Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Serr.qxd
One-year Results of Photorefractive Keratectomy With and Without Surface Smoothing Using the Technolas 217C Laser
Sebastiano Serrao, MD, PhD; Marco Lombardo, MD
ABSTRACT PURPOSE: To assess the efficacy, predictability,
Several factors can affect smoothness of the
stability, and safety of a smoothing technique in patients with myopia immediately after photore-
laser beam diameter1, laser beam homogeneity, the
fractive keratectomy (PRK) using a scanning-spot excimer laser.
ejected molecular ablative debris deposited back
METHODS: Using the Technolas 217C excimer
onto the corneal surface, and the thermal compo-
laser, PRK was performed on 100 eyes of
nent of the ablation process. Most refractive surgery
54 patients. Ablation zone diameter was 6.0 mm and
techniques are associated with irregularities on the
transition zone diameter was 9.0 mm. The eyes
corneal surface which, in turn, may cause an
were randomized into two groups: in 50 eyes PRK alone was performed and in the other 50 eyes, a
increase in the number high order aberrations and
smoothing technique was performed after the ini-
reduced visual acuity in certain light conditions. tial ablation. Preoperative mean spherical equiva-
The reduction in the regularity of the first corneal
lent refraction was -4.98 ± 1.71 D in the PRK only
surface after the photoablation phase of photore-
group (range -2.25 to -8.60 D) and -4.82 ± 1.61 D in
fractive keratectomy (PRK) can lead to three unde-
the smoothing group (range -2.00 to -8.00 D). Follow- up was 12 months for all patients.
sirable phenomena: a decrease in corneal trans-
RESULTS: At 1 year after surgery, mean manifest
parency2, regression of refractive outcome3, and a
spherical equivalent refraction was -0.61 ± 0.50 D (range -2.25 to +0.62 D) in the PRK only group and
The irregularity of the ablated surface is the
in the smoothing group, +0.02 ± 0.32 D (range -0.75
“primum movens” for delayed wound healing and
to +0.75 D). Postoperative regularity topographic indices were lower in the smoothing group than in
abnormal epithelial and stromal remodeling. the PRK group (P<.001).
Abnormalities include stromal thickening and
CONCLUSIONS: Smoothing after PRK for cor-
epithelial hyperplasia or distortion of the existing
rection of myopia up to -6.50 D increased surface regularity, as expressed by lower topography sur-
In our opinion, none of the laser systems devel-
face regularity indices, and reduced the incidence and severity of postoperative haze. We observed
oped to date produce a sufficiently smooth stromal
higher predictability throughout follow-up in the
surface. This, in addition to patient eye and head
smoothing group, which may be addressed by a
movements during laser refractive surgery, result in
nomogram adjustment in the PRK only group.
erroneous targeting of the surgical beam and hence
[J Refract Surg 2004;20:444-449]
a sub-optimal correction.8 Efforts by laser manufac-turers to produce more sophisticated eye trackingdevices9 and to improve the quality of the emittedlaser light have not yet produced an optimal out-come. From the Catholic University of Rome, Department of Ophthalmology,Rome, Italy (Serrao, Lombardo) and the University of Padua, Department
Carones demonstrated that even when the most
of Ophthalmology, Padua, Italy (Serrao).
effective eye tracking system was employed,
The authors have no financial interest in the materials described
Maloney's topographic regularity index (BFTI) did
Correspondence: Sebastiano Serrao MD, PhD, Via Orazio 31, 00193
not significantly differ from that achieved when
Rome, Italy. Tel: 39.380.333.11.00; Fax: 39.380.333.11.00; E-mail:
other devices were used. The eye tracker device is
advantageous, especially in uncooperative patients
Received: December 5, 2002Accepted: March 30, 2004Journal of Refractive Surgery Volume 20 September/October 2004 PRK With and Without Smoothing Using the Technolas 217C Laser/Serrao and Lombardo
Many authors have evaluated the physical char-
corneal surgery.12 In this study, we compare the
acteristics of various types of excimer lasers. Huang
refractive data and corneal regularity indices of eyes
and Arif simulated corneal ablations using different
treated using the same excimer laser system
beam diameters and beam profiles similar to those
(Technolas 217C), with PRK alone and PRK with
currently used in commercial excimer laser sys-
tems.1 Their aim was to study the efficacy of thescanning laser in correcting high order aberrations. PATIENTS AND METHODS
They concluded that beam sizes р1 mm should besufficient for elimination of most high order optical
Patients
Fifty-four patients (35 women and 19 men)
Other authors have compared the operative out-
between 22 and 50 years of age (mean 33.8±6.21 yr)
come with a broad beam laser to that observed with
were recruited for a total of 100 treated eyes.
scanning spot and scanning slit lasers. They con-
Patients were randomly enrolled from the excimer
cluded that the corneal surface was smoothest fol-
laser surgery waiting list of the Department of
lowing scanning spot laser surgery.10 At present, it
Ophthalmology of the Catholic University of Rome.
is widely held that a smooth postoperative ablation
Inclusion criteria were the absence of ocular
surface is mandatory if refractive surgery is to be
pathology, no previous ocular surgery, refractive
considered maximally effective. Benefits of a regu-
astigmatism less than 1.50 diopters (D), and at least
lar corneal surface include faster re-epithelializa-
1 year of refractive stability. Patients wearing con-
tion, less haze and regression, and improved visual
tact lenses were asked to discontinue use for at least
performance. As suggested by Vinciguerra and col-
4 weeks prior to preoperative evaluation. Informed
leagues, the smoothing technique is an effective pro-
consent was obtained from all patients.
cedure for achievement of a smoother ablated stro-
Preoperative evaluation included the determina-
tion of manifest and cycloplegic refraction, uncor-
In spite of the fact that the results following PRK
rected visual acuity (UCVA) both for reading and
performed using the Technolas 217C are satisfacto-
distance, best spectacle-corrected visual acuity
ry, all users must include some hypercorrection in
(BSCVA), and autorefraction (Nidek AR-600, Tokyo,
the treatment planning (about 5% to 10% of the
Japan). Slit-lamp microscopy, tonometry, and fun-
spectacle correction). This is done to avoid the over-
dus examination were also performed. Corneal
correction consequent to regression of refractive out-
thickness was measured using a contact ultrasound
come that occurs in the months following surgery.
pachymeter (Optikon 2000, Rome, Italy) and corneal
We believe that this regression is due to the irregu-
topography was performed with the Keratron Scout
larity of the ablated corneal surface. We present
(Optikon). Emmetropia was the refractive goal in all
results obtained when a smoothing technique was
performed after refractive treatment (PRK) using a
We randomized the eyes into two groups using a
statistical package (Matlab, software version 6.5).
The smoothing technique was used to obtain a
In one group (26 patients; 16 women and 10 men,
smooth ablation surface, thus eliminating gross and
mean age 34.7 ± 4.97 yr; 50 eyes) PRK only was per-
small irregularities and flattening the borders of the
formed, whereas in the second group (28 patients;
ablation edges. This technique is similar to pho-
19 women and 9 men, mean age 31.7 ± 7.45 yr;
totherapeutic keratectomy (PTK), which is useful
50 eyes), smoothing was performed immediately
for treatment of corneal diseases such as Reis-
Bückler's dystrophy or band-like keratopathy, and
Mean preoperative refraction (mean cycloplegic
in order to achieve corneal smoothness after ptery-
spherical equivalent refraction ± standard devia-
tion) was -4.98 ± 1.71 D in the PRK only group
Other studies2,3 have demonstrated that smooth-
(mean cylinder -0.58 ± 0.41 D) and -4.82 ± 1.61 D in
ing after PRK using a scanning slit laser, such as
the smoothing group (mean cylinder -0.55 ± 0.53 D).
the the Nidek EC-5000, facilitates a better optical
Statistical comparison of preoperative data in
surface, better visual results, and less haze and
both groups revealed no significant differences
regression. Alió and colleagues demonstrated that
(Fischer test, P>.05). Statistically significant differ-
the Technolas 217C laser used in PTK mode with a
ences between means of the two study groups were
masking fluid was useful for treating irregular
determined by the Student's paired t-test. P-values
corneal astigmatism caused by previous refractive
less than .05 were considered significant.
Journal of Refractive Surgery Volume 20 September/October 2004 PRK With and Without Smoothing Using the Technolas 217C Laser/Serrao and Lombardo Mean Cycloplegic Spherical Equivalent Refraction (D) Before and After PRK, With and Without Smoothing, in 100 Eyes of 54 Patients (Number of Eyes Examined) Refractive Range (D) Preoperative Postoperative PRK with smoothing -1.75 to -3.00 PRK only -1.75 to -3.00 Surgical Technique
until complete re-epithelialization of the cornea,
Surgery was performed by one surgeon (SS)
sodium diclofenac 0.1% preservative-free eyedrops
under topical anesthesia achieved using oxybupro-
three times daily for 3 days, topical fluorometholone
caine hydrochloride eye drops. The corneal epitheli-
0.1% twice daily for 1 month after complete re-
um was removed using the Amoils brush. Laser
epithelialization, and sodium hyaluronate 0.18%
ablation was performed using the Bausch & Lomb
hypotonic solution preservative-free eyedrops five
Technolas 217C Planoscan excimer laser (Bausch &
times daily for 6 months after surgery. A bandage
Lomb Chiron Technolas, Dornach, Germany; wave-
contact lens was applied until the third postopera-
length 193 nm). Ablation zone diameter was
6.0 mm and transition zone diameter was 9.0 mm.
Twelve-month follow-up included evaluation of
This laser is also equipped with an active eye track-
corneal haze, UCVA and BSCVA, refraction, corneal
er device and utilizes a 2-mm flying-spot laser
topography, evaluation of high order aberrations
beam. The fluence at the corneal plane was
from the first corneal surface, pachymetry, and
120 mJ/cm², the ablation rate was 0.25 µm per
pulse, and the repetition rate (frequency) was 50 Hz. No nomogram adjustment was used in this study.
Final smoothing was performed with the same
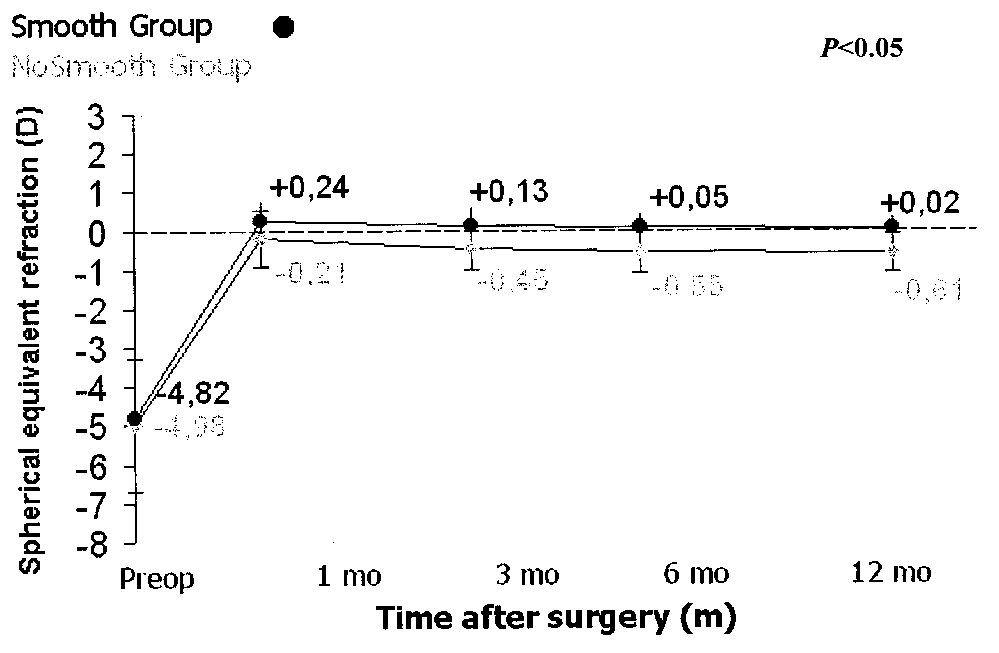
At 1-year follow-up, mean cycloplegic spherical
laser in PTK mode. The maximum diameter of the
equivalent refraction in the PRK only group was
ablation zone was 9.00 mm. A viscous solution of
-0.61 ± 0.50 D; in the smoothing group it was +0.02
0.25% sodium hyaluronate was used for masking
± 0.32 D (Table). Differences in spherical equivalent
the cornea. The fluence, ablation rate, and frequen-
refractive error observed in the two groups at
cy in the PTK mode were the same as in PRK mode.
1 month (P<.05), 3 months (P<.05), 6 months
Before the procedure, we re-targeted the ablation
(P<.05), and 1 year (P<.05) following surgery were
area at the center of the pupil and fixed it with the
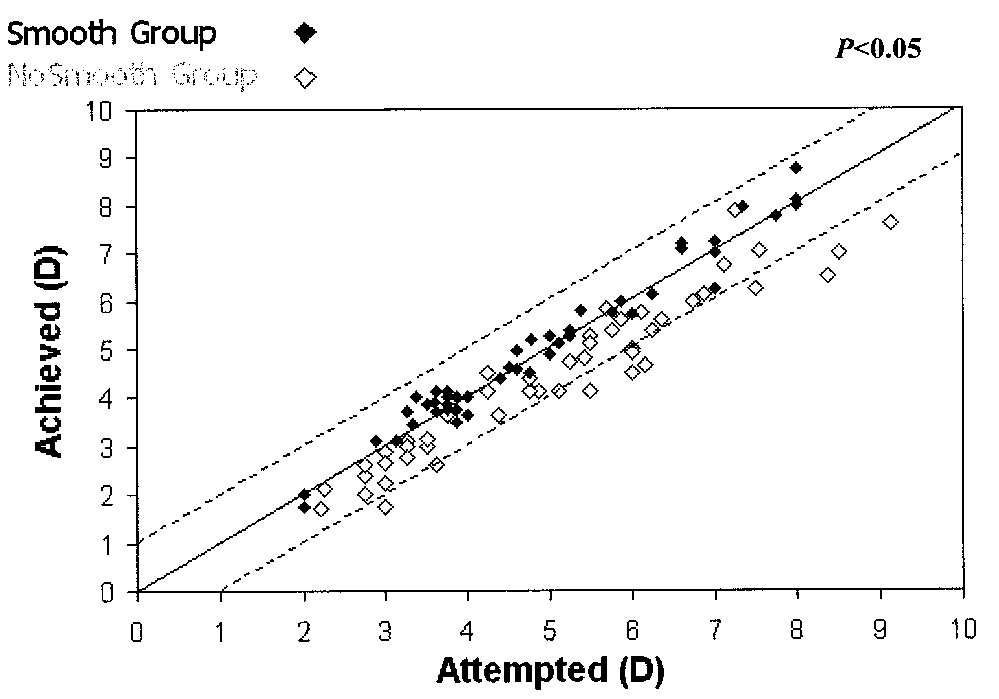
The scattergram of the attempted versus the
We standardized the smoothing procedure using
achieved correction for both groups is shown
the Technolas 217C laser. Ablation depth was set at
in Figure 1. Twenty-six eyes (52%) had a manifest
10 µm (divided into four intervals for a total of
spherical equivalent refraction within ±0.50 D of
428 spots) and a spatula was used to spread the
emmetropia in the PRK only group, whereas this
masking fluid on the corneal surface.
result was achieved in 46 eyes (92%) in the smooth-
The viscous masking solution formed a stable and
ing group; 41 eyes (81%) were within ±1.00 D in the
uniform coating on the surface of the eye. In partic-
PRK only group and 50 eyes (100%) were within
ular, it filled the depressed areas on the cornea and
±1.00 D in the smoothing group. Figure 2 shows
efficaciously masked the tissue to be protected
mean spherical equivalent refraction during follow-
Postoperatively, patients were prescribed micro-
Preoperative refractive astigmatism ranged from
nomicin preservative-free eyedrops six times daily
0 to -1.50 D in both groups, with a mean of -0.58 ±
Journal of Refractive Surgery Volume 20 September/October 2004 PRK With and Without Smoothing Using the Technolas 217C Laser/Serrao and Lombardo Figure 2. Mean (SD) change in cycloplegic refraction during follow- Figure 1. Scattergram at 1 year after PRK shows slight overcorrec-
up in the two study groups. There was a slight hyperopic shift in the
tion of the refractive target in the PRK only group (50 eyes) and the
smoothing group during the early postoperative period. A regression
high predictability of the refractive results in the PRK with smooth-
of the refractive effect occurred in the PRK only group between the
ing group (50 eyes). The P-value was calculated using Student's
1st and 3rd postoperative months. P-value was statistically signifi-
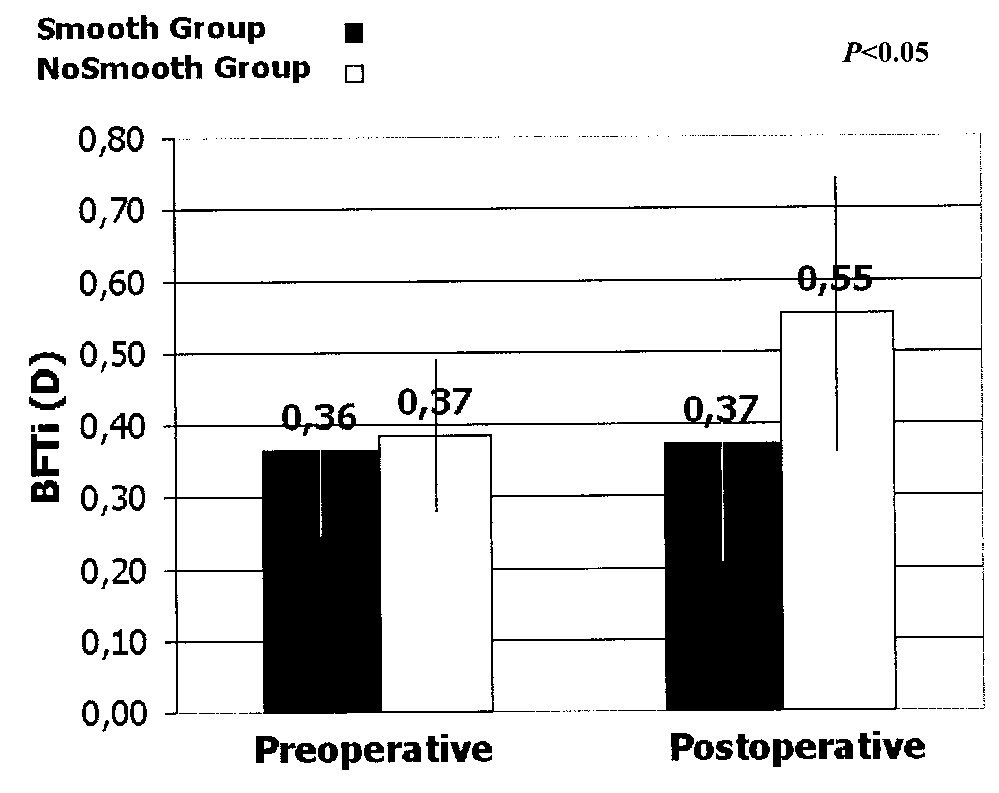
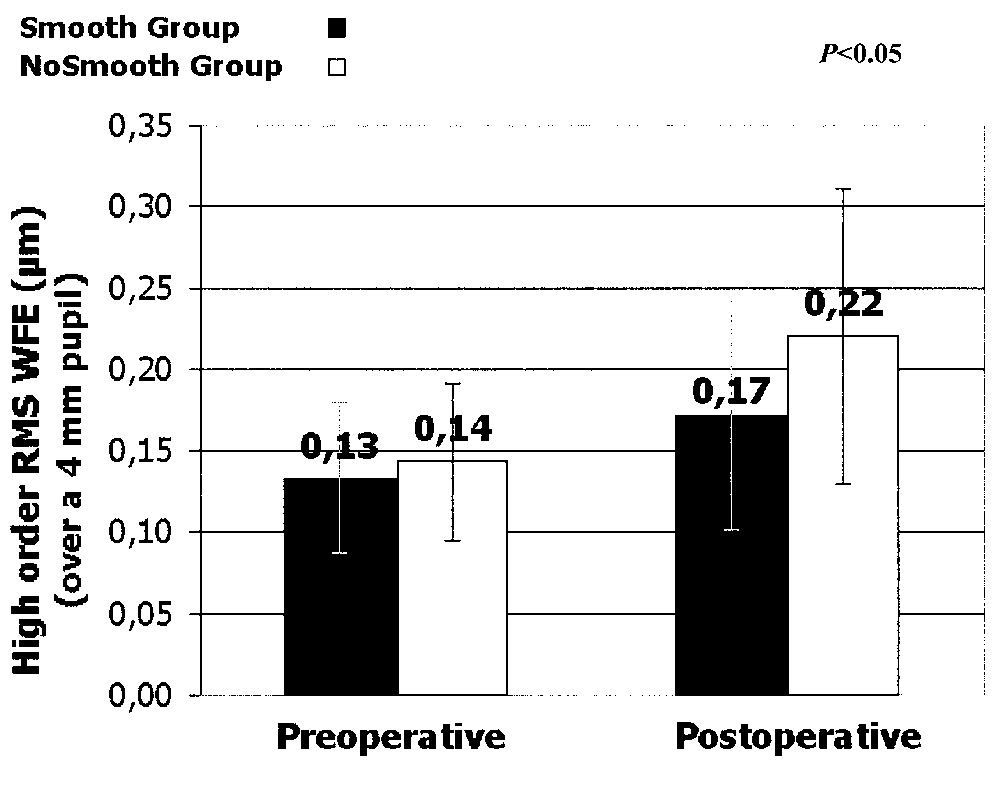
cant (P<.05) at each follow-up examination. Figure 3. At the end of follow-up, an increase in the postoperative Figure 4. At 1 year after PRK with and without smoothing, the ablat-
topographic irregularity index (BFTI) was observed in the PRK only
ed first corneal surface showed a mean increase of the 3rd to 6th
group. The regression observed in this group may be explained by
high order optical aberrations. The smoothing technique performed
the more marked irregularity of the ablated corneal surface. The
at the end of the PRK procedure reduced postoperative stromal
irregularities, facilitating a more even surface with respect to PRKonly. The mean induced high order optical aberrations in the PRKwith smoothing group was less marked (P<.05).
0.41 D in the PRK only group and -0.55 ± 0.53 D in
with an efficacy index of 1.03 versus 0.97 in the PRK
the smoothing group. At 1 year, refractive astigma-
only group, where only two eyes (4%) gained 2 or
tism was reduced to a mean -0.37 ± 0.40 D in the
PRK only group and +0.05 ± 0.51 D in the smooth-
Two eyes (4%) in the smoothing group and six
ing group, with no surgically-induced astigmatism.
eyes (12%) in the PRK only group had haze greater
No eye lost any Snellen lines of spectacle-correct-
ed visual acuity during follow-up. The safety index
The regularity of the first corneal surface was
was 1.02 in the PRK only group and 1.06 in the
determined using two topographic indices: Best Fit
smoothing group. In the smoothing group, 10 eyes
Topographic Irregularity (BFTI)14 and the high
(20%) gained 2 or more lines of Snellen visual acuity
order root-mean-square wavefront error (RMS). Journal of Refractive Surgery Volume 20 September/October 2004 PRK With and Without Smoothing Using the Technolas 217C Laser/Serrao and Lombardo
The BFTI is measured in diopters and is fit to the
ularities induce a more pronounced healing
central 4-mm-diameter circle at the center of the
response when compared to a smoother ablation
videokeratograph to approximate the size and loca-
surface.21 Altered wound healing is the first step
tion of the entrance of the pupil; it is defined as the
toward the onset of haze and a less than desirable
root-mean-square sum of the differences between
the measured cornea and the best-fit spherocylinder
In our PRK study, we used a 2-mm beam spot size
that minimizes the distance between the two sur-
device. In one group, smoothing was performed
immediately after PRK. Results confirm that the
High order RMS is measured in microns and rep-
smoothing technique improved the quality of the
resents the difference between the measured
ablated corneal surface and visual outcome, espe-
corneal wavefront and an aberration-free wave-
cially in eyes with a spherical equivalent refraction
front. We calculated RMS over a 4-mm-diameter
up to -6.50 D. The observed hyperopic shift was due
pupil and for 3rd to 6th Zernike orders.
to the diameter of the optical zone of the Technolas
Figures 3 and 4 show preoperative and 1-year
217C laser. This instrument allows for a maximum
postoperative values for BFTI and RMS in the two
PTK zone of 6 mm with a 3-mm transition zone.
study groups. Postoperative values were greater
When this smoothing technique is performed using
than preoperative values, showing that ablation
a Nidek EC-5000 laser with a 9-mm PTK zone with-
caused an increase in irregularity; the increase was
out transition, it did not induce a consistent hyper-
less consistent in the smoothing group and the dif-
opic shift for such a limited tissue ablation (up to
ference was statistically significant (P<.05). A post-
operative reduction in RMS was observed in nine
Many authors report induction of a hyperopic
eyes (18%) in the smoothing group, but in only two
shift for attempted correction as the major compli-
cation of PTK.23 Various techniques have been pro-posed to minimize the refractive shift: use of a
DISCUSSION
masking agent to reduce the real depth of tissue
In accordance with other reports3, we observed
ablation, use of a large ablation zone with a transi-
that the outcome of refractive surgery was influ-
tion zone, and setting a low ablation depth.24-27
enced primarily by final optical quality of the ablat-
Corneal topography analysis can identify whether
ed corneal surface. In experimental settings, a PTK-
or not the better result was due only to the hyper-
type treatment at the end of PRK allows for a
opic shift. For this reason, we analyzed the topo-
smoother ablation.10,15,16 Smoothing of the corneal
graphic indices and the topographic wavefront. The
surface involves the use of a fluid that, when applied
BFTi and the RMS over a 4-mm-diameter pupil and
to the cornea, masks deeper tissues while at the
for 3rd to 6th Zernike orders demonstrated a differ-
same time leaves protruding irregularities
ence between the two groups: the smoothing group
exposed17; subsequent ablation of the irregular
had a result closer to emmetropia but it was also
anterior stromal surface should therefore focally
associated with better topographic indices.
excise elevated corneal tissue, thereby reducing sur-
In our clinical study, the eyes in which smoothing
was performed postoperatively had higher pre-
The ideal fluid to be used in this technique has
dictability for the refractive target; this may be
not yet been established. The 0.25% sodium
explained by the hyperopic shift induced by PTK,
hyaluronate masking fluid that we used is a moder-
and might also be achieved in the PRK only group
ately viscous solution with an ablation rate similar
by a nomogram adjustment. In the smoothing
to that of corneal tissue. Thanks to these properties,
group, we found a more regular first corneal surface
it can cover the irregular surface uniformly and not
as expressed by topography indices and better visu-
run off too quickly, hence, only stromal peaks are
al acuity, compared to the PRK only group.
This smoothing procedure, which facilitated a
A smoother surface allows for better epithelial
smoother anterior stromal surface compared to PRK
adhesion and migration. Experimental studies have
alone, permitted faster re-epithelialization7,28,29
shown that epithelial migration can be inhibited by
with less haze and better visual outcome.
irregularities in the surface of the substratum.18,19
Performing smoothing at the end of PRK was an
Correct and rapid re-epithelialization is the prin-
effective means to improve corneal regularity after
cipal process that regulates epithelial and stromal
PRK with a scanning laser system, with a beam size
remodeling after PRK. Postoperative ablation irreg-
Journal of Refractive Surgery Volume 20 September/October 2004 PRK With and Without Smoothing Using the Technolas 217C Laser/Serrao and Lombardo REFERENCES
1. Huang D, Arif M. Spot size and quality of scanning laser cor-
15. Fasano AP, Moreira H, McDonnel PJ, Sinbaway A. Excimer
rection of higher-order wavefront aberrations. J Cataract
laser smoothing of a reproducible model of anterior corneal
surface irregularity. Ophthalmology 1991;98-1782-1785.
2. Vinciguerra P, Azzolini M, Radice P, Sborgia M, De Molfetta
16. Horgan SE, McLaughlin-Borlace L, Stevens JD, Munro
V. A method for examining surface and interface irregulari-
PMG. Phototherapeutic smoothing as an adjunct to photore-
ties after photorefractive keratectomy and laser in situ ker-
fractive keratectomy in porcine corneas. J Refract Surg
atomileusis: Predictor of optical and functional outcomes.
17. Kornmehl EW, Steinert RF, Puliafito CA. A comparative
3. Vinciguerra P, Azzolini M, Airaghi P, Radice P, De Molfetta
study of masking fluids for excimer laser phototherapeutic
V. Effect of decreasing surface and interface irregularities
keratectomy. Arch Ophthalmol 1991;109:860-863.
after photorefractive keratectomy and laser in situ ker-
18. Fitton JH, Dalton BA, Beumer G, Johnson G, Griesser HJ,
atomileusis on optical and functional outcomes. J Refract
Steele JG. Surface topography can interfere with epithelial
tissue migration. J Biomed Mater Res 1998;42:242-257.
4. Applegate RA, Hilmantel G, Howland HC, Tu EY, Starck T,
19. Steele JG, Johnson G, McLean KM, Beumer GJ, Griesser
Zayac EJ. Corneal first surface optical aberrations and
HJ. Effect of porosity and surface hydrophilicity on migra-
visual performance. J Refract Surg 2000;16:507-514.
tion of epithelial tissue over synthetic polymer. J Biomed
5. Moller-Pedersen T, Li HF, Petroll WM, Cavanagh HD,
Jester JV. Confocal microscopic characterization of wound
20. Wilson SE. Molecular cell biology for the refractive corneal
repair after photorefractive keratectomy. Invest Ophthalmol
surgeon: programmed cell death and wound healing.
6. Fantes FE, Hanna KD, Waring G III, Pouliquen Y,
21. Lee YC, Wang IJ, Hu FR, Kao WWY. Immunohistochemical
Thompson KP, Savoldelli M. Wound healing after excimer
study of subepithelial haze after phototherapeutic keratec-
laser keratomileusis (photorefractive keratectomy) in mon-
tomy. J Refract Surg 2001;17:334-341.
keys. Arch Ophthalmol 1990;108:665-675.
22. Wilson Se, Mohan RR, Hong JW, Lee JS, Choi R, Mohan RR.
7. Weber BA, Gan L, Fagerholm P. Wound healing response in
The wound healing response after laser in situ keratomileu-
the presence of stromal irregularities after excimer laser
sis and photorefractive keratectomy: elusive control of bio-
treatment. Acta Ophthalmol Scand 2001;79:381-388.
logical variability and effect on custom laser vision correc-
8. Taylor NM, Eikelboom RH, van Sarloos PP, Reid PG.
tion. Arch Ophthalmol 2001;119:889-896.
Determining the accuracy of an eye tracking system for
23. Amano S, Oshika T, Tazawa Y, Tsuru T. Long-term follow-up
laser refractive surgery. J Refract Surg 2000;16:S643-S646.
of excimer laser phototherapeutic keratectomy. Jpn J
9. Fiore T, Carones F, Brancato R. Broad beam vs. flying spot
excimer laser: refractive and videokeratographic outcomes
24. Dogru M, Katakami C, Yamanaka A. Refractive changes
of two different ablation profiles after photorefractive kera-
after excimer laser phototherapeutic keratectomy.
tectomy. J Refract Surg 2001;17:534-541.
J Cataract Refract Surg 2001; 27:686-692.
10. Argento C, Valenzuela G, Huck H, Cremona G, Cosentino
25. Liu C. Hyperopic shift and the use of masking agents in
MJ, Ruiz Gale MF. Smoothness of ablation on acrylic by four
excimer laser superficial keratectomy. Br J Ophthalmol
different excimer lasers. J Refract Surg 2001;17:43-45.
11. Dogru M, Katakami C, Miyashita M, Hida E, Uenishi M,
26. Fagerholm P. Phototherapeutic keratectomy: 12 years of
Tetsumoto K, Kanno S, Nishida T, Yamanaka A. Ocular sur-
experience. Acta Ophthalmol Scand 2003;81:19-32.
face changes after excimer laser phototherapeutic keratec-
27. Schipper I, Senn P, Lechner A. Tapered transition zone and
tomy. Ophthalmology 2000;107:1144-1152.
surface smoothing ameliorate the results of excimer-laser
12. Alio JL, Belda JI, Shalaby AM. Correction of irregular astig-
photorefractive keratectomy for myopia. Ger J Ophthalmol
matism with excimer laser assisted by sodium hyaluronate.
28. Serrao S, Lombardo M, Mondini F. Photorefractive keratec-
13. Koch DD, Kohnen T, Obstbaum SA, Rosen ES. Format for
tomy with and without smoothing: a bilateral study.
reporting refractive surgical data. J Cataract Refract Surg
29. Reidy JJ, Jacobson MS, Thompson HW, Beuerman RW,
14. Maloney RK, Bogan SJ, Waring GO III. Determination of
Leach DH, McDonald MB. Comparison of corneal epithelial
corneal image-forming properties from corneal topography.
wound healing after photorefractive and lamellar keratec-
tomy. J Refract Surg 1996;12:352-357. Journal of Refractive Surgery Volume 20 September/October 2004
§ 16 : Comerciante - Contrato de venta . 1 COMERCIAL (actos -) = MERCANTIL (espíritu -, REGISTRO -) COMERCIANTE (noción jurídica): Depende de la JURISDICCIóN de los TRIBUNALES DE COMERCIO el JUEZ CONSULAR el JUICIO el JUZGADO el TRIBUNAL el LITIGIO el PLEITO la SENTENCIA el TESTIGO 2 (Véase Código de Comercio : arts. 1 y 3) Sus
Thématiques: Autisme: problématiques actuelles Questions de l'heure Les vitamines B6 (et le magnésium) dans le traitement de l'autisme Bernard Rimnland, Ph. D. (texte recueilli par Sylvie Ruest) À ma connaissance, chacune des douze études ayant fait l'objet d'une évaluation de la vitamine B6, en tant que traitement des enfants autistes, a conduit à des résultats positifs
 PRK With and Without Smoothing Using the Technolas 217C Laser/Serrao and Lombardo
PRK With and Without Smoothing Using the Technolas 217C Laser/Serrao and Lombardo