANTITATIVE COMPOSITION
NuvaRing contains 11.7 mg etonogestrel and 2.7 mg ethinylestradiol. The ring releases etonogestrel and ethinylestradiol at an average amount of 0.120 mg and 0.015 mg, respectively per 24 hours, over a period of 3 weeks. For excipients, see 6.1.
3. PHARMACEUTICAL
NuvaRing is flexible, transparent, colorless to almost colorless ring, with an outer diameter of 54 mm and a cross-sectional diameter of 4 mm.
4. CLINICAL PARTICULARS 4.1 Therapeutic indications
NuvaRing is intended for women of fertile age. The safety and efficacy has been established in women aged 18 to 40 years.
Posology and method of administration
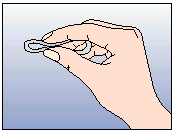
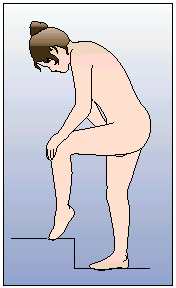
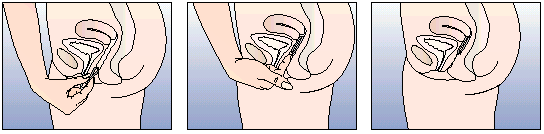
The woman herself can insert NuvaRing in the vagina. The physician should advise the woman how to insert and remove NuvaRing. For insertion the woman should choose a position that is most comfortable for her, e.g. standing with one leg up, squatting, or lying down. NuvaRing should be compressed and inserted into the vagina until it feels comfortable. The exact position of NuvaRing in the vagina is not critical for the contraceptive effect of the ring (see Figures 1-4).
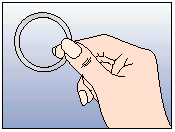
Once NuvaRing has been inserted (see ‘How to start NUVARING’) it is left in the vagina continuously for 3 weeks. If NuvaRing is accidentally expelled (e.g. while removing a tampon), it can be rinsed with cool to lukewarm (not hot) water and should be reinserted immediately. NuvaRing must be removed after 3 weeks of use on the same day of the week as the ring was inserted. After a ring-free interval of one week a new ring is inserted (e.g. when NuvaRing is inserted on a Wednesday at about 22.00 h the ring should be removed again on the Wednesday 3 weeks later at about 22.00 h. The following Wednesday a new ring should be inserted). NuvaRing can be removed by hooking the index finger under the ring or by grasping the ring between the index and middle finger and pulling it out. The used ring should be placed in the sachet (keep out of the reach of children and pets) and discarded as described in Section 6.6. The withdrawal bleed usually starts 2-3 days after removal of NuvaRing and may not have finished completely before the next ring insertion is due.
NUVARING Figure 1 Take NuvaRing out of the sachet Choose a comfortable position to Figure 4A Figure 4B Figure 4C Insert the ring into the vagina with one hand (Figure 4A), if necessary the labia may be spread with the other. Push the ring into the vagina until the ring feels comfortable (Figure 4B). Leave the ring in place for 3 weeks (Figure 4C).No hormonal contraceptive use in the preceding cycle
Counting the first day of menstruation as ‘Day 1’, NuvaRing should be inserted between Day 1 and 5, but at the latest on Day 5 of the cycle, even if the woman has not finished her menstrual bleed. During the very first 7 days of NuvaRing use, it is recommended to additionally use a barrier method such as a condom.
Changing from a combined oral contraceptive (COC)
The woman should insert NuvaRing at the latest on the day fol owing the usual tablet-free or placebo tablet interval of her previous COC.
Changing from a progestagen-only method, e.g. progestagen-only-pill (POP or minipill), implant or injection
The woman may switch on any day from the POP. She should switch from an implant on the day of its removal and from an injectable on the day when the next injection would be due. In al of these cases, the woman should use
NUVARING
an additional barrier method for the first 7 days.
The woman may start immediately. When doing so, she needs not to take additional contraceptive measures. If an immediate switch is considered undesirable, the woman should follow the advice given for ‘no hormonal contraceptive use in the preceding cycle’. In the mean-time, she should be advised to use an alternative contraceptive method.
Following delivery or second-trimester abortion
For breast-feeding women, see Section 4.6.
Women should be advised to start during the fourth week after delivery or second-trimester abortion. When starting later, the woman should be advised to additionally use a barrier method for the first 7 days of NuvaRing use. However, if intercourse has already occurred, pregnancy should be excluded or the woman has to wait for her first menstrual period, before starting NuvaRing use.
Contraceptive efficacy and cycle control may be compromised if the woman deviates from the recommended regimen. To avoid loss of contraceptive efficacy in case of a deviation, the following advice can be given:
• What to do in case of a lengthened ring-free interval
The woman should insert a new ring as soon as she remembers. A barrier method such as a condom should be used in addition for the next 7 days. If intercourse took place during the ring-free interval, the possibility of a pregnancy should be considered. The longer the ring-free interval, the higher the risk of a pregnancy.
• What to do if the ring was temporarily outside the vagina
NuvaRing should be left in the vagina for a continuous period of 3 weeks. If the ring is accidentally expelled and is left outside of the vagina for less than 3 hours contraceptive efficacy is not reduced. The woman should reinsert the ring as soon as possible, but at the latest within 3 hours.
If NuvaRing has been out of the vagina for more than 3 hours, contraceptive efficacy may be reduced. The woman should reinsert the ring as soon as she remembers. A barrier method such as a condom should be used in addition until NuvaRing has been in the vagina continuously for 7 days. If the first of these 7 days fall within the third week of ring use, it means that NuvaRing should then be used for more than three weeks. The ring should subsequently be removed and a new ring inserted, after a ring- free interval of one week. If ring removal for more than 3 hours occurs during the first week of ring use, the possibility of pregnancy should be considered.
• What to do in case of lengthened ring-use
As long as NuvaRing has been used for maximally 4 weeks, contraceptive efficacy is still adequate. The woman may maintain her one-week ring-free interval and subsequently insert a new ring. If NuvaRing has been left in place for more than 4 weeks, contraceptive efficacy may be reduced and pregnancy should be ruled out before inserting a new NuvaRing. NUVARING
If the woman has not adhered to the recommended regimen and subsequently has no withdrawal bleed in the following ring-free interval, pregnancy should be ruled out before inserting a new NuvaRing.
HOW TO SHIFT PERIODS OR HOW TO DELAY A PERIOD
delay a period the woman may insert a new ring without having a ring-
free interval. The next ring can be used for up to 3 weeks again. The woman may experience bleeding or spotting. Regular use of NuvaRing is then resumed after the usual one week ring-free interval.
shift her period to another day of the week than the woman is used to
with her current scheme, she can be advised to shorten her forthcoming ring-free interval by as many days as she likes. The shorter the ring-free interval, the higher the risk that she does not have a withdrawal bleed and will experience breakthrough bleeding and spotting during the use of the next ring.
4.3 Contraindications
NuvaRing should not be used in the presence of any of the conditions listed below. Should any of the conditions appear for the first time during the use of NuvaRing, it should be removed immediately.
Presence or history of venous thrombosis, with or without the involvement of pulmonary embolism.
Presence or history of arterial thrombosis (e.g. cerebrovascular accident, myocardial infarction) or prodromi of a thrombosis (e.g. angina pectoris or transient ischaemic attack).
Known predispostion for venous or arterial thrombosis, with or without hereditary involvement such as Activated Protein C (APC) resistance, antithrombin-III deficiency, protein C deficiency, protein S deficiency, hyperhomocysteinaemia and antiphospholipid antibodies (anticardiolipin antibodies, lupus anticoagulant).
Diabetes mellitus with vascular involvement.
The presence of a severe or multiple risk factor(s) for venous or arterial thrombosis may also constitute a contraindication (see under ‘Special warnings and special precautions for use’).
Presence or history of severe hepatic disease as long as liver function values have not returned to normal.
Presence or history of liver tumors (benign or malignant).
Known or suspected malignant conditions of the genital organs or the breasts, if sex steroid-influenced.
Hypersensitivity to the active substances or to any of the excipients of NuvaRing
NUVARING Special warnings and special precautions for use
If any of the conditions/risk factors mentioned below is present, the benefits of the use of NuvaRing should be weighed against the possible risks for each individual woman and discussed with the woman before she decides to start using it. In the event of aggravation, exacerbation or first appearance of any of these conditions or risk factors, the woman should contact her physician. The physician should then decide on whether its use should be discontinued. All data presented below are based upon epidemiological data obtained with combined oral contraceptives (COC). No epidemiological data are available on vaginal route of administration for the hormones but the warnings are also considered applicable to the use of NuvaRing.
• The use of hormonal contraceptives has been associated with the
occurrence of venous thrombosis (deep venous thrombosis and pulmonary embolism) and arterial thrombosis and associated complications, sometimes with fatal consequences.
• Use of any combined oral contraceptive (COC) carries an increased
risk of venous thromboembolism (VTE) compared with no use. This increased risk is less than the risk of VTE associated with pregnancy, which is estimated as 60 per 100 000 pregnant woman years. VTE is fatal in 1%-2% of cases. It is not known how NuvaRing influences the risk compared with other COCs.
• Extremely rarely, thrombosis has been reported to occur in other blood
vessels, e.g. hepatic, mesenteric, renal, cerebral or retinal veins and arteries, in COC users. There is no consensus as to whether the occurrence of these events is associated with the use of COCs.
• Symptoms of venous or arterial thrombosis can include: unilateral leg
pain and / or swelling; sudden severe pain in the chest, whether or not it radiates to the left arm; sudden breathlessness; sudden onset of coughing; any unusual, severe, prolonged headache; sudden partial or complete loss of vision; diplopia; slurred speech or aphasia; vertigo; collapse with or without focal seizure; weakness or very marked numbness suddenly affecting one side or one part of the body; motor disturbances; ‘acute’ abdomen.
• The risk of venous thromboembolism (VTE) increases with:
− a positive family history (i.e. venous thromboembolism ever in a sibling
or parent at a relatively early age). If a hereditary predisposition is suspected, the woman should be referred to a specialist for advice before deciding about any hormonal contraceptive use;
− prolonged immobilization, major surgery, any surgery to the legs, or
major trauma. In these situations it is advisable to discontinue use (in the case of elective surgery at least four weeks in advance) and not to resume until two weeks after complete remobilization.
− obesity (body mass index over 30 kg/m2);
− and possibly also with superficial thrombophlebitis and varicose veins.
There is no consensus about the possible role of these conditions in
NUVARING
• The risk of arterial thromboembolic complications increases with:
− smoking (with heavier smoking and increasing age the risk further
increases, especial y in women over 35 years of age);
− obesity (body mass index over 30 kg/m2);
− a positive family history (arterial thrombosis ever in a sibling or parent
at a relatively early age). If a hereditary predisposition is suspected, the woman should be referred to a specialist for advice before deciding about any hormonal contraceptive use;
• Biochemical factors that may be indicative of hereditary or acquired
predisposition for venous or arterial thrombosis include Activated Protein C (APC) resistance, hyperhomocysteinaemia, antithrombin-III deficiency, protein C deficiency, protein S deficiency, antiphospholipid antibodies (anticardiolipin antibodies, lupus anticoagulant).
• Other medical conditions, which have been associated with adverse
circulatory events, include diabetes mellitus, systemic lupus erythematosus, hemolytic uraemic syndrome, chronic inflammatory bowel disease (e.g. Crohn's disease or ulcerative colitis).
• The increased risk of thromboembolism in the puerperium must be
considered (for information on ‘Pregnancy and Lactation’ see Section 4.6).
• An increase in frequency or severity of migraine (which may be
prodromal of a cerebrovascular event) may be a reason for immediate discontinuation of NuvaRing use.
• Women using COCs should be specifically pointed out to contact their
physician in case of possible symptoms of thrombosis. In case of suspected or confirmed thrombosis, COC use should be discontinued. Adequate contraception should be initiated because of the teratogenicity of anti-coagulant therapy (coumarins).
• An increased risk of cervical cancer in long-term users of COCs has
been reported in some epidemiological studies, but there continues to be controversy about the extent to which this finding is attributable to the confounding effects of sexual behavior and other factors such as human papilloma virus (HPV).
• A meta-analysis from 54 epidemiological studies reported that there is
a slightly increased relative risk (RR = 1.24) of having breast cancer diagnosed in women who are currently using COCs. The excess risk gradually disappears during the course of the 10 years after cessation of COC use. Because breast cancer is rare in women under 40 years of age, the excess number of breast cancer diagnoses in current and recent COC users is small in relation to the overall risk of breast cancer. The breast cancers diagnosed in ever-users tend to be less advanced clinically than the cancers diagnosed in never-users. The
NUVARING
observed pattern of increased risk may be due to an earlier diagnosis of breast cancer in COC users, the biological effects of COCs or a combination of both.
• In rare cases, benign liver tumors, and even more rarely, malignant liver
tumors have been reported in users of COCs. In isolated cases, these tumors have led to life-threatening intra-abdominal hemorrhages. Therefore, a hepatic tumor should be considered in the differential diagnosis when severe upper abdominal pain, liver enlargement or signs of intra-abdominal hemorrhage occur in women using NuvaRing.
• Women with hypertriglyceridemia, or a family history thereof, may be at
an increased risk of pancreatitis when using hormonal contraceptives.
• Although small increases in blood pressure have been reported in many
women using hormonal contraceptives, clinically relevant increases are rare. A definitive relationship between hormonal contraceptive use and clinical hypertension has not been established. However, if a sustained clinically significant hypertension develops during the use of NuvaRing then it is prudent for the physician to suspend the use of the ring and treat the hypertension. Where considered appropriate, NuvaRing use may be resumed if normotensive values can be achieved with antihypertensive therapy.
• The following conditions have been reported to occur or deteriorate with
both pregnancy and during the use of hormonal contraceptives, but the evidence of an association with its use is inconclusive: jaundice and / or pruritus related to cholestasis; gallstone formation; porphyria; systemic lupus erythematosus; hemolytic uraemic syndrome; Sydenham’s chorea; herpes gestationis; otosclerosis-related hearing loss.
• Acute or chronic disturbances of liver function may necessitate the
discontinuation of the use of NuvaRing until markers of liver function return to normal. Recurrence of cholestatic jaundice and/ or pruritus related to cholestasis, which occurred first during pregnancy or previous use of sex steroids necessitates the discontinuation of the ring.
• Although estrogens and progestagens may have an effect on peripheral
insulin resistance and glucose tolerance, there is no evidence for a need to alter the therapeutic regimen in diabetics using hormonal contraception. However, diabetic women should be carefully monitored while using NuvaRing especial y in the first months of use.
• A deterioration of Crohn’s disease and colitis ulcerosa has been
reported in association with the use of hormonal contraceptives.
• Chloasma may occasionally occur, especially in women with a history of
chloasma gravidarum. Women with a tendency to chloasma should avoid exposure to the sun or ultraviolet radiation whilst using NuvaRing.
• If a woman has any of the following conditions she may not be able to
insert NuvaRing correctly or may in fact lose the ring: prolapse of the uterine cervix, cystocele and or rectocele, severe or chronic constipation.
• During the use of NuvaRing, women may occasional y experience
vaginitis. There are no indications that the efficacy of NuvaRing is affected by the treatment of vaginitis, nor that the use of NuvaRing affects the treatment of vaginitis.
Prior to the initiation or reinstitution of NuvaRing use a complete medical history (including a family medical history) should be taken and pregnancy
NUVARING
should be excluded. The blood pressure and a physical examination should be taken, guided by the contraindications (Section 4.3) and warnings (Section 4.4). The woman should be advised to carefully read the package leaflet and to follow the advice given. The frequency and nature of further periodic checks should be based upon established clinical practice and adapted to the individual woman. .
Women should be advised that NuvaRing does not protect against HIV infections (AIDS) and other sexually transmitted diseases.
The efficacy of NuvaRing may be reduced in the event of non-compliance (Section 4.2), or concomitant medication (Section 4.5).
Irregular bleeding (spotting or breakthrough bleeding) may occur during the use of NuvaRing. If bleeding irregularities occur after previously regular cycles while NuvaRing has been used according to the recommended regimen, then non-hormonal causes should be considered, and adequate diagnostic measures are indicated to exclude malignancy or pregnancy. These may include curettage.
In some women a withdrawal bleed may not occur during the ring-free interval. If NuvaRing has been used according to the instructions described in Section 4.2, it is unlikely that the woman is pregnant. However, if NuvaRing has not been used according to these instructions prior to the first missed withdrawal bleed or if two withdrawal bleeds are missed, pregnancy must be ruled out before use of NuvaRing is continued.
MALE EXPOSURE TO ETHINYL ESTRADIOL AND ETONOGESTREL
The extent and possible pharmacological role of exposure of male sexual partners to ethinylestradiol and etonogestrel through absorption through the penis have not been examined.
Interaction with other medicinal products and other forms of interaction
Interactions between hormonal contraceptives and other medicinal products may lead to breakthrough bleeding and/or contraceptive failure. The following interactions have been reported in the literature.
Hepatic metabolism: Interactions can occur with medicinal products that induce microsomal enzymes, which can result in increased clearance of sex hormones (e.g., phenytoin, phenobarbital, primidone, carbamazepine, rifampicin, and possibly also oxcarbazepine, topiramate, felbamate, ritonavir, griseofulvin and products containing St. John’s wort).
Interference with Enterohepatic Circulation: Some clinical reports suggest that enterohepatic circulation of estrogens may decrease when certain antibiotic agents are given, which may reduce ethinyl estradiol
NUVARING
concentrations (e.g., penicillins, tetracyclines).
Women on treatment with any of these drugs should temporarily use a barrier method in addition to NuvaRing or choose another method of contraception. With microsomal enzyme-inducing drugs, the barrier method should be used during the time of concomitant drug administration and for 28 days after their discontinuation. Women on treatment with antibiotics (except rifampicin and griseofulvin) should use the barrier method until 7 days after discontinuation. If concomitant drug administration runs beyond the 3 weeks of a ring-cycle, the next ring should be inserted immediately, without having the usual ring-free interval.
Based on pharmacokinetic data, vaginally administered antimycotics and spermicides are unlikely to affect the contraceptive efficacy and safety of NuvaRing.
The use of contraceptive steroids may influence the results of certain laboratory tests, including biochemical parameters of liver, thyroid, adrenal and renal function, plasma levels of carrier proteins, (e.g. corticosteroid binding globulin and sex hormone binding globulin), lipid / lipoprotein fractions, parameters of carbohydrate metabolism and parameters of coagulation and fibrinolysis. Changes generally remain within the normal laboratory range.
4.6 Pregnancy lactation
NuvaRing is not indicated during pregnancy. If pregnancy occurs with NuvaRing in situ, the ring should be removed. Extensive epidemiological studies have revealed neither an increased risk of birth defects in children born to women who used COCs prior to pregnancy, nor a teratogenic effect when COCs were used inadvertently during early pregnancy.
Due to the intravaginal administration, intrauterine concentrations of the contraceptive steroids in NuvaRing are likely to be higher than in COC users. An effect on the foetus can therefore not be excluded. Clinical experience of the outcomes of pregnancies exposed to NuvaRing has not been reported
Lactation may be influenced by estrogens, as they may reduce the quantity and change the composition of breast milk. Therefore, the use of NuvaRing should generally not be recommended until the nursing mother has completely weaned her child. Small amounts of the contraceptive steroids and / or their metabolites may be excreted with the milk but there is no evidence that this adversely affects the infant’s health.
Effects on ability to drive and use machines
On the basis of the pharmacodynamic profile, NuvaRing is expected to have no or negligible influence on the ability to drive and use machines.
4.8 Undesirable
The most frequently reported undesirable effects in the clinical trials with
NUVARING
NuvaRing were headache and vaginitis and leukorrhoea, each reported by 5-6% of the women. Possibly related undesirable effects have been listed in the Table below.
Frequency of adverse reactions Body system Uncommon
≥ 1/100 < 1/100, ≥ 1/1000
breast pain, device-related problems (e.g. expulsion, coital problems and foreign body feeling), dysmenorrhoea, leukorrhoea, vaginal discomfort, vaginitis
A number of undesirable effects have been reported in women using combined oral contraceptives, which are discussed in more detail in Section 4.4 Special warnings and precautions for use. These include: Venous thromboembolic disorders; Arterial thromboembolic disorders; Hypertension; Hormone-dependent tumours (e.g. liver tumours, breast cancer); Chloasma.NUVARING 4.9 Overdose
There have been no reports of serious deleterious effects from an overdose of hormonal contraceptives. Symptoms that may occur in this case are: nausea, vomiting and, in young girls, slight vaginal bleeding. There are no antidotes and further treatment should be symptomatic.
PHARMACOLOGICAL PROPERTIES 5.1 Pharmacodynamic properties
NuvaRing contains etonogestrel and ethinylestradiol. Etonogestrel is a 19- nortestosterone-derived progestagen and binds with high affinity to progesterone receptors in the target organs. Ethinylestradiol is an estrogen widely used in contraceptive products. The contraceptive effect of NuvaRing is based on various mechanisms, the most important of which is the inhibition of ovulation.
Clinical studies were performed in women between the age of 18 and 40 years. During these clinical investigations performed in paral el in Europe and in the USA the total exposure was more than 23,000 cycles. In Europe the following results were obtained:
Analysis method Number of Analysis method Number of
The different results obtained are mainly ascribed to the lower degree of
compliance to the recommended dose regimen in the US study. In addition, temporary removals beyond 3 hours (for which condition no standard back-up contraception was advised) were more frequent in the US study.
To limit the risk of unwanted pregnancies during actual use, the recommendations for use have been tightened compared to those applied in the clinical investigations. This mainly concerns the advice to use the ring for 3 weeks continuously and to use a barrier method in case of deviations from the recommended use (see Section 4.2).
With the use of higher-dosed COCs (0.050 mg ethinylestradiol) the risk of endometrial and ovarian cancer is reduced. Whether this also applies to a lower-dosed contraceptive like NuvaRing remains to be determined.
NUVARING 5.2 Pharmacokinetic properties Etonogestrel
Etonogestrel released by NuvaRing is rapidly absorbed by the vaginal mucosa. Maximum serum concentrations of etonogestrel of approximately 1700 pg/mL are reached at about 1 week after insertion. Serum concentrations show small fluctuations and slowly decrease to approximately 1400 pg/mL after 3 weeks. Absolute bioavailability is approximately 100%, which is higher than after oral administration.
Etonogestrel is bound to serum albumin and to sex hormone binding globulin (SHBG). The apparent volume of distribution of etonogestrel is 2.3 L/kg.
Etonogestrel is metabolized by the known pathways of steroid metabolism. The apparent clearance from serum is about 3.5 L/h. No direct interaction was found with the co-administered ethinylestradiol.
Etonogestrel serum levels decrease in two phases. The terminal elimination phase is characterized by a half-life of approximately 29 hours. Etonogestrel and its metabolites are excreted at a urinary to biliary ratio of about 1.7:1. The half-life of metabolite excretion is about 6 days.
Ethinylestradiol
Ethinylestradiol released by NuvaRing is rapidly absorbed by the vaginal mucosa. Maximum serum concentrations of about 35 pg/mL are reached 3 days after insertion and decrease to 18 pg/mL after 3 weeks. Absolute bioavailability is approximately 56%, which is comparable with oral administration of ethinylestradiol.
Ethinylestradiol is highly but non-specifically bound to serum albumin. An apparent volume of distribution of about 15 L/kg was determined.
Ethinylestradiol is primarily metabolized by aromatic hydroxylation but a wide variety of hydroxylated and methylated metabolites are formed. These are present as free metabolites and as sulfate and glucuronides conjugates. The apparent clearance is about 35 L/h.
Ethinylestradiol serum levels decrease in two phases. The terminal elimination phase is characterized by a large individual variation in half-life, resulting in a median half-life of approximately 34 hours. Unchanged ethinylestradiol is not excreted; ethinylestradiol metabolites are excreted at a urinary to biliary ratio of 1.3:1. The half-life of metabolite excretion is about 1.5 days.
5.3 Preclinical
Preclinical data with ethinylestradiol and etonogestrel reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential and toxicity to
NUVARING
reproduction, other than those already known for humans.
6. PHARMACEUTICAL PARTICULARS List of excipients
Ethylene vinylacetate copolymer, 28% vinylacetate;
ethylene vinylacetate copolymer, 9% vinylacetate; magnesium stearate.
6.2 Incompatibilities 6.3 Shelf Special precautions for storage
The dispenser places a date of dispensing on the box. The product should not be inserted after 4 months from the date of dispensing or the expiry date, whichever comes first. After dispensing:
Nature and contents of container
Sachet containing one NuvaRing. The sachet is made of aluminum foil with an inner layer of low-density polyethylene and an outer layer of polyester. It is reclosable and waterproof. The sachet is packed in a printed cardboard box together with the package leaflet. Each box contains 1 or 3 rings.
Instructions for use / handling, and disposal
See Section 4.2: ‘Posology and method of administration’. The dispenser has to indicate the date of dispensing and the date before which NuvaRing has to be used on the box. After removal, NuvaRing should be replaced in the reclosable sachet and disposed of with the normal household waste in a manner that avoids accidental contact with others. NuvaRing should not be flushed down the toilet.
7. MARKETING AUTHORISATION NUVARING 8. MARKETING AUTHORIZATION DATE OF FIRST AUTHORISATION / RENEWAL OF THE AUTHORISATION DATE OF REVISION OF THE TEXT
Irrigación nasal hipersalina en niños con rinitis alérgica estacional sintomática Irrigación nasal hipersalina en niños con rinitis alérgica estacional sintomática Un estudio aleatorio Werner Garavello1, Marco Romagnoli1, Lorenza Sordo1,Renato Maria Gaini1, Cristina Di Berardino2 y Alfonso Angrisano2 Introducción Evidencia reciente sugiere que la irrigación nasal conLa rinitis a
Curriculum vitae Insaf Fadl khalil Education 2000 PhD , graduated from University of Copenhagen, Faculty of Health Science. Thesis: Cotrimoxazole and Fansidar in the treatment of acute uncomplicated falciparum malaria: Efficacy, safety and molecular characterisation of resistance. 1996 Diploma in Tropical Medicine and International Health, University of Copenhagen, MS (Medical
 NUVARING
NUVARING