20. Nisbet AP, Foster OJ, Kingsbury A, Eve DJ, Daniel SE, Marsden
40. Berkowitz BA. The relationship of pharmokinetics to pharmaco-
CD, Lees AJ. Preproenkephalin and preprotachykinin messenger
logical activity, morphine, methadone and naloxone. Clin Pharma-
RNA expression in normal human basal ganglia and in Parkinson’s
disease. Neuroscience 1995;66:361–376.
41. Ngai SH, Berkowitz BA, Yang JC, Hempstead J, Spector S. Pharma-
21. Calon F, Birdi S, Rajput AH, Hornykiewicz O, Bedard PJ, Di PT.
cokinetics of naloxone in rats and in man: basis for its potency and
Increase of preproenkephalin mRNA levels in the putamen of
short duration of action. Anesthesiology 1976;44:398 – 401.
Parkinson disease patients with levodopa-induced dyskinesias.
42. Manson AJ, Schrag A, Lees AJ. Low-dose olanzapine for levodopa
J Neuropathol Exp Neurol 2002;61:186 –196.
induced dyskinesias. Neurology 2000;55:795–799.
22. Piccini P, Weeks RA, Brooks DJ. Alterations in opioid receptor
43. Sieradzan KA, Fox SH, Hill M, Dick J, Crossman AR, Brotchie
binding in Parkinson’s disease patients with levodopa-induced
JM. Cannabinoids reduce levodopa-induced dyskinesia in Parkin-
dyskinesia. Ann Neurol 1997;42:720 –726.
son’s disease: a pilot study. Neurology 2001;57:2108 –2111.
23. Henry B, Fox SH, Crossman AR, Brotchie JM. - and ␦-Opioid
44. Rascol O, Nutt JG, Blin O, et al. Induction by dopamine D1
receptor antagonists reduce levodopa-induced dyskinesia in the
receptor agonist ABT-431 of dyskinesia similar to levodopa in
MPTP-lesioned primate model of Parkinson’s disease. Exp Neurol
patients with Parkinson disease. Arch Neurol 2001;58:249 –254.
45. Rascol O, Arnulf I, Peyro-Saint Paul H, et al. Idazoxan, an alpha-2
24. Klintenberg R, Svenningsson P, Gunne L, Andre´n PE. Naloxone
antagonist, and L-DOPA-induced dyskinesias in patients with Par-
reduces levodopa-induced dyskinesias and apomorphine-induced
kinson’s disease. Mov Disord 2001;16:708 –713.
rotations in primate models of parkinsonism. J Neural Transm
46. Verhagen Metman L, Del Dotto P, Natte´ R, van den Munckhof
P, Chase TN. Dextromethorphan improves levodopa-induced
25. Gomez-Mancilla B, Bedard PJ. Effect of nondopaminergic drugs
dyskinesias in Parkinson’s disease. Neurology 1998;51:203–
on L-DOPA-induced dyskinesias in MPTP-treated monkeys. Clin
47. Verhagen Metman L, Del Dotto P, van den Munckhof P, Fang J,
26. Trabucchi M, Bassi S, Frattola L. Effects of naloxone on the
Mouradian MM, Chase TN. Amantadine as treatment for dyski-
“on-off” syndrome in patients receiving long-term levodopa ther-
nesias and motor fluctuations in Parkinson’s disease. Neurology
apy. Arch Neurol 1982;39:120 –121.
27. Sandyk R, Snider SR. Naloxone treatment of L-dopa-induced
48. Strong JA, Dalvi A, Samaha FJ, Gong J, Xu K, Yue X, Yu L. Mu
dyskinesias in Parkinson’s disease. Am J Psychiatry 1986;143:118.
opioid receptor polymorphisms and L-Dopa induced dyskinesia inParkinson’s disease. Proc Soc Neurosci 1999;25:846.2.
28. Price P, Baxter RC, Parkes JD, Marsden CD. Opiate antagonists
and Parkinson’s disease. Arch Neurol 1979;36:661.
29. Nutt JG, Rosin AJ, Eisler T, Calne DB, Chase TN. Effect of an opiate
antagonist on movement disorders. Arch Neurol 1978;35:810 – 811.
30. Rascol O, Fabre N, Blin O, et al. Naltrexone, an opiate antagonists,
fails to modify motor symptoms in patients with Parkinson’s
disease. Mov Disord 1994;9:437– 440.
31. Manson AJ, Katzenschlager R, Hobart J, Lees AJ. High dose
naltrexone for dyskinesias induced by levodopa. J Neurol Neuro-surg Psychiatry 2001;70:554 –556.
Stuart J. Fellows, PhD,* and Johannes Noth, MD
32. Delitala G, Giusti M, Mazzocchi G, Granziera L, Tarditi W,
Giordano G. Participation of endogenous opiates in regulation of
Neurologische Klinik, Universita¨tsklinikum
the hypothalamic-pituitary-testicular axis in normal men. J Clin
Endocrinol Metab 1983;57:1277–1281.
33. Bonuccelli U, Piccini P, Del Dotto P, Rossi G, Corsini GU,
Muratorio A. Naloxone partly counteracts apomorphine side ef-
Abstract: In recent years it has been shown that a variety of
fects. Clin Neuropharmacol 1991;14:442– 449. movement disorders are associated with abnormalities of
34. Limone P, Calvelli P, Altare F, Ajmone-Catt P, Lima T, Molinatti
the fine motor control of the hand. In Parkinson’s disease
GM. Evidence of an interaction between alpha-MSH and opioids
(PD), these changes consist of a slowing of the rate of grip
in the regulation of gonadotropin secretion in man. J Endocrinol
force development and the use of abnormally large grip forces both during lifting and static holding of an object. It
35. Coiro V, Volpi R, Capretti L, et al. Different effects of naloxone on
has been suggested, however, that these changes are a direct
the growth hormone response to melatonin and pyridostigmine in
effect of the patient’s levodopa medication or associated
normal men. Metabolism 1998;47:814 – 816. with levodopa induced dyskinesias. Accordingly, we exam-
36. Tomasi PA, Fanciulli G, Palermo M, Pala A, Demontis MA,
ined the performance of de novo Parkinson patients in a
Delitala G. Opioid receptor blockade blunts growth hormone (GH)
precision lifting task. All patients (n ؍ 6) were newly diag-
secretion induced by GH-releasing hormone in the male. HormMetab Res 1998;30:34 –36. nosed and showed rigidity, bradykinesia, or both, but were
37. Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical
unaffected by tremor or dyskinesia. None of the patients
diagnosis of idiopathic Parkinson’s disease: a clinico-patholog-ical study of 100 cases. J Neurol Neurosurg Psychiatry 1992;55:181–184.
*Correspondence to: Dr. Stuart Fellows, Neurologishe Klinik, Uni-
38. Langston JW, Widner H, Goetz CG, Brooks D, Fahn S, Freeman
versita¨tsklinikum der RWTH Aachen, Pauwelsstr. 30, D-52074
T, Watts R. Core assessment program for intracerebral transplan-
Aachen, Germany. E-mail: [email protected]
tations (CAPIT). Mov Disord 1992;7:2–13.
Received 1 August 2003; Revised 25 September 2003; Accepted 13
39. Evans JM, Hogg MI, Lunn JN, Rosen M. Degree and duration of
reversal by naloxone of effects of morphine in conscious subjects. Published online 18 December 2003 in Wiley InterScience (www. interscience.wiley.com). DOI: 10.1002/mds.10710 Movement Disorders, Vol. 19, No. 5, 2003GRIP FORCE ABNORMALITIES IN DE NOVO PDhad received antiparkinson medication. Grip force was TABLE 1. Clinical details of the patients abnormally high in both the lifting and hold phases. This exaggeration was equal in magnitude to that observed pre- viously in medicated patients. Thus we conclude that the abnormalities in grip force observed here are intrinsic fea- tures of PD and not the result of dopamine medication or its side effects. 2003 Movement Disorder Society Key words: Parkinson’s disease; de novo; precision grip
In recent years it has been shown that a variety of
Stage 0, no signs of disease; Stage 1, unilateral disease; Stage 1.5,
unilateral plus axial involvement; Stage 2, bilateral disease without
movement disorders are associated with abnormalities of
impairment of balance; Stage 2.5, mild bilateral disease with recovery
fine motor control of the hand.1–7 In Parkinson’s disease
on pull test; Stage 3, mild to moderate bilateral disease, some postural
(PD), these changes consist of a slowing of the rate of
instability, physically independent; Stage 4, severe disability, still ablewalk or stand unassisted; Stage 5, wheelchair-bound or bedridden
grip force development8 and the use of abnormally large
grip forces, during both lifting and static holding of an
object.9,10 It has been suggested, however, that thesechanges were a direct effect of the patient’s levodopa(L-dopa) medication.11 This claim is somewhat surpris-
Details of the apparatus and methods employed have
ing, given the improved quality of movement generally
been fully described elsewhere.9 Briefly, the investiga-
reported by the patients themselves, and indeed, L-dopa
tion was carried out in a quiet room with subdued light-
medication has been shown to markedly improve reach-
ing. The subject was seated in a stable chair that sup-
to-grasp movements in patients with PD.12 A more likely
ported the back (but not the head) before a table on which
suggestion was that the exaggerated grip force levels
was situated the lifting device. Subjects were positioned
resulted from L-dopa induced dyskinesias.13 Accord-
so that they were able to grip the object between their
ingly, we examined the performance of de novo Parkin-
forefinger and thumb and lift and hold the object at the
son patients in a precision lifting task. These patients
wrist while their elbow remained fully supported on a
were in the early stages of the disease and did not exhibit
padded rest. The measuring instruments built into the
tremor or dyskinesia as part of their symptoms. They had
device registered the grip force exerted on the object
had no exposure to L-dopa or other dopaminergic medi-
(9301b; Kistler, Winterhur, Switzerland) and its vertical
cation, and so their performance clearly could not be
position (T60500; VAC, Mu¨nchen, Germany). These
influenced, directly or indirectly, by effects of
signals were amplified and then passed to the analogue-
We show that they demonstrated grip force abnormalities
to-digital converter board (NI-PCI-MIO-16XE; National
compatible with those of a group of parkinsonian pa-
Instruments, Austin, TX) of a laboratory computer
(Macintosh PPC 7600/132; Apple, Cupertino, CA) sam-
abnormalities are an intrinsic feature of the pathophysi-
ology of PD. An alternative explanation for these deficits
The subjects were required, without visual feedback
concerning hand position, to grip and lift the object 4 to6 cm above the table, then hold it steady for 6 to 8seconds before replacing the object on the table and
SUBJECTS AND METHODS
releasing it. The contact pads on the object for thumb and
The study involved 6 patients who were referred to our
forefinger were covered with sandpaper (extra-fine, corn
outpatient clinic with a suspected and subsequently con-
400). A second laboratory computer (Macintosh IIVX;
firmed diagnosis of PD (Table 1). In cases of hemipar-
Apple) was used to control the load of the object via a
kinsonism, the affected hand was studied, whereas in the
servo-device. A torque motor attached via a nonelastic
other cases the dominant hand was used. None of the
band to the object was used to alter object load between
patients was receiving or had received parkinsonian
lifts without the subject’s knowledge in a pseudo-random
medication. A control group comprised 12 age-matched
manner between two levels, namely 3.3 N (light) and 7.8
subjects (6 men, 6 women; mean age, 61 Ϯ 3 years) with
N (heavy), such that five lifts could be selected for each
no history of neurological disorder. All subjects gave
load where the load remained unaltered from the preced-
their informed consent to the procedures, which had been
ing lift. A 10- to 15-second pause was allowed between
approved previously by the local ethics committee. Movement Disorders, Vol. 19, No. 5, 2003
status and object load as the main factors. Post-hoctesting was carried out using the Tukey-Kramer test.
All 6 de novo PD patients displayed obvious abnor-
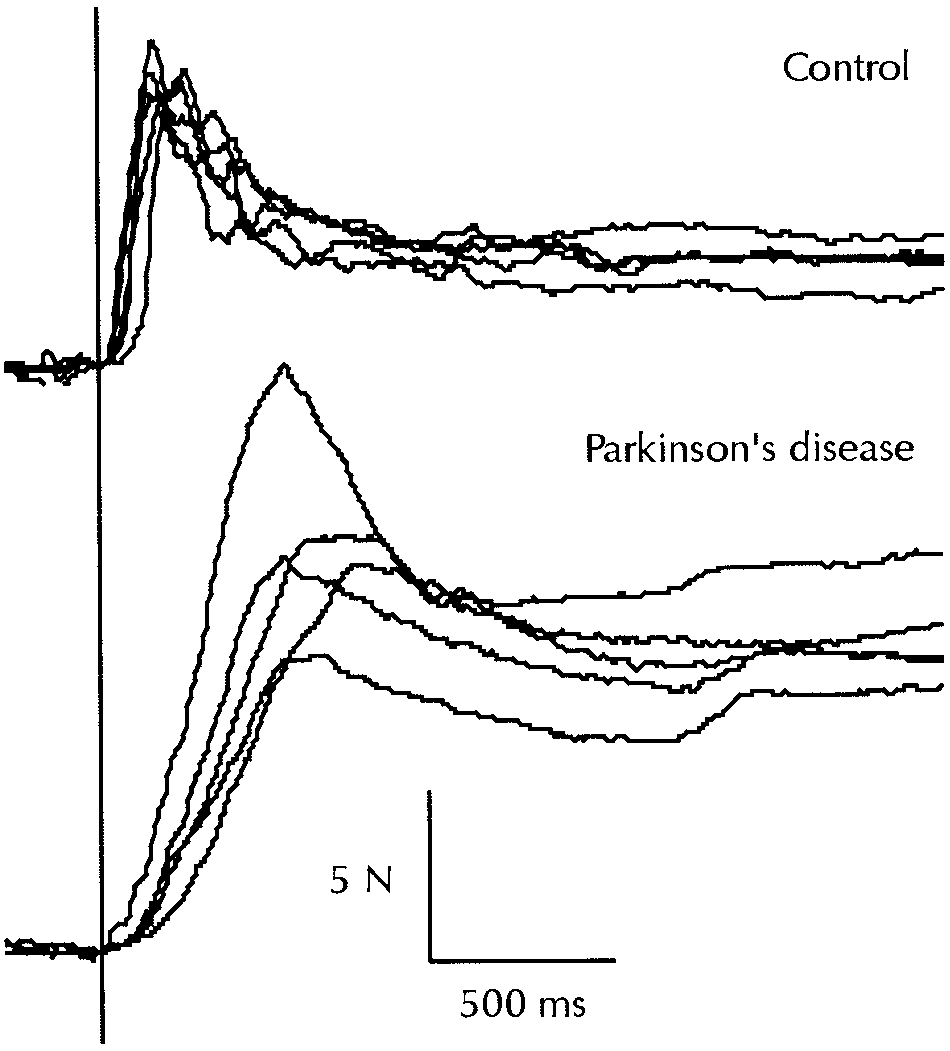
malities in their grip force curves. Figure 2 shows 5 gripforce profiles obtained while lifting a light load for arepresentative control subject (upper traces) and a patientwith PD (lower traces). It is apparent that the patientdeveloped grip force markedly slower than did the con-trol subject, and consistently employed exaggerated lev-els of grip force, in both the dynamic and static phases ofthe lift.
The group values for the four lifting parameters are
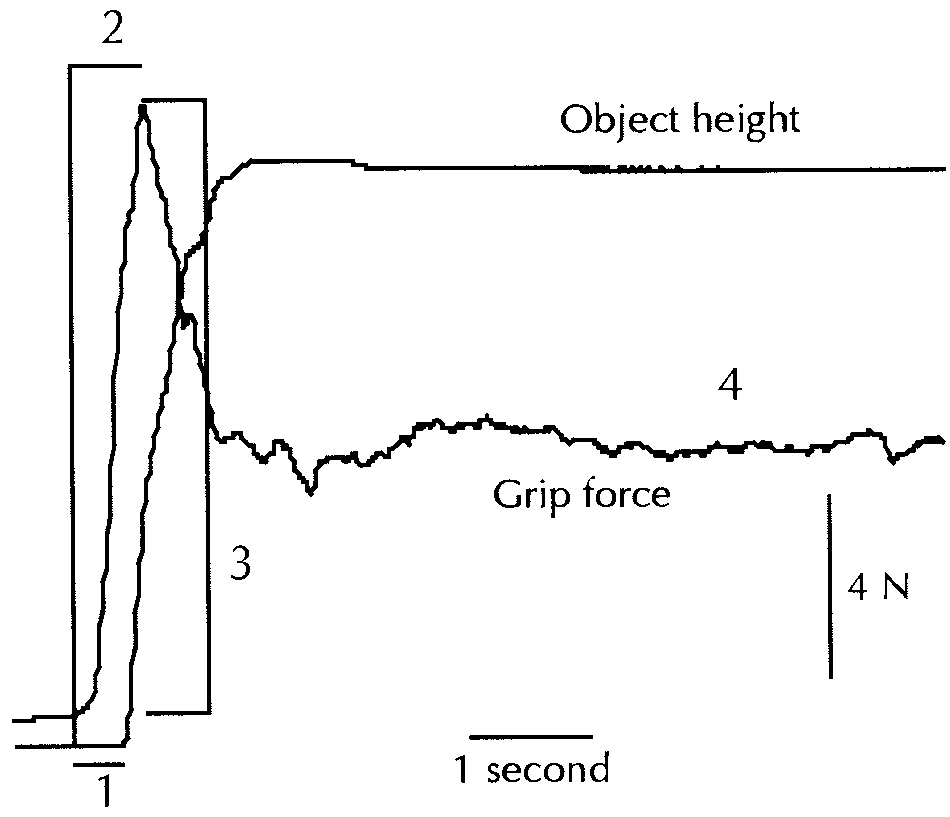
displayed in Figure 3. Each dot represents the value of asingle parkinsonian patient, whereas the grey boxes rep-resent the mean value for the control group (ϮSEM). FIG. 1. The grip force and object position curves for a typical control
The mean values for the patients with PD are shown as
subject lifting the light load. The parameters obtained from these curves
filled triangles. Figure 3A shows the data for the IGL. It
are numbered. 1, Time between onset of grip force development and object lift-off (IGL), a measure of finger/wrist co-ordination; 2, time
may be seen that the parkinsonian patients all demon-
taken to achieve peak grip force (TPGF), a measure of the rate for grip
strated timings outside or at the upper end of the range of
force development; 3, peak grip force (PGF) developed in the dynamic
values shown by the control group. On a group basis, this
lifting phase, a measure of pre-planned matching of grip force to object properties; and 4, static grip force (SGF), the grip force developed
prolongation was highly significant (P Ͻ 0.01) and its
while holding the object steady above the table, a measure of grip force
magnitude was comparable with that observed in an
adaptation to actual conditions based on cutaneous afferent feedback.
The grip force curves obtained from each of the lifts
carried out was measured subsequently (see Fig. 1) toyield a series of parameters: (1) IGL, the time betweenthe onset of grip force and the lift-off of the object(msec); (2) TPGF, the time taken to reach the peak gripforce (msec); (3) PGF, peak grip force magnitude (N);and (4) SGF, the stable grip force adopted while holdingthe object steady above the table (N). The IGL may beconsidered to provide a measure of the co-ordinationbetween the fingers gripping the object and more prox-imal arm muscles responsible for the actual horizontallift of the object. TPGF provides information about therate of grip force development at the fingers. PGF pro-vides information on the largely automatic processes ofthe selection from memory of motor sets matched toobject properties,14 whereas the SGF is the result ofmodification of these stored commands by actual sensoryfeedback concerning object properties obtained duringthe lift itself.15
Statistical analysis was carried out using the Statview5.0 package (SAS Institute, Cary, NC). For this purpose,
FIG. 2. The 5 grip force profiles obtained while lifting the light load
the median value obtained from five lifts with a given
by a typical control subject (upper traces) and a patient with PD (4,lower traces). Grip force development clearly was slower in the patient,
load were obtained for each parameter and compared
who also developed consistently excessive force levels during both the
between subjects using MANOVA analysis with clinical
dynamic lifting phase and the static hold phase. Movement Disorders, Vol. 19, No. 5, 2003GRIP FORCE ABNORMALITIES IN DE NOVO PDFIG. 3. Group values for the four lifting pa- rameters. Each dot represents the value of a single parkinsonian patient, whereas grey boxes represent the mean value for the control group (ϮSEM). The parkinsonian mean is represented by a filled triangle. All four parameters showed a significant increase over control values in PD (P Ͻ 0.01, except TPGF, P Ͻ 0.05). The adap- tation of the values according to load seen in the control group was maintained in PD, with the exception of TPGF (IGL, P Ͻ 0.05; PGF, SGF, P Ͻ 0.01). The percentage values under each load give the increase in the parkinsonian mean relative to the control mean. Abnormalities are more evident with the lighter load, and grip force is exaggerated especially in the static holding phase.
earlier study9 involving patients at a later stage of the
grip force to load was retained (P Ͻ 0.01). It is interest-
disease who were on a stable regime of L-dopa medication.
ing to note that the exaggeration was more marked for
IGL modulation with load remained significant (P Ͻ 0.05)
the light load (on average, twice the mean level of the
in the parkinsonian patients. The relative increase over
control group) than for the heavy load (on average, an
control values (ϳ60%) was equal for both loads.
increase of two-thirds). The exaggeration was also more
TPGF values for the parkinsonian patients (Fig. 3B)
marked than that observed previously in the patients with
were also prolonged relative to the control group (P Ͻ
a longer duration of disease,9 although the fact that the
0.05). This prolongation was less marked, however, than
latter were receiving L-dopa medication must be borne in
that observed previously in patients with a longer disease
mind. Figure 3D shows the data for SGF and it can be
duration.9 The modulation of timing with load observed
seen that a significant exaggeration of grip force levels in
in the latter group of patients and in the control group
de novo PD patients occurred (P Ͻ 0.01), even more
was not significant in the group of de novo patients.
marked than in the dynamic phase of the lift, particularly
The most pronounced abnormalities shown by the de
for the light load, where the exaggeration over control
novo patients were observed in the exaggerated levels of
values was (in relative terms) almost twice as great as
grip force employed in both the dynamic and static
that observed with the heavy load. Scaling of grip force
phases of the lift. PGF values (Fig. 3C) for patients were
to load was retained (P Ͻ 0.01). Once again, the exag-
significantly higher than control values (P Ͻ 0.01) for
geration was more marked than that observed previously
both the light and the heavy load, although the scaling of
in patients with a longer duration of disease.9
Movement Disorders, Vol. 19, No. 5, 2003DISCUSSION
that patients with PD suffer a decreased sensitivity to sen-
An unequivocal result of this study is that grip force
sory input acting on structures at a cortical level. We would
abnormalities were present in the early stages of PD, in
argue that this is supported further by our findings. Firstly,
although the scaling of grip force levels to load was main-
more, the greatest abnormalities were observed in grip
tained, a general shift to larger values was found. Secondly,
force magnitude. Thus the hypothesis put forward by
the extent of the exaggerated grip force relative to the
Gordon and Reilmann,11 that exaggerated grip forces are
control values was significantly higher for the light load
than for the heavy load. As more afferent input would be
L-dopa medication, is contradicted by our
findings. Another suggestion, namely that exaggerated
expected in the latter case, it could be argued that theexaggerated grip force levels result from a degree of insen-
grip force levels result from L-dopa-induced dyskine-
sitivity to afferent input caused by an upward shift in the
sia,13 can also be ruled out as an explanation for our
threshold level at which sensory input can act effectively.
findings, as none of the patients showed dyskinesia and
The finding that the relative grip force abnormalities are
as de novo patients had had clearly no chance to develop
most pronounced for the SGF, the control of which relies
L-dopa-induced dyskinesia. Indeed, the grip force pro-
heavily on cutaneous feedback information, further sup-
files of parkinsonian patients with L-dopa-induced dys-
kinesia (Wenzelburger and associates,13 Fig. 2C) resem-
In summary, we conclude that exaggerated grip force
observed in patients with PD are intrinsic features of the
Huntington’s disease (see Hermsdo¨rfer and colleagues,5
pathophysiology of the disease, and not the result of
Fig. 2A) than the markedly slowed profiles obtained in
dopamine medication or its side effects. Rather, we sug-
the present study and in a group of PD patients on a
gest that abnormalities arise from decreased efficiency in
stable L-dopa regime,9 indicating that a different patho-
the utilization of sensory input concerning object prop-
physiology may underlie the two phenomena.
erties and the performance of the motor apparatus.
Although this is more a matter of interpretation, we
would also argue that the present results provide strong
Acknowledgments: This work was supported by grants
support for the hypothesis that grip force abnormalities in a
from the Deutsche Forschungsgemeinschaft as part of the pro-
variety of basal ganglia disorders result from a disturbance
gram SPP 1001 “sensomotorische Integration”. We thank Pro-fessor M. Schwarz, Dr. R. To¨pper, and Dr. P. Weiss-Blanken-
of sensorimotor processing.5,9,16 This idea arose in part
horn for fruitful discussions of our findings.
from the similarities between exaggerated grip force pro-files seen in basal ganglia disorders and those of neurolog-
REFERENCES
ically normal subjects with a local anesthesia-induced block
1. Fellows SJ, Ernst J, Schwarz M, To¨pper R, Noth J. Precision grip
of the cutaneous receptors of the hand and wrist,17 or in
deficits in cerebellar disorders in man. Clin Neurophysiol 2001;
patients with sensory neuropathy of the fingers.18 Peripheral
sensory function, however, is largely normal in basal gan-
2. Fellows SJ, Schwarz M, Schaffrath C, Do¨mges F, Noth J. Senso-
rimotor deficits and the delay of compensatory responses to slip of
glia disorders, implying that disordered central processing
an object held in the fingers of patients with Huntington’s disease.
of sensory input is the likely cause of any abnormalities.
Electroencephalograph Clin Neurophysiol 1998;106:41– 42P.
Reports of abnormal sensorimotor function in PD have
3. Gordon A, Quinn L, Reilmann R, Marder K. Coordination of
prehensile forces during precision grip in Huntington’s disease.
appeared steadily in recent years. In particular, parkinsonian
patients performing arm movements without visual guid-
4. Hermsdo¨rfer J, Wessel K, Mai N, Marquardt C. Perturbation of
ance regularly underestimate the extent of a movement,
precision grip in Friedrich’s ataxia and late-onset cerebellar ataxia. Mov Disord 1994;9:650 – 654.
either passively imposed or self-performed,19–22 and have
5. Schwarz M, Fellows SJ, Schaffrath C, Noth J. Deficits in sensori-
difficulty in judging arm or finger position on the basis of
motor control during precise hand movements in Huntington’s
proprioceptive information alone.23 A similar deficit has
disease. Clin Neurophysiol 2001;112:95–106.
6. Serrien D, Burgunder JM, Wiesendanger M. Disturbed sensorimo-
been observed when patients replicating a movement im-
tor processing during control of precision grip in patients with
posed on the other hand must rely solely on kinesthetic
writer’s cramp. Mov Disord 2000;15:965–972.
information or receive visual cues designed to distract them
7. Serrien D, Wiesendanger M. Grip-load force co-ordination in
cerebellar patients. Exp Brain Res 1999;128:76 – 80.
from relevant kinesthetic input.24 It was found recently that
8. Ingvarsson P, Gordon A, Forssberg H. Coordination of manipula-
patients with PD lack the inhibition of responses in wrist
tive forces in Parkinson’s disease. Exp Neurol 1997;145:489 –501.
muscles to transcortical magnetic stimulation seen normally
9. Fellows SJ, Noth J, Schwarz M. Precision grip and Parkinson’s
disease. Brain 1998;121:1771–1784.
during passive movement of the joint at which the target
10. Mu¨ller F, Abbs J. Precision grip in Parkinsonian patients. In:
muscles operate.25 Taken together, these results indicate
Streifler M, Korczyn A, Melamed E, Youdim M, editors. Advances
Movement Disorders, Vol. 19, No. 5, 2003VERB PROCESSING IN HUNTINGTON’S DISEASE
in neurology, Vol.53. Parkinson’s disease: anatomy, pathology and
and in a non-demented group (n ؍ 17, Dementia Rating
therapy. New York: Raven Press; 1990. p 191–195. Scale > 129) of Huntington’s disease (HD) patients com-
11. Gordon A, Reilmann R. Getting a grasp on research: does treatment
pared to 26 matched normal subjects. We did not find a
taint testing of parkinsonian patients? Brain 1999;122:1597–1598. specific deficit for verb production in non-demented pa-
12. Castiello U, Bennett K, Bonfiglioli C, Peppard R. The reach-to-
grasp movement in Parkinson’s disease before and after dopami-
tients who had a performance similar to but weaker than
nergic medication. Neuropsychologia 2000;38:46 –59. that of the controls across the four tasks. The profile of
13. Wenzelburger R, Zhang BR, Pohle S, et al. Force overflow and
results was different in the demented group because, apart
levodopa-induced dyskinesias in Parkinson’s disease. Brain 2002;
from a global deficit whatever the task in comparison with both non-demented and control groups, the demented pa-
14. Gordon A, Westling G, Cole K, Johanson RS. Memory represen-
tients exhibited increased difficulties in the two tasks im-
tations underlying motor commands used during manipulation ofcommon and novel objects. J Neurophysiol 1993;69:1789 –1796. plying verb production. The deficit of verb production ob-
15. Westling G, Johansson RS. Factors influencing the force control
served in demented HD patients is discussed in relation to
during precision grip. Exp Brain Res 1984;53:277–284. the damage to the motor loop in HD patients at later stages
16. Noth J, Fellows SJ, Schwarz M, To¨pper R. Disturbances of preci-
of disease. 2003 Movement Disorder Society
sion grip in movement disorders. Pflu¨gers Arch 2001;441:R117.
17. Macefield V, Ha¨ger-Ross C, Johansson RS. Control of grip force
Key words: Huntington’s disease; language; word genera-
during restraint of an object held between finger and thumb:
responses of cutaneous afferents from the digits. Exp Brain Res1996;108:155–171.
18. Thonnard JL, Detrembleur C, Van den Bergh P. Assessment of
Besides motor deficiencies, Huntington’s disease
hand function in a patient with chronic sensory demyelinatingneuropathy. Neurology 1997;49:253–257.
(HD) is characterized by several cognitive deficits in
19. Demirci M, Grill S, McShane L, Hallet M. A mismatch between
memory and executive functions such as problem solv-
kinesthetic and visual perception in Parkinson’s disease. Ann Neu-
ing, visuoperceptive processing, and spatial or arithmet-
20. Jobst E, Melnick M, Byl N, Dowling G, Aminoff M. Sensory
ical reasoning.1 Language disorders mainly concern
perception in Parkinson disease. Arch Neurol 1997;34:450 – 454.
“frontal” aspects such as some features of syntactic abil-
21. Klockgether T, Borutta M, Rapp H, Spieker S, Dichgans J. A defect
ities2,3 and verbal fluency.4 Ho and colleagues4 specified
of kinesthesia in Parkinson’s disease. Mov Disord 1995;10:460 – 465.
22. Schneider J, Diamond S, Markham C. Parkinson’s disease: sensory
that this fluency deficit seems to concern specifically the
and motor problems in arms and hands. Neurology 1987;37:951–956.
ability to switch across subcategories, reflecting impair-
23. Zia S, Cody F, O’Boyle D. Joint position sense is impaired by
Parkinson’s disease. Ann Neurol 2000;47:218 –228.
ment of frontostriatal circuits, rather than the size of
24. Byblow WD, Lewis GN, Stinear JW. Effector-specific visual in-
formation influences kinesthesis and reaction time performance in
The frontal nature of language impairment in HD can
Parkinson’s disease. J Mot Behav 2003;35:97–102.
25. Lewis GN, Byblow WD. Altered sensorimotor integration in Par-
be envisaged in another paradigm that concerns a differ-
kinson’s disease. Brain 2002;125:2089 –2099.
ential deficit between verb and noun processing. Clinicalevidence5–9 shows a relationship between object-namingdeficit and damage to the left temporal lobe, and between
action-naming deficit and large lesions in the left frontalcortex. Damasio and Tranel7 formulated the hypothesis
that in the left hemisphere, noun retrieval is mediatedpreferentially by temporal regions, whereas verb re-
Jean-Franc¸ois De´monet, MD, PhD, Cyril Pernet, MSc,
trieval is subserved by a large network including the
prefrontal cortex; this hypothesis has received further
Institut National de la Sante´ et de la Recherche Me´dicale U
support in studies devoted to degenerative diseases af-
455, Fe´de´ration de Neurologie, Centre Hospitalier
fecting the frontal cortex. A verb deficit was observed in
Universitaire Purpan, Toulouse, France
frontotemporal dementia10 and in motor neuron diseaseassociated with pathological changes in two frontal ar-
Abstract: We compared noun- and verb-generation tasks in
eas, namely Brodmann areas 44 and 45.11 Language
a demented group (n ؍ 9, Dementia Rating Scale < 129)
studies in Parkinson’s disease (PD) have also revealedthe existence of such dysfunction; Grossman and col-leagues12 showed a verb learning impairment in a group
*Correspondence to: Patrice Pe´ran, INSERM U 455, CHU Purpan, 31059
Toulouse Cedex 3, France. E-mail: [email protected]
of early PD patients. Our group has shown recently that
Received 26 April 2003; Revised 23 July 2003, 8 October 2003;
word generation tasks may be useful to unveil in non-
demented PD patients a specific impairment of verb
Published online 12 December 2003 in Wiley InterScience (www. interscience.wiley.com). DOI: 10.1002/mds.10706
production compared with noun generation.13
Movement Disorders, Vol. 19, No. 5, 2003
V Congreso Internacional del CLAD sobre la Reforma del Estado y de la Administración Pública, Santo Domingo, 24-27 Oct. 2000 Finanças públicas e orçamento participativo: a experiência municipal brasileira Eduardo de Lima Caldas Curso de Mestrado em Administração Pública e Governo Introdução O objetivo deste trabalho é apresentar a experiências de elaboração de orçamen
One Step Myoglobin/CK-MB/Troponin I Combo Test Device Blood/Serum/Plasma) can be performed using whole blood (from venipuncture or *NOTE: The intensity of the color in the test line region(s) will vary depending on the (Whole Blood/Serum/Plasma) concentration of Myoglobin, CK-MB and/or Troponin I present in the specimen. One Step Troponin I To collect Fingerstick Whole Blood
 status and object load as the main factors. Post-hoctesting was carried out using the Tukey-Kramer test.
status and object load as the main factors. Post-hoctesting was carried out using the Tukey-Kramer test. GRIP FORCE ABNORMALITIES IN DE NOVO PD
FIG. 3. Group values for the four lifting pa-
GRIP FORCE ABNORMALITIES IN DE NOVO PD
FIG. 3. Group values for the four lifting pa-