Allen N. Sapadin, MD, and Raul Fleischmajer, MD
Tetracyclines are broad-spectrum antibiotics that act as such at the ribosomal level where they interferewith protein synthesis. They were first widely prescribed by dermatologists in the early 1950s when it wasdiscovered that they were effective as a treatment for acne. More recently, biologic actions affectinginflammation, proteolysis, angiogenesis, apoptosis, metal chelation, ionophoresis, and bone metabolismhave been researched. The therapeutic effects of tetracycline and its analogues in various diseases havealso been investigated. These include rosacea, bullous dermatoses, neutrophilic diseases, pyodermagangrenosum, sarcoidosis, aortic aneurysms, cancer metastasis, periodontitis, and autoimmune disorderssuch as rheumatoid arthritis and scleroderma. We review the nonantibiotic properties of tetracycline and itsanalogues and their potential for clinical application. ( J Am Acad Dermatol 2006;54:258-65.)
Tetracyclines were discovered in 1948 as Abbreviationsused:
natural fermentation products of a soilbacterium, Streptomyces aureofaciens. The
first chemically purified tetracycline was chlortetra-
cycline Currently, 3 groups of tetracyclinesare available: tetracycline natural products, tetracy-cline semisynthetic compounds, and chemicallymodified tetracyclines (CMTs).Perusal of the
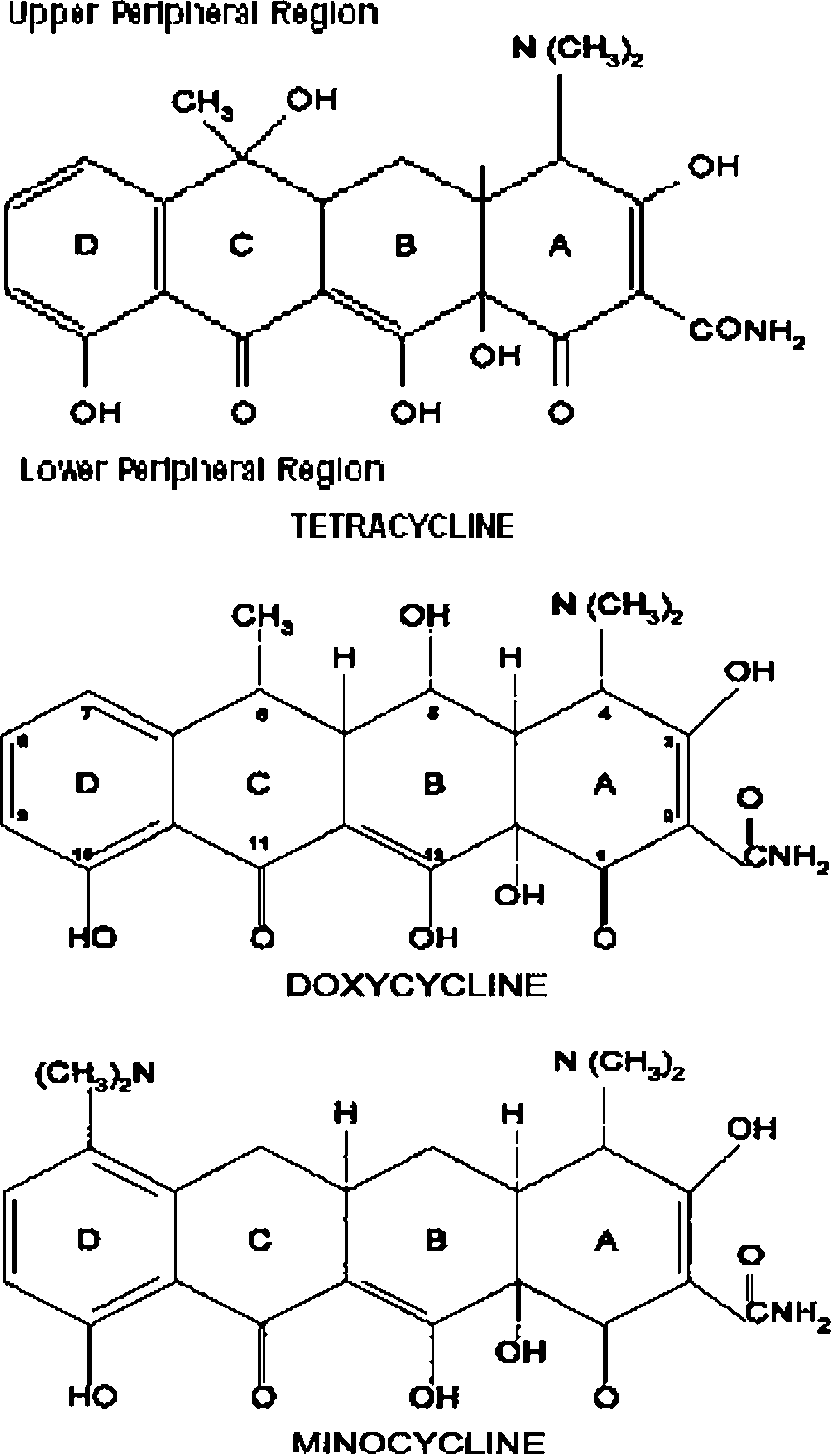
The ring structure of tetracyclines is surrounded
literature suggests that tetracyclines, besides acting
by upper and lower peripheral zones. These contain
as antibiotics, may also affect inflammation, immu-
various chemical functional groups and substitu-
Synthetic modification of the lower peripheral
region reduces both antibiotic and nonantibioticproperties. On the other hand, biological targets
may be enhanced by modifying the upper peripheral
Tetracyclines and analogues with biological
zone, particularly in positions C7 through C9 of the
effects on bacteria and mammalian targets show a
D ring. This has been accomplished with tetracycline
basic chemical structure consisting of a tetracyclic
semisynthetic compounds such as minocycline and
naphthacene carboxamide ring system ().
Tetracyclines with antibiotic activity have a dimethyl-amine group at carbon 4 (C4) in ring A. Removal ofthe dimethylamino group from C4 reduces its anti-
biotic properties, but enhances nonantibiotic ac-
Ionophores are organic compounds capable of
tions.Utilization of this strategy was the basis for
forming lipid-soluble complexes with metal cations.
the development of several chemically modified
Transportation of these cations across hydrophobic
barriers, such as artificial or biological membranes,is an important function of these compounds. Tetracyclines bind divalent metal cations, mostly
From the Department of Dermatology, Mount Sinai School of
along the lower peripheral region, and circulate in
blood plasma primarily as Ca11 and Mg11 chelates.
Funding sources: None. Conflicts of interest: None identified.
Their role as calcium ionophores has important
Reprint requests: Allen N. Sapadin, MD, Box 1048, Mount Sinai
biologic implications. After its intracellular incorpo-
School of Medicine, One Gustave L. Levy Place, New York, NY
ration, Ca11 can act as a secondary messenger
and affect pathways such as secretory processes,
receptor activation or inhibition, cell division, and
ª 2006 by the American Academy of Dermatology, Inc. doi:10.1016/j.jaad.2005.10.004
The nonantibiotic properties of tetracyclines are
summarized in and discussed in detail below.
Both laboratory and clinical studies have investi-
gated the anti-inflammatory properties of tetracy-clines. summarizes inhibitory effects oftetracyclines on inflammation.
Tetracyclines and their analogues inhibit matrix
metalloproteinases (MMPs). MMPs are zinc-depen-dent endopeptidases that play an important role inthe remodeling of the connective tissue and areinvolved in embryogenesis, wound healing, rheu-matoid arthritis, and tumor invasion and metasta-sis.There are MMPs that break down fibrillarcollagens known as collagenases (MMP-1, MMP-8,MMP-13) and those that can affect basement mem-brane collagen (collagen IV) known as gelatinases(MMP-2, MMP-9). Tetracycline and its analogues caninhibit both collagenases and gelat
Angiogenesis, the formation of new blood ves-
sels, occurs in many diseases. These include benignconditions (eg, rosacea) and malignant processes(eg, cancer). Matrix-degrading enzymes, present inthe extracellular matrix of tissues, facilitate angio-genesis by allowing new blood vessels to penetrateinto the matrix. MMPs represent one such class ofenzymes involved in this process.
Fig 1. Chemical structures of tetracycline, doxycycline,
Minocycline and doxycycline inhibit angiogenesis
induced by implanted tumors in rabbit cornea.Doxycycline and, to a lesser degree, CMTs inhibitsynthesis of MMPs (MMP-8, MMP-9) by endothelial
specific proteinases) play an important role in the
cells. This inhibition, noted at the protein and mRNA
regulation of mammalian apoptotic cell dea
levels, may affect migration of endothelial cells
Caspase-1, also known as the interleukin 1b (IL-
during angiogenesis.The antiangiogenic effect of
1b)-converting enzyme for its ability to convert the
tetracyclines may have therapeutic implications in
precursor IL-1b into mature IL-1b, is important in
inflammatory processes accompanied by new blood
mediating neuronal cell death after experimental
vessel formation (eg, autoimmune disorders, rosa-
traumatic brain injury in mice. Decreased mature
cea, cancer invasion). Well-controlled studies must
IL-1b production may be correlated with a reduction
be performed, at both the laboratory and clinical
in tissue injury and an improvement in neurological
levels, to investigate this potential.
Recent experimental data indicate that tetracy-
Apoptosis, programmed cell death, is of funda-
neal administration of minocycline 12 hours before or
mental importance for the homeostasis and devel-
30 minutes after traumatic brain injury was shown to
opment of any organism. Disease states such as
prevent neuronal cell death in mice by inhibiting
cancer and neurodegenerative disorders may result
This effect had clinical implications since
from its deregulation. Crucial components of the
it reduced tissue injury and neurological deficits.
apoptotic pathway have been elucidated. A family
Improved neurological function correlated with
of proteases termed caspases (cysteinyl aspartate-
decreased lesion size and decreased capsase-1
Fig 2. Nonantimicrobial properties of tetracycline and its derivatives.
Table I. Inhibitory effects of tetracyclines on
osteoarthritic knees of untreated dogs are signifi-
cantly higher than the levels in doxycycline-treateddogs. This effect is accompanied by inhibition of
proliferation and hypertrophy of chondrocytes and
Recent experimental evidence indicates that min-
ocycline, by stimulating new bone formation, pre-
vents the decrease in mineral density (osteoporosis)
observed in ovariectomized old rats.This model
mimics the accelerated bone loss commonly experi-
enced by postmenopausal women. The effect could
be related to a reduction in osteoclast function by
tetracycline and CMTAdditional well-controlled
studies must be performed to more clearly elucidate
the cellular and molecular mechanisms involved.
Diseases, both dermatologic and nondermato-
logic, that have been investigated for the therapeutic
The mechanisms of action of the tetracyclines and
tetracycline derivatives in the treatment of variousskin diseases discussed in this section are summa-
CMT, Chemically modified tetracycline; DCN, doxycycline; IL-10,
interleukin 10; MCN, minocycline; MMP, matrix metalloproteinase;
Acne. Tetracycline, minocycline, and doxycycline
are effective in the treatment of acne, particularly
activity, as measured by mature IL-1b production.
during the inflammatory stage. It has previously
Minocycline may also have beneficial effects in
been suggested that the beneficial effect of tetracy-
chronic neurodegenerative diseases such as Hun-
cline is due to the inhibition of Propionibacterium
tington diseaseand amyotrophic lateral sclerosis.
acnes accompanied by a reduction in sebum freefatty acids and extracellular lipases.However, it is
currently believed that the inflammatory reaction
Prophylactic administration of doxycycline re-
plays an important role in the pathophysiology of
duces the severity of canine osteoarthritis in the
acne.The exact cascade of events that is respon-
dog anterior cruciate model.Levels of active and
sible for inflammation in acne is not known.
total collagenase activity in extracts of cartilage from
However, there is evidence of chemotaxis of
Table II. Therapeutic use of tetracyclines in
Table III. Mechanisms of action of tetracycline
and tetracycline derivatives in the treatment ofskin disease
inflammatory reaction involving lymphocytes andneutrophils. The mechanism of action may includeinhibition of neutrophil and eosinophil chemotaxis
neutrophils,which are known to store MMP-9.
or inhibition of protease release from granulocytes.
Thus the therapeutic effect of tetracyclines in acne
Tetracycline or minocycline, alone or in combination
may at least in part be due to reduction in neutro-
with nicotinamide, were shown to be effective in
philic chemotaxisas well as their inhibitory effect
bullous dermatoses affecting the dermoepidermal
on proinflammatory cytokines and MMP-9. This
junction, such as bullous pemphigoid, cicatricial
contention is supported by a recent study that
pemphigoid, linear IgA disease, and lichen planus
showed that subantimicrobial-dose doxycycline (20
pemphigoides.These reports are generally un-
mg taken twice daily) reduced the number of both
controlled, and it is possible that a selection bias
inflammatory and noninflammatory lesions in pa-
toward patients with milder disease or spontaneous
tients with moderate facial acne.No detectable
remission may be operative. Additional studies are
also necessary to evaluate whether tetracycline in
combination with nicotinamide is more effective than
Rosacea. Tetracyclines and their analogues are
either of the two drugs administered as monotherapy.
effective in the treatment of rosacea and related
Nevertheless, this therapeutic option represents an
disorders, such as perioral dermatitis, ocular rosacea,
attractive alternative to systemic corticosteroids in the
and steroid-related rosaceaA single daily dose
initial treatment of bullous dermatoses affecting the
of doxycycline may be effective for ocular rosacea.
dermoepidermal junction. While avoiding the poten-
The anti-inflammatory effects of tetracyclines already
tial complications of immunosuppressive agents, the
mentioned may explain, at least in part, their bene-
combination of tetracycline and nicotinamide offers
ficial effects in rosacea. Inhibition of angiogenesis
obvious advantages for older patients who may have
may be a contributory factor in the therapeutic effect
concomitant osteoporosis, diabetes mellitus, or
of tetracyclines in this group of disorders. Features
hypertension. Finally, if the administration of an
that favor angiogenesis may contribute to the telan-
immunosuppressive agent is deemed necessary,
giectasia of rosacea. These include protease-trig-
tetracycline may be administered concomitantly as
gered release of angiogenetic factors stored in the
combination therapy so that the dosage of the
extracellular matrix, release of inhibition of endo-
immunosuppressant may be tapered more rapidly.
thelial factors, and release of angiogenic factors from
Cutaneous sarcoidosis. More recently, the use
of minocycline for the treatment of sarcoidosis was
Bullous dermatoses. Subepidermal bullae are
reported.Minocycline, 200 mg daily for 12 months,
frequently accompanied by splitting or dissolution
was administered to 12 patients. The median follow-
of the basement membrane accompanied by an
demonstrated complete clearing of their lesions,
collagenase activity in synovial fluid and synovial
whereas 2 patients showed a partial response. The
fibroblasts.Oral administration of minocycline in
duration of response ranged from 10 to 41 months.
adjuvant and collagen-induced arthritis in rats re-
No relapse occurred during the 12-month treatment
duced the incidence of arthritisFurthermore,
period. However, maintenance of remission re-
minocycline administration reduced collagenase ac-
quired concomitant administration of corticosteroids
tivity in the synovial fluid derived from patients with
in several of the patients. In addition, a moderately
severe hypersensitivity reaction to minocycline was
There have been several double-blind, placebo-
experienced by one patient in the study.
controlled clinical trials using 200 mg daily of min-
It is interesting to note that tetracyclines, minocy-
ocycline in patients with rheumatoid arthritis.
cline and doxycycline inhibit in vitro granuloma
Kloppenburg et al treated a cohort of 80 patients
formation by monocytes exposed to dextrin beads.
and noted significant improvement in joint tender-
This effect is thought to be due to inhibition of
ness, number of swollen joints, and levels of C-
protein kinase C by tetracycline. These in vitro results
reactive protein. In another study involving 219
provided the rationale for the successful use of
patients with mild to moderate arthritis treated for
minocycline in the treatment of other granulomatous
48 weeks with minocycline, there was alleviation of
dermatoses, such as silicone-induced subcutaneous
joint swelling and tenderness, although the effect
was moderate.A more significant result was noted
Kaposi’s sarcoma. Kaposi’s sarcoma is charac-
in a study involving 60 patients with early (\1 year
terized by proliferation of endothelial cells and
duration) rheumatoid arthritis treated for 2 years with
increase in MMP activity. A preliminary clinical trial
200 mg daily of minocycline versus hydroxychlor-
involved 18 patients with AIDS-related Kaposi’s
sarcoma who were treated with a chemical modified
Scleroderma. In an uncontrolled study, mino-
tetracycline, COL-3.After receiving 25, 50, or 70
cycline 200 mg daily was administered for 12 months
mg/m2 per day for 25 weeks, one patient showed
to 11 patients with early diffuse scleroderma. Four
complete resolution and 7 demonstrated partial
patients showed complete resolution.Confirma-
improvement of skin lesions. The overall response
tion from a larger scale, controlled study would add
rate was 44%, and median time to response was 4
validity to this spectacular response. It would be of
weeks. There was also a reduction in MMP-2 serum
interest to determine whether minocycline specifi-
levels. On the basis of these preliminary data, addi-
cally alters the inflammatory response in sclero-
tional studies investigating the use of COL-3 as
derma. If so, it would be worthwhile to conduct a
monotherapy in patients with early Kaposi’s sarcoma
similar study with localized scleroderma.
and in combination with other therapies in patients
Cancer. Carcinogenesis is a 3-step process in-
with more severe disease seem warranted.
volving tumor cell adhesion, extracellular matrix
Miscellaneous dermatoses. There have been
proteolysis, and cell migration.Degradation of
isolated reports describing the effectiveness of tetra-
basement membrane and its surrounding connective
cyclines in pyoderma gangrenosum,hidradenitis
tissue stroma plays a major role in cancer invasion
and metastasis. MMP-2 and MMP-9 (gelatinases A
drome,a1-antitrypsin deficiency panniculitis,
and B) are frequently expressed in various malignant
and pityriasis lichenoides chrEvaluation of
tumors.Experimental data using various carci-
larger numbers of patients in well-controlled studies
noma cell lines and animal carcinogenesis models
is necessary before any conclusions can be drawn
showed that doxycycline, minocycline, and CMTs
regarding the efficacy of tetracycline and its deriva-
may inhibit tumor growth by inhibiting MMPs and by
tives in the treatment of these conditions.
a direct effect on cell proliferation.Few clinicaltrials investigating the use of tetracyclines in cancer
treatment have been conducted. Recently, a phase I
The immunomodulatory and anti-inflammatory
clinical trial of oral COL-3 (6-demethyl, 6-deoxy, 4-
properties of minocycline suggested that this drug
dedimethylaminotetracycline) was administered to
might be effective in the treatment of autoimmune
35 patients with multiple refractory metastasizing
tumors. Although COL-3 appeared to have stabilized
Rheumatoid arthritis. Rheumatoid arthritis is
nonepithelial-type malignancies, additional follow-
a chronic inflammatory disease affecting about 2 mil-
up studies are necessary to determine its true efficacy
lion Americans. Although the cause of rheumatoid
in the prevention of progression of cancer metastasis
arthritis is not entirely known, it has been shown that
Cardiovascular system. Abdominal aortic an-
joint destruction is at least in part due to enhanced
associated with a life-threatening risk of rupture.
2. Golub LM, Soummalainen K, Sorsa T. Host modulation with
Degradation of aortic wall elastin and collagen
tetracyclines and their chemically modified analogues. CurrOpin Dent 1992;2:80-90.
occurs secondary to local production of several
3. Nelson ML. Chemical and biological dynamics of tetracyclines.
MMPs. Doxycycline inhibits MMP-2 and MMP-9
derived from human vascular cell types and from
4. Shapira LL, Soskolne WA, Houri Y, Barak V, Halabi A, Stabholz
tissue explants from abdominal aortic aneurysms.
A. Protection against endotoxic shock and lipopolysaccharide-
The administration of 200 mg of doxycycline for
induced local inflammation by tetracycline: correlation withinhibition of cytokine secretion. Infect Immun 1996;64:825-8.
7 days before aortic aneurysm surgery resulted in a
5. Golub LM, Lee HM, Ryan ME, Giannobile WV, Payne J, Sorsa T.
3-fold reduction of aortic MMP-2 expression and
Tetracyclines inhibit connective tissue breakdown by multiple
non-antimicrobial mechanisms. Adv Dent Res 1998;12:12-26.
double-blind placebo-controlled pilot study involv-
6. Martin RB. Tetracyclines and daunorubicin in metal ions in
ing 32 patients, the administration of doxycycline
biological systems. In: Sigel H, editor. Antibiotics and theircomplexes. New York: Marcel Dekker; 1985. pp. 19-40.
was associated with a significant reduction in aneu-
7. White JR, Pearce FL. Characterization of chlortetracycline
rysm expansion rates as demonstrated by ultrasound
(aureomycin) as a calcium ionophore. Biochemistry 1982;21:
surveillance.Preliminary data also showed that
doxycycline reduces polymorphonuclear leukocyte
8. Thong YH, Ferrante A. Inhibition of mitogen-induced human
lymphocyte proliferative responses to tetracycline analogues. Clin Exp Immunol 1979;35:443-6.
9. Martin RR, Warr GA, Couch RB, Yeager H, Knight V. Effects of
Periodontitis. Chronic periodontal inflamma-
tetracyclines on leukotaxis. J Infect Dis 1974;129:110-6.
tion is a common cause of irreversible loss of tooth
10. Esterly NB, Furey NL, Flanagan LE. The effect of antimicrobial
attachment. This process involves increased apical
agents on leukocyte chemotaxis. J Invest Dermatol 1978;
proliferation and migration of gingival sulcular epi-
11. Brundula V, Rewcastle NB, Metz LM, Bernard CC, Yong VW.
thelial cells, an increase in periodontal microbial
Targeting leukocyte MMPs and transmigration: minocycline
pathogens, and eventual destruction of collagen in
as a potential therapy for multiple sclerosis. Brain 2002;125:
the gingival, periodontal ligament, and alveolar bone.
The source of the proteolytic enzymes is the gingival
12. Plewig G, Schopf E. Anti-inflammatory effects of antimicrobial
epithelial sulcular epithelium (MMP-2, -7, -8, -13,
agents. An in vivo study. J Invest Dermatol 1975;65:532-6.
13. Kloppenburg M, Breedveld FC, Terwiel J, Mallee C, Dijkmans
-14)and from periodontal pathogens.Early stud-
BAC. Minocycline in active rheumatoid arthritis: a double
ies showed that tetracycline, doxycycline, and min-
blind, placebo-controlled trial. Arthritis Rheum 1994;37:
ocycline inhibit collagenase of gingival crevicular
fluid derived from adult periodontitis.The oral
14. Pruzanski W, Greenwald RA, Street IP, Laliberte F, Stefanski E,
administration of submicrobial dose of doxycycline
Vadas P. Inhibition of enzymatic activity of phospholipaseA
(20 mg twice daily) as an adjuvant for conventional
by minocycline and doxycycline. Biochem Pharmacol
procedures for adult periodontitis resulted in a sig-
15. Ritchlin CT, Haas-Smith SA, Schwarz EM. Minocycline but not
nificant improvement in tooth attachment as well as
doxycycline upregulates IL-10 production in human synovio-
reduction of pocket depth and bleeding after prob-
cytes, mononuclear cells and synovial explants. Arthritis
More recently, local delivery of doxycycline
16. Amin AR, Attur MG, Thakker GD, Patel PD, Vyas PR, Patel RN,
showed similar effects in chronic periodontitis.
et al. A novel mechanism of action of tetracyclines: effects ofnitric oxide synthases. Proc Nat Acad Sci U S A 1996;93:14014-9.
17. Amin AR, Patel RN, Thakker GD, Lowenstein CJ, Attur MG,
Tetracycline and its analogues have been used in
Abramson SB. Post-transcriptional regulation of induciblenitric oxide synthase mRNA in murine macrophages by
the treatment of various dermatologic and non-
doxycycline and chemically modified tetracyclines. FEBS Lett
dermatologic diseases. Although there is some
evidence for anti-inflammatory and immunomodu-
18. Stetler-Steveson WG, Liotta LA, Kleiner DE. Extracellular matrix
latory effects, additional studies must be performed,
6: role of matrix metalloproteinases in tumor invasion and
at both the laboratory and clinical levels, to corrob-
19. Golub LM, Lee HM, Lehrer G, Nemiroff A, McNamara TF, Kaplan
R, et al. Minocycline reduces gingival collagenolytic activity
We thank David Feman for assistance with the prep-
during diabetes: preliminary observations and a proposednew mechanism of action. J Periodont Res 1983;18:516-26.
20. Golub LM, Ramamurthy NS, McNamara TF, Greenwald RA,
Rifkin BR. Tetracyclines inhibit connective tissue breakdown:
new therapeutic implications for an old family of drugs. Crit
1. Stephens CR, Conover LH, Pasternak R, Hochstein FA, More-
land WT, Regna PP, et al. The structure of aureomycin. J Am
21. Tamargo RJ, Bok RA, Brem H. Angiogenesis inhibition by
minocycline. Cancer Res 1991;51:672-5.
22. Hanemaaijer R, Visser H, Koolwijk P, Sorsa T, Salo T, Golub LM,
40. Jansen T, Plewig G. Rosacea: classification and treatment.
et al. Inhibition of MMP synthesis by doxycycline and chem-
ically modified tetracyclines (CMTs) in human endothelial cells.
41. Frucht-Pery J, Chayet AS, Feldman ST, Lin S, Brown SJ. The
effect of doxycycline on ocular rosacea. Am J Ophthalmol
23. Fink KB, Andrews LJ, Butler WE, Ona VO, Li M, Bogdanov M,
et al. Reduction of post-traumatic brain injury and free radical
42. Wilkin JK. Rosacea—pathophysiology and treatment. Arch
production by inhibition of the caspase-1 cascade. Neurosci-
43. Beck MA, Lorincz AL. The treatment of bullous pemphigoid
24. Friedlander RM, Gagliardini V, Hara H, Fink KB, Li W,
successfully controlled by tetracycline and nicotinamide.
MacDonald G, et al. Expression of a dominant negative mutant
A preliminary report. Arch Dermatol 1986;122:670-4.
of interleukin-1 beta converting enzyme in transgenic mice
44. Peoples D, Fivenson DP. Linear IgA bullous dermatosis:
prevents neuronal cell death induced by trophic factor
successful treatment with tetracyclines and nicotinamide.
withdrawal and ischemic brain injury. J Exp Med 1997;185:
45. Chaffins ML, Collison D, Fivenson DP. Treatment of pemphigus
25. Li M, Ona VO, Chen M, Kaul M, Tenneti L, Zhang X, et al.
and linear IgA dermatosis with nicotinamide and tetracycline:
Functional role and therapeutic implications of neuronal
a review of 13 cases. J Am Acad Dermatol 1993;28:998-1000.
caspase-1 and -3 in a mouse model of traumatic spinal cord
46. Fivenson D, Breneman D, Rosen GB, Hersh CS, Cardone S,
injury. Neuroscience 2000;99:333-42.
Mutasim D. Nicotinamide and tetracycline therapy of bullous
26. Yrjanheikki J, Keinanen R, Pellikka M, Hokfelt T, Koistinaho J.
pemphigoid. Arch Dermatol 1994;130:753-8.
Tetracyclines inhibit microglial activation and are neuropro-
47. Poskitt L, Wojnarowska F. Minimizing cicatricial pemphigoid
tective in global brain ischemia. Proc Natl Acad Sci U S A
orodynia with minocycline. Br J Dermatol 1995;132:784-9.
48. Kolbach DN, Remme JJ, Bos WH, Jonkman MF, De Jong MCJM,
27. Yrjanheikki J, Tikka T, Keinanen R, Goldstein G, Chan PH,
Pas HH, et al. Bullous pemphigoid successfully controlled by
Koistinaho J. A tetracycline derivative, minocycline, reduces
tetracycline and nicotinamide. Br J Dermatol 1995;133:88-90.
inflammation and protects against focal cerebral ischemia
49. Fivenson DP, Kimbrough TL. Lichen planus pemphigoides:
with a wide therapeutic window. Proc Natl Acad Sci U S A
combination therapy with tetracycline and nicotinamide. J Am
28. Sanchez Mejia RO, Ona VO, Li M, Friedlander RM. Minocycline
50. Yomoda M, Komai A, Hashimoto T. Sublamina densa-type
reduces traumatic brain injury-mediated caspase-1 activation,
linear IgA bullous dermatosis successfully treated with oral
tissue damage, and neurological dysfunction. Neurosurgery
tetracycline and niacinamide. Br J Dermatol 1999;141:608-9.
51. Wojnarowska F, Kirtschig G, Khumalo N. Treatment of sub-
29. Chen M, On VO, Mingwei L, Ferrante RJ, Fink KB, Zhu S, et al.
epidermal immunobullous diseases. Clin Dermatol 2001;19:
Minocycline inhibits caspase-1 and caspase-3 expression and
delays mortality in a transgenic mouse model of Huntington
52. Loo WJ, Kirtschig G, Wojnarowska F. Minocycline as a thera-
peutic option in bullous pemphigoid. Clin Exp Dermatol 2001;
30. Zhu S, Stavrovskaya IG, Drozda M, Kim BYS, Ona V, Mingwei LI,
et al. Minocycline inhibits cytochrome c release and delays
53. Chaidemenos GCh. Tetracycline and niacinamide in the treat-
progression of amyotrophic lateral sclerosis in mice. Nature
ment of blistering skin diseases. Clin Dermatol 2001;19:
31. Yu LP, Smith GN, Brandt KD, Myers SL, O’Connor BL, Brandt
54. Bachelez H, Senet P, Candranel J, Kaoukhov A, Dubertret L.
DA. Reduction of the severity of canine osteoarthritis by
The use of tetracyclines for the treatment of sarcoidosis. Arch
prophylactic treatment with oral doxycycline. Arthritis Rheum
55. Webster GF, Toso SM, Hegemann L. Inhibition of a model of in
32. Williams S, Wakisaka A, Zeng QQ, Barnes J, Seyedin S, Martin G,
vitro granuloma formation by tetracyclines and ciprofloxacin.
et al. Effect of minocycline on osteoporosis. Adv Dent Res
56. Senet P, Bachelez H, Ollivaud L, Vignon-Pennamen D, Duber-
33. Ryan ME, Greenwald RA, Golub LM. Potential of tetracycline
tret L. Minocycline for the treatment of cutaneous silicone
to modify cartilage breakdown in osteoarthritis. Curr Opin
granulomas. Br J Dermatol 1999;140:985-7.
57. Veller Fornasa C, Catalano P, Peserico A. Minocycline in
34. Vernillo AT, Rifkin BR. Effects of tetracyclines on bone metab-
granulomatous cheilitis: experience with 6 cases. Dermatology
35. Plewig G, Kligman AM. Acne and rosacea. 2nd ed. Berlin:
58. Cianfrocca M, Cooley TP, Lee JY, Rudek MA, Scadden DT,
Ratner L, et al. Matrix metalloproteinase inhibitor COL-3 in
36. Del Rosso J. A status report on the use of subantimicrobial-
the treatment of AIDS-related Kaposi’s sarcoma: a phase I
dose doxycycline. A review of the biologic and antimicrobial
AIDS malignancy consortium study. J Clin Oncol 2002;20:
effects of the tetracyclines. Cutis 2004;74:118-22.
37. Esterly NB, Koransky JS, Furey NL, Trevisan M. Neutrophil
59. Berth-Jones J, Tan SV, Graham-Brown RAC, Pembroke AC. The
chemotaxis in patients with acne receiving oral tetracycline
successful use of minocycline in pyoderma gangrenosum-a
therapy. Arch Dermatol 1984;120:1308-13.
report of seven cases and review of the literature. J Dermatol
38. Skidmore R, Kovach R, Walker C, Thomas J, Bradshaw M,
Leyden J, et al. Effects of subantimicrobial-dose doxycycline
60. Jemec GB, Wendelboe P. Topical clindamycin versus systemic
in the treatment of moderate acne. Arch Dermatol 2003;139:
tetracycline in hidradenitis suppurativa. J Am Acad Dermatol
39. Macdonald A, Feiwel M. Perioral dermatitis: aetiology and
61. Vignon-Pennamen MD, Wallach D. Cutaneous manifestations
treatment with tetracycline. Br J Dermatol 1972;87:315-9.
of neutrophilic disease. Dermatologica 1991;183:255-64.
62. Joshi RK, Atukorala DN, Abanmi A, al Khamis O, Haleem A.
metastasis by an oral non-antimicrobial tetracycline analog
Successful treatment of Sweet’s syndrome with doxycycline.
(COL-3) in a metastatic prostate cancel model. Int J Cancer
63. Humbert P, Faivre B, Gibey R, Agache P. Use of anti-collagenase
75. Rubins JB, Charboneau D, Alter MD, Bitterman PB, Kratzke RA.
properties of doxycycline in treatment of alpha 1-antitrypsin
Inhibition of mesothelioma cell growth in vitro by doxycycline.
deficiency panniculitis. Acta Derm Venereol 1991;71:189-94.
64. Piamphongsan TT. Tetracycline for the treatment of pityriasis
76. Rudek MA, Figg WD, Dyer V, Dahut W, Turner ML, Seth M, et al.
lichenoides. Br J Dermatol 1974;91:319-22.
Phase I clinical trail of oral COL-3, a matrix metalloproteinase
65. Hanemaaijer R, Sorsa T, Konttinen YT, Ding Y, Sutinen M, Visser
inhibitor in patients with refractory metastatic cancer. J Clin
H, et al. Matrix metalloproteinase-8 is expressed in rheumatoid
synovial fibroblasts and endothelial cells. Regulation by tumor
77. Thompson RW, Baxter BT. MMP inhibition in abdominal aortic
necrosis factor-a and doxycycline. J Biol Chem 1997;272:
aneurysms. Ann N Y Acad Sci 1999;878:159-78.
78. Mosorin M, Juvonen J, Biancari F, Satta J, Surcel HM, Leinonen
66. Sewell KL, Breedveld F, Furrie E, O’Brien J, Brinckerhoff C,
M, et al. Use of doxycycline to decrease the growth rate of
Dynesius-Trentham R, et al. The effect of minocycline in rat
abdominal aortic aneurysms: a randomized double-blind,
models of inflammatory arthritis: correlation of arthritis sup-
placebo-controlled pilot study. J Vasc Surg 2001;34:757-8.
pression with enhanced T-cell calcium flux. Cell Immunol
79. Takeshita S, Ono Y, Kozuma K, Suzuki M, Kawamura Y,
Yokoyama T, et al. Modulation of oxidative burst of neutro-
67. Kloppenburg M, Verweij CL, Miltenburg AMM, Verhoeven AJ,
phils by doxycycline in patients with acute myocardial infarc-
Daha MR, Dijkmans BAC, et al. The influence of tetracyclines
tion. J Antimicrob Chemother 2002;49:411-3.
on T cell activation. Clin Exp Immunol 1995;102:635-41.
80. Tervahartiala T, Pirila E, Ceponis A, Maisi P, Salo T, Tuter G,
68. Tilley BC, Alarcon GS, Heyse SP, Trentham DE, Neuner R,
et al. The in vivo expression of the collagenolytic matrix
Kaplan DA, et al. Trial Group. Minocycline in rheumatoid
metalloproteinase (MMP-2, -8, -13 and -14) and matrilysin
arthritis: a 48 week double-blind placebo controlled trial. Ann
(MMP-7) in adult and localized juvenile periodontitis. J Dent
69. O’Dell JR, Blakely KW, Mallek JA, Eckhoff PJ, Leff RD, Wees SJ,
81. Grenier D, Plamondon P, Sorsa T, Lee HM, McNamara T,
et al. Treatment of early seropositive rheumatoid arthritis:
Ramamurthy NS, et al. Inhibition of proteolytic serpinolytic
a two-year double-blind comparison of minocycline and
and progelatinase-b activation activities of periodontopath-
hydroxychloroquine. Arthritis Rheum 2001;44:2235-41.
ogens by doxycycline and the non-antimicrobial chemically
70. Le CH, Morales A, Trentham DE. Minocycline in early diffuse
modified tetracycline derivatives. J Periodontol 2002;73:79-85.
scleroderma. Lancet 1998;352:1755-6.
82. Golub LM, Ramamurthy NS, McNamara TF, Gomes BC, Wolff
71. Westermarck J, Kahari V-M. Regulation of matrix metallopro-
MS, Casino A. Tetracyclines inhibit tissue collagenase activity:
teinase expression in tumor invasion. FASEB J 1999;13:781-92.
a new mechanism in the treatment of periodontal disease.
72. Duivenvoorden WC, Hirte HW, Singh G. Use of tetracycline as
an inhibitor of matrix metalloproteinase activity secreted by
83. Ciancio S, Ashley R. Safety and efficacy of sub-antimicrobial
human bone-metastasizing cancer cells. Invasion Metastasis
dose doxycycline therapy in patients with adult periodontitis.
73. Hidalgo M, Eckhardt SG. Development of matrix metallopro-
84. Wennstrom JL, Newman HN, MacNeill SR, Killoy WJ, Griffiths
teinase inhibitors in cancer therapy. J Natl Cancer Inst 2001;
GS, Gillam DG, et al. Utilization of locally delivered doxycycline
in non-surgical treatment of chronic adult periodontitis:
74. Lokeshwar BL, Selzer MG, Zhu BQ, Block NL, Golub LM.
a comparative multi-center trial of 2 treatment approaches.
Inhibition of cell proliferation, invasion, tumor growth and
8. Modelos experimentais em pesquisa1 Lydia Masako Ferreira2, Bernardo Hochman3, Marcus Vinícius Jardini Barbosa4 1. Trabalho desenvolvido no Programa de Pós-Graduação em Cirurgia Plástica da Universidade Federal de São Paulo – Escola Paulista de2. Professora Titular da Disciplina de Cirurgia Plástica e Coordenadora do Programa de Pós-Graduação em Cirurgia Plástica da UNIFESP �
 The nonantibiotic properties of tetracyclines are
summarized in and discussed in detail below.
The nonantibiotic properties of tetracyclines are
summarized in and discussed in detail below.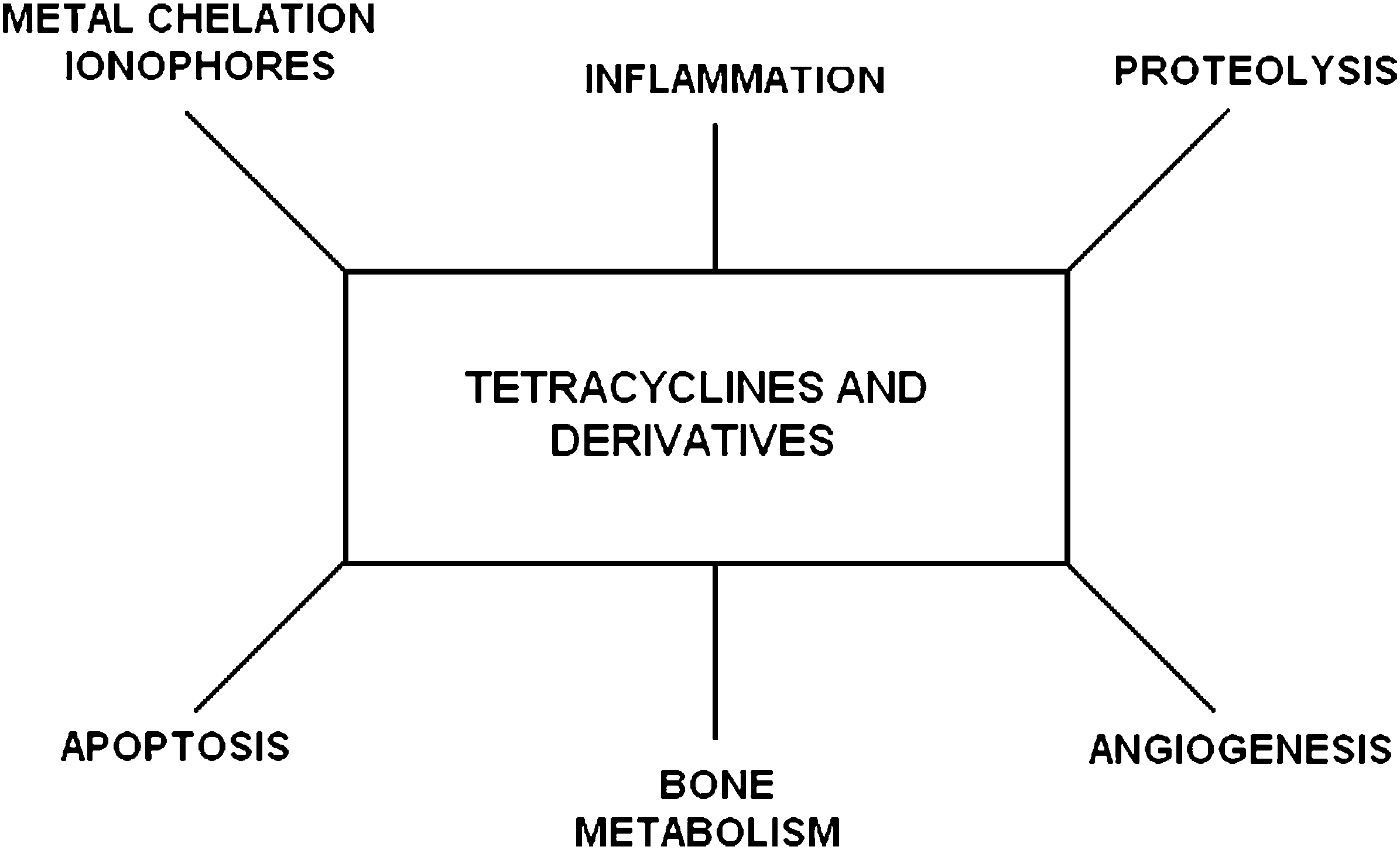 Fig 2. Nonantimicrobial properties of tetracycline and its derivatives.
Fig 2. Nonantimicrobial properties of tetracycline and its derivatives. 62. Joshi RK, Atukorala DN, Abanmi A, al Khamis O, Haleem A.
62. Joshi RK, Atukorala DN, Abanmi A, al Khamis O, Haleem A.