Toxoplasma gondii is an intracellular coccidian parasite and is one of the most common parasitic diseases of animals and man. The definitive hosts for the parasite (the only animals in which the organism reproduces sexually) are members of the Felidae family (mainly domestic cats). T gondii is of primary importance since the range of intermediate hosts which can become infected encompasses virtually all warm-blooded animals, including man. Although infection with T gondii is extremely common, it is rarely a cause of significant disease in any species.
Life cycle
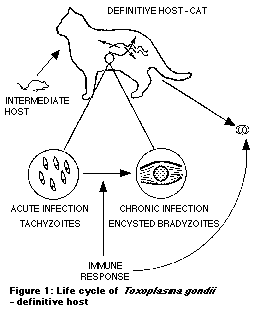
Cats usually become infected with T gondii by ingestion of encysted organisms present in the tissues of a chronically infected intermediate host. The cyst wall is digested by the cat, releasing infectious organisms into the intestinal lumen. The organisms penetrate through the intestinal wall and replicate throughout the body as rapidly dividing tachyzoites (extra-intestinal cycle). Simultaneously, the organisms invade and replicate within the intestinal epithelial cells (entero-epithelial cycle). This entero-epithelial cycle culminates in sexual reproduction and the formation of oocysts (eggs) which are excreted in the faeces. As the cat develops an immune response, oocyst shedding is halted, and the development of tachyzoites is also arrested with the resultant formation of bradyzoites (slowly replicating forms of the organism) contained within tissue cysts. Tissue cysts are present in a variety of sites throughout the body of chronically infected animals, each cyst containing large numbers of bradyzoites.
Cats previously unexposed to T gondii usually begin shedding oocysts between 3 and 10 days after ingestion of infected tissue, and continue shedding for around 10-14 days, during which time many millions of oocysts may be produced. Once a cat has developed an immune response, further shedding of oocysts is extremely rare.
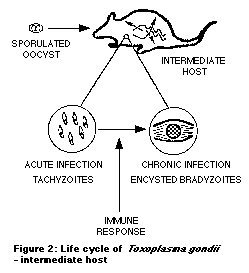
After oocysts have been passed in the faeces, they undergo sporulation (formation of infection sporozoites within the oocyst). This process takes 1-5 days depending on environmental conditions and, prior to this, they are not infectious. Oocysts are very resistant and may survive in the environment for well over a year.
Intermediate hosts (e.g. rodents, birds, sheep, pigs, cattle) may become infected by ingestion of sporulated oocysts. As in the cat, an extra-intestinal cycle of infection occurs, and the subsequent immune response results in the development of encysted bradyzoites. The tissue cysts probably remain viable (contain infectious organisms) for the life of the animal. Unlike infection in the cat, an enteroepithelial cycle (with oocyst production) does not occur in intermediate hosts. Encysted bradyzoites are infectious to cats, and importantly, also to other intermediate hosts, so that in man for example, infection may be acquired either through the ingestion of oocysts, or through the ingestion of cysts within infected meat.
In addition to ingestion of sporulated oocysts or bradyzoites, infection with T gondii may also be acquired by a foetus in utero (transplacental infection). This can only occur if the host acquires infection during pregnancy, as it is only tachzoites (present during the acute stage of infection) that are able to cross the placenta.
Despite the high prevalence of T gondii infection, significant clinical disease in cats (and other species) appears to be very rare. When disease does occur, it may develop either following primary infection (where an inadequate immune response fails to arrest the invasive tachyzoites), or as a result of reactivated infection (where compromised immunity allows the reactivation of infection from encysted bradyzoites with the formation of invading, multiplying tachyzoites).
Clinical disease appears to be most common in young cats (less than 2 years of age), and this may be due, in part, to a poorly developed immune response in these cats. Reactivation of infection in older cats may be linked to co-infection with feline leukaemia virus or feline immunodeficiency virus in some cats.
The most commonly reported clinical signs associated with feline toxoplasmosis are anorexia, weight loss, lethargy, difficulty breathing (due to pneumonia), ocular signs and high temperature. Other less common features include gastrointestinal signs (vomiting/diarrhoea), neurological signs and jaundice.
Detection of oocysts Faecal samples may be examined for the presence of T gondii oocysts, although this test is both technically difficult and requires experience to correctly identify the oocysts. Furthermore, clinical signs usually do not develop until after oocyst shedding has ceased. For these reasons, oocyst detection is rarely helpful. Treatment of feline toxoplasmosis In the past, treatment for toxoplasmosis has been based on a combination of sulphadiazine and pyrimethamine. However, recently, clindamycin used at doses of 25-50mg/kg/day (divided into two or four doses) has been suggested as the treatment of choice in feline toxoplasmosis. Although it has been proposed that the use of clindamycin obviates the need for concurrent pyrimethamine therapy, studies in man suggest dual therapy is still required to maintain efficacy. The situation in cats is unclear, but combining clindamycin with pyrimethamine (at 1mg/kg/day) may provide more effective therapy. Pyrimethamine therapy is often associated with myleosuppression and, to avoid this, cats may be given folic acid at 5mg/day for the duration of treatment. The zoonotic potential of T gondii Toxoplasmosis is an important zoonotic disease. Around 30% of the adult population in the UK have serological evidence of infection but, as with cats, the vast majority of these human infections are either asymptomatic or result in only mild clinical disease. Of major concern however, is congenitally acquired toxoplasmosis. As noted above, this can only occur when a previously unexposed (non-immune) woman acquires toxoplasmosis during pregnancy. In this situation there is approximately a 40% chance that the foetus will acquire the infection, and in around 10% of these cases, severe neurological or ocular disease is present at birth. Most surveys show that owning a cat or having direct contact with a cat does not constitute an increased risk of acquiring toxoplasmosis. Although cats are crucial in the life-cycle of T gondii, and are the only known source of oocysts present in the environment, it is stray and feral cats more than pet cats that are implicated in this. In the UK and other industrialised countries, it is mainly adolescent and adult humans who acquire infection with T gondii, and this is primarily correlated with the acquired habits of eating undercooked meat, and of poor meat hygiene. Ingestion of infected meat therefore appears to be the major source of human infection in the UK.
Following a few sensible environmental and meat hygiene measures can greatly reduce the risk of human infection.
Cook all meat thoroughly to at least 70°C Wash hands, utensils and surfaces carefully after handling raw meat Wash all vegetables carefully Wear gloves when gardening in soil potentially contaminated by cat faeces Empty cat litter trays daily, dispose of litter carefully and disinfect tray with
boiling water. If this is done every day, even if a cat is excreting oocysts, they will not have sporulated and therefore will not be infectious by the time the litter is changed
Discourage pet cats from hunting and avoid feeding raw/undercooked meat Cover any children's sandpits/boxes to prevent cats using them as a litter tray
Sleep Medicine Reviews (2008) 12, 153–162aSleep Disorders and Research Center, Henry Ford Hospital, 2799 W Grand Blvd, CFP-3, Detroit,MI 48202, USAbDepartment of Psychiatry and Behavioral Neuroscience, School of Medicine, Wayne State University,Detroit, MI, USACaffeine is one of the most widely consumed psychoactive substancesand it has profound effects on sleep and wake function. Laborat
UNIVERSIDAD DE CHILE Centro Interdisciplinario de Estudios en Bioética Ética de la Investigación Biomédica y Psicosocial Estudio de Caso: “Evaluación piloto de dos (2) regímenes antirretrovirales en un entorno de escasos recursos” Sede: Instituto Tecnológico de Santo Domingo, República Dominicana Alumno: César Lara Álvarez ([email protected]) Coordinador Local
 Toxoplasma gondii is an intracellular coccidian parasite and is one of the most common parasitic diseases of animals and man. The definitive hosts for the parasite (the only animals in which the organism reproduces sexually) are members of the Felidae family (mainly domestic cats). T gondii is of primary importance since the range of intermediate hosts which can become infected encompasses virtually all warm-blooded animals, including man. Although infection with T gondii is extremely common, it is rarely a cause of significant disease in any species.
Life cycle
Toxoplasma gondii is an intracellular coccidian parasite and is one of the most common parasitic diseases of animals and man. The definitive hosts for the parasite (the only animals in which the organism reproduces sexually) are members of the Felidae family (mainly domestic cats). T gondii is of primary importance since the range of intermediate hosts which can become infected encompasses virtually all warm-blooded animals, including man. Although infection with T gondii is extremely common, it is rarely a cause of significant disease in any species.
Life cycle