Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Doi:10.1016/s0736-4679(03)00044-
The Journal of Emergency Medicine, Vol. 24, No. 4, pp. 441– 447, 2003
doi:10.1016/S0736-4679(03)00044-1 Pharmacology in Emergency Medicine DROPERIDOL IN THE EMERGENCY DEPARTMENT: IS IT SAFE?
John R. Richards, MD* and Aaron B. Schneir, MD†
*Division of Emergency Medicine and Toxicology, University of California, Davis Medical Center, Sacramento, California and
†Department of Emergency Medicine, Division of Medical Toxicology, University of California, San Diego Medical Center, San Diego
Division, California Poison Control System, San Diego, California
Reprint Address: John R. Richards, MD, Division of Emergency Medicine, UC Davis Medical Center, 2315 Stockton Boulevard,
e Abstract—Droperidol is an antipsychotic and antiemetic
was more useful in the treatment of psychosis, and Hal-
drug that has been used extensively by Emergency Physi-
operidol was the first agent to be approved for this use in
cians, Psychiatrists, and Anesthesiologists worldwide since
1957 Droperidol has been used extensively for the
1967. It also has been used effectively for other diverse
past 30 years by Psychiatrists, Emergency Physicians,
conditions, such as treatment of headache and vertigo. As of
and Anesthesiologists. Recently, however, the drug has
January 2001, Droperidol was no longer available in Eu-
come under intense scrutiny for its role in prolonging QT
rope after its founder, Janssen-Cilag Pharmaceuticals, dis- continued its distribution. In December 2001, the United
intervals and development of fatal cardiac dysrhythmias
States Food and Drug Administration (FDA) placed a black
The Medicines Control Agency of the United
box warning on the use of Droperidol in response to an
Kingdom initially raised a safety concern regarding the
association between Droperidol and fatal cardiac dysrhyth-
chronic use of high-dose Droperidol in psychiatric pa-
mias, such as torsade de pointes, resulting from prolonga-
tients. This may have led its founding firm, Janssen-
tion of the QT interval. In this review we closely examine
Cilag Ltd of Belgium, to discontinue production and
the pharmacology, indications, use, and complications as-
distribution of Droperidol to most of the world as of
sociated with Droperidol, and speculate on its future use in
January 2001 This resulted in an outcry from
the Emergency Department. 2003 Elsevier Inc.
physicians in Europe, mainly anesthesiologists, who
used Droperidol extensively for postoperative nausea
Keywords—Droperidol; Inapsine; antipsychotic; Emer- gency Department; FDA warning
and vomiting (PONV) and remarked on its efficacy, lowcost, patient satisfaction, and excellent safety profile
INTRODUCTION
In December 2001, the United States Food and Drug
Administration (FDA) issued a “black box warning”
Droperidol is a butyrophenone, a class of antipsychotic
(Appendix), its most serious alert, on the use of Droperi-
agents that include Haloperidol, and is marketed in the
dol The Canadian Health Protection Branch followed
United States under the trade name Inapsine™. Butyro-
soon thereafter Before these warnings, doses greater
phenones were initially studied in the late 1950s at the
than 25 mg were considered to put patients at higher risk
Janssen laboratories in Belgium as a potential substitute
of QT prolongation and dysrhythmia, and it was esti-
for Morphine It was soon realized this class of drugs
mated Droperidol constituted 30% of the antiemetic mar-
Pharmacology in Emergency Medicine is coordinated by Richard F. Clark, MD, of the University of California San Diego Medical Center, San Diego, California
RECEIVED: 26 April 2002; FINAL SUBMISSION RECEIVED: 9 September 2002;ACCEPTED: 15 October 2002
erate doses During this sedation, the patient isresponsive to commands and is usually indifferent to hisor her surroundings. There is evidence Droperidol inhib-its specific GABA and nicotinic receptors in high doses,which may explain the anxiety, dysphoria, and akathisiathat accompanies high doses in certain patients
Droperidol is the shortest acting of the butyrophe-
nones, with a half-life of 2 h Peak serum levelsoccur 1 h after intramuscular (i.m.) and intravenous (i.v.)injection, and it is widely protein bound with a volume ofdistribution of 2 L/kg. Droperidol may be administeredorally, i.m., and i.v. Typical antiemetic doses range from0.625 to 2.5 mg i.v./i.m., and doses for chemical restraintbegin at 5 mg i.v./i.m. and higher. It readily crosses theblood-brain barrier and is distributed into the cerebrospi-nal fluid It slowly traverses the placenta, and it isunclear if it is present in breast milk It is exten-sively metabolized in the liver, and excretion is primarilyrenal (75%) with the remainder excreted in the feces. Itsmetabolites, benzimidazolone, p-fluorophenylacetic acid,and p-hydroxypiperidine, are inactive. Roughly 10% isexcreted in the urine unmetabolized
Figure 1. Chemical structure of Droperidol. INDICATIONS
ket, with over 25 million units sold in 2000 North
The most common indications for Droperidol use in the
American Anesthesiologists, Pharmacists, and Emer-
ED are for chemical restraint of acute psychosis and
gency Physicians reacted skeptically to these new restric-
agitation, and for antiemesis Of interest,
tions on the use of Droperidol Now Emergency
Droperidol has received FDA approval for only two
Physicians (EPs) who still have access to Droperidol
indications, as an antiemetic and as an anxiolytic/amnes-
must decide the risk/benefit ratio for its use in their
tic agent before diagnostic or surgical procedures for
particular practice. To aid in this decision, in this article
children and adults. Droperidol is a powerful and inex-
we extensively review the current and past literature
pensive antiemetic, as demonstrated by several studies
regarding Droperidol and its potential for adverse drug
However, it does not have FDA approval for
reactions in the Emergency Department (ED).
hyperemesis gravidarum and chemotherapy-inducednausea and vomiting, despite several studies demonstrat-ing its efficacy when compared to other alternative anti-
PHARMACOLOGY
Perhaps the most important use of Droperidol in the
Butyrophenones, of which Droperidol is a member, are
ED is rapid tranquilization of the violent, agitated patient
potent dopamine (D) antagonists with less potent ␣ re-
A plethora of studies has proven the efficacy of
ceptor effects. Droperidol binds preferentially to the D-2
Droperidol for this particular indication, especially when
and ␣-1 receptors, respectively Both its antiemetic
compared to other agents, such as benzodiazepines
and antipsychotic properties derive from this potent D-2
Furthermore, Droperidol has been effective for treat-
antagonism. Unlike the phenothiazines, butyrophenones
ing all subsets of agitation, including stimulant abuse,
have weaker anticholinergic and antihistaminic proper-
head injury, mania or psychosis, and in pediatric patients
ties, and greater tendency to produce extrapyramidal side
Unlike Haloperidol, Droperidol has never re-
effects. Structurally butyrophenones are sim-
ceived FDA approval for use in treatment of acute psy-
ilar to ␥-aminobutyric acid (GABA) and are concen-
trated in the central nervous system (CNS) This may
Droperidol, originally synthesized as a potential alter-
account for their potent tranquilization properties, in
native to Morphine, also has been used for atypical pain
which a quiescent state with reduced motor activity,
syndromes. Before the FDA warning, Droperidol had
anxiety, and apprehension is achieved with low to mod-
become increasingly popular for treatment of headache
Two recent studies demonstrated Droperidol to be
ported with Droperidol, but these phenomena seem to be
an effective agent in the treatment of benign headaches
very rare events Agranulocytosis was reported
in the ED In Europe, there has been interest in
in two patients after addition of Droperidol to an existing
the use of Droperidol in combination with Fentanyl for
phenothiazine regimen, but no further reports exist
cardiac chest pain, but results in one study have demon-strated higher 12 month mortality for unstable anginapatients receiving Droperidol and Fentanyl versus those
ADVERSE DRUG EFFECTS: CARDIAC
receiving Morphine A case study of Droperidoluse in a patient with neuropathic pain of central origin
After administration of Droperidol, tachycardia and mild
reported diminished lightning pain after subarachnoid
hypotension, presumably from ␣-1 antagonism, have
block In another study, patients undergoing anorec-
been reported, but these side effects are extremely rare
tal surgery received either Droperidol or Butorphanol as
Decreased left ventricular end diastolic pres-
an adjunct to epidural anesthesia, and the Droperidol
sure, but not cardiac contractility or systemic vascular
group had improved analgesia One explanation for
resistance, was noted after i.v. Droperidol administration
this phenomenon may be that Droperidol selectively
in a study of nine patients Droperidol’s effects on
blocks the fast sodium channels in the dorsal horn neu-
the ionic currents of the heart were recognized by
rons of the spinal cord Another indication for
Hauswirth in 1967 and by Kern and associates in 1971
Droperidol is the emergency treatment of peripheral ver-
This was followed by several studies that further
tigo, including Meniere’s disease and benign positional
defined Droperidol’s site of action The process
variants Two studies have demonstrated impressive
of repolarization of cardiac cells involves sodium, cal-
cium, and several different potassium channels Droperidol and many other antipsychotic drugs seemto delay repolarization of ventricular cells by blocking a
ADVERSE DRUG EFFECTS: NON-CARDIAC
specific type of channel, the potassium rectifier (I )
channel This is represented by QT interval
Droperidol has several CNS side effects that have been
prolongation on the electrocardiogram (EKG).
previously described. Dysphoria, drowsiness, hallucina-
Corrected QT intervals less than 440 ms in duration
tions, shivering, and anxiety have been reported after
are considered normal, and intervals greater than 500 ms
Droperidol injection, but are uncommon Extra-
are considered high risk Torsade de pointes is a
pyramidal side effects from Droperidol’s action on the
unique polymorphic ventricular dysrhythmia associated
D-2 receptor include akathisia and dystonias, such as
with a long QT interval, which is usually unresponsive to
torticollis, and oculogyric crisis Neuroleptic
standard antidysrhythmic drugs It exists in a
malignant syndrome after Droperidol administration has
primary congenital form, and in a secondary form that is
been described in patients on long-term antipsychotics,
most often drug induced Treatment of torsade de
such as Lithium and phenothiazines, and during elective
pointes typically involves i.v. magnesium and possibly
surgery under anesthesia The risk of Droperidol
cardioversion or cardiac pacing. Other risk factors in-
lowering threshold for seizure seems to be a common
clude hypomagnesemia, hypokalemia, pre-existing dys-
dogma, but there is little evidence for its support in the
rhythmia, history of cardiac or liver disease, or concom-
form of case reports or controlled studies One study
itant use of drugs known to inhibit hepatic metabolism of
in mice demonstrated low to moderate doses of Droperi-
Droperidol In a study of 55 patients, Guy and col-
dol lowered seizure threshold, whereas high doses para-
leagues injected 0.25 mg/kg i.v. Droperidol and noted
doxically raised it A report from Russia noted tonic
prolongation of the QT interval in 70% of subjects after
episodes resembling seizures in patients after receiving
1 min No one developed torsade de pointes in their
study, but they recommended caution with administra-
One of Droperidol’s most important advantages is its
tion of Droperidol. Reilly and associates compared
lack of respiratory depression even in high doses
EKGs between patients taking antipsychotics and
Only one case of respiratory distress has been described
healthy subjects Abnormal QT interval was asso-
after 5 mg i.v. Droperidol was given to a patient suffer-
ciated with older age, use of tricyclic antidepressants,
ing from lysergic acid (LSD) toxicity who had been
Thioridazine, Droperidol, or high doses of any antipsy-
taking Lithium and Risperidone After becoming
chotic. Lischke et al., in a series of 40 patients injected
rigid and unable to self-ventilate, he was intubated. It
with increasing dosages of Droperidol, determined a
was postulated by the authors that Droperidol may have
direct association between dose and QT interval prolon-
induced serotonin syndrome in this patient. Angioedema,
laryngospasm, and true allergic reactions have been re-
In their review of antipsychotics, Glassman and Big-
Table 1. Drugs That Prolong QT Interval or Induce Torsade de Pointes Figure 2. Types of receptors involved in the cardiac action potential and ionic flow. (a) Surface electrocardiogram. The QT interval is measured from the beginning of the QRS
* associated with prolonged QT and torsade de pointes. †
complex to the return of the T wave to the isoelectric base-
associated with torsade de pointes only. line. (b) Action potential showing the four phases of cardiac depolarization and repolarization with the various sites of the ion channel effects. I
؍ L-type calcium channel; I T-type calcium channel; I
cardiac deaths per 10,000 person-years in subjects with-
؍ depolarizing sodium channel;
؍ Inwardly rectifying potassium current; I
؍ rapidly
out cardiac disease, or 2.39 times greater risk of death
activating delayed rectifier potassium current; I
؍ slowly
than patients not taking antipsychotics. To date there
activating delayed rectifier potassium current; I rapidly activating delayed rectifier potassium current;
have been over 100 reports of cardiovascular events
؍ transient outward potassium currents. (c) Ion
attributed directly to Droperidol reported to the FDA,
current directions during activation of various ion channels.
including 20 cases of torsade de pointes, nine cardiac
EC, extracellular; IC, intracellular. (Reprinted with permis- sion, Buckley NA, Sander P. Cardiovascular adverse effects
arrests, and two deaths at doses of 2.5 mg i.v. or less
of antipsychotic drugs. Drug Saf. 2000;23:218. 2000 Adis)
Although evidence exists that Droperidol causes pro-
longation of the QT interval based on the aforementioned
ger emphasized that most members of this class of drugs
studies, it is difficult to ascertain whether Droperidol
cause QT interval prolongation Many other drugs
alone is at fault for the genesis of subsequent dysrhyth-
that prolong the QT interval, such as Amiodarone, are
mias, as patients who receive the drug often have con-
rarely associated with torsade de pointes Con-
comitant medical and psychiatric problems. Many case
versely, quinidine is more frequently associated with
reports describe patients undergoing elective and emer-
torsade de pointes despite less QT interval prolongation
gent surgery in the operating room under general anes-
The phenothiazine Thioridazine, in particular, seems
thesia Many of these patients also may have
to be the most dangerous of the antipsychotics for the
been taking cardiac and psychotropic medication. For
production of torsade de pointes and sudden death
instance, a recent case report involves a patient with
These dysrhythmias seem to be more pronounced in
chronic renal failure on hemodialysis who underwent a
elderly patients with heart disease, patients who smoke,
total hysterectomy under general anesthesia and devel-
and patients on multiple medications. The risk of sudden
oped a chaotic ventricular dysrhythmia Another
death from antipsychotic drug use was estimated by Ray
series involved three critically ill patients with esopha-
and associates in their study of half a million subjects
geal varices receiving vasopressin and nitroglycerin
over 2.5 years Their calculation was 11 sudden
The influence of general anesthetic agents combined
with Droperidol on development of dysrhythmias is un-
on adverse reactions. To avoid any risk of QT interval
clear One study reported no dysrhythmias in a
prolongation, the Emergency Physician is essentially left
group of patients receiving Enflurane and Droperidol for
with benzodiazepines and barbiturates as the only alter-
surgery compared to those receiving Enflurane and Hy-
natives for sedation. Although the FDA has recom-
oscine (0 vs. 4.4%, respectively) Furthermore, pa-
mended continuous cardiac monitoring for patients re-
tients requiring Droperidol may already be under the
ceiving Droperidol, our review demonstrates this may be
influence of stimulants such as Methamphetamine and
an overstatement of the risk. Although patients at higher
Cocaine, which are already prodysrhythmogenic In
risk for cardiac events, such as those with prior history of
their review of case reports involving Droperidol and
dysrhthmia and those receiving high doses of Droperidol,
Haloperidol, Lawrence and Nasraway found 11 reports
warrant consideration of continuous cardiac monitoring,
of 18 patients with conduction disturbances linked to buty-
many low-risk patients receiving small doses may not
rophenone use. Thirteen (72%) had a history of cardiovas-
require continuous cardiac monitoring. For those clini-
cular disease Of interest, Haloperidol does not have
cians who have come to rely on Droperidol and choose to
a black box warning by the FDA, even though it has the
continue using it, we recommend careful patient selec-
same cardiac effects as Droperidol and has been associ-
tion and screening for high-risk individuals, adherence to
ated with torsade de pointes To date, no case reports
the FDA guidelines, and continuous cardiac monitoring
involving cardiac dysrhythmia and Droperidol have ap-
of the high-risk patient after administration. An under-
peared in Emergency Medicine journals.
standing of the potential complications of Droperidol
The promise of improved patient safety with second
use, such as dystonia, torsade de pointes, and their treat-
generation antipsychotics such as Olanzapine, Risperi-
ments, will ultimately reduce potential liability and in-
done, Ziprasidone and Quetiapine has been questionable
Their safety profile may not be fully knownuntil these drugs have achieved widespread use, as ex-emplified by Sertindole, which was withdrawn after be-
REFERENCES
ing linked to 12 sudden deaths in Europe The newer
1. Bowman MC, Rand MJ. Textbook of pharmacology. Oxford:
antipsychotics also affect the QT interval, and most are
not available in an injectable form, thus limiting their use
2. Glassman AH, Bigger JT Jr. Antipsychotic drugs: prolonged QTc
in an acute care setting The same situation seems to
interval, torsade de pointes, and sudden death. Am J Psychiatry2001;158:1774 – 82.
apply to antiemetic drugs, as the newer serotonin antag-
3. SoRelle R. Warnings strengthened on tranquilizer inapsine
onists, such as Dolasetron, seem to affect the QT interval
(Droperidol). Circulation 2001;104:E9061–2.
as well and are considerably more expensive than
4. Haines J, Barclay P, Wauchob T. Optimising management of delir-
ium. Withdrawal of Droleptan (droperidol). BMJ 2001;322:1603.
5. Tramer MR, Reynolds DJ, Goodman NW. Whose drug is it any-
6. Lehot JJ, Ferry S. And now we present droperidol! Ann Fr Anesth
CONCLUSION
7. U.S. Food and Drug Administration. FDA strengthens warnings
for droperidol. FDA Talk Paper 2001;T01– 62.
For the past 3 decades, Droperidol has proven to be an
8. Wooltorton E. Droperidol: cardiovascular toxicity and deaths.
excellent antipsychotic and antiemetic agent with an
9. Gan TJ, White PF, Scuderi PE, Watcha MF, Kovac A. FDA “Black
extensive history of use in the ED. It also has been
Box” warning regarding use of droperidol for postoperative nausea
effectively utilized for headache and spinal-cord-medi-
and vomiting: is it justified? Anesthesiology 2002;97:287.
10. Ben-David B, Weber S, Chernus S. Droperidol “Black Box” warn-
ated pain syndromes, as well as for suppression of ver-
ing warrants scrutiny. Anesthesiology 2002;97:288.
tigo. It is inexpensive, rapid acting, efficacious, and has
11. Bailey P, Norton R, Karan S. The FDA Droperidol warning: is it
a short half-life. Droperidol does not cause respiratory
justified? Ansesthesiology 2002;97:288 –9.
12. Young D. Black box warning for droperidol surprises pharmacists.
depression even in high doses, and has equivalent i.m.
Am J Health Syst Pharm 2002;59:502– 4.
and i.v. dosing. Despite the powerful advantages of
13. Horowitz BZ, Bizovi K, Moreno R. Droperidol— behind the black
Droperidol, the risk of prolonged QT interval and torsade
box warning. Acad Emerg Med 2002;9:615– 8.
14. Heyer EJ, Flood P. Droperidol suppresses spontaneous electrical
de pointes does exist. Furthermore, it seems many other
activity in neurons cultured from ventral midbrain. Implications for
unrelated drugs have this risk as well but most
neuroleptanesthesia. Brain Res 2000;863:20 – 4.
do not carry an FDA black box warning.
15. Flood P, Coates K. Droperidol inhibits GABA
nicotinic receptor activation. Anesthesiology 2002;96:987–93.
There are several alternative drugs available to the
16. Lener ME, Velasquez N, Watson WA. Droperidol for radiologic
Emergency Physician for treatment of nausea and eme-
procedures. Semin Interv Radiol 1987;4:179 – 82.
sis, but far fewer for the control of psychosis and agita-
17. Cressman WA, Plostnieks J, Johnson PC. Absorption, metabolism
and excretion of droperidol by human subjects following intramuscu-
tion. It seems likely that Haloperidol will also receive a
lar and intravenous administration. Anesthesiology 1973;38:363–9.
black box warning from the FDA given its current focus
18. Lehmann KA, Van Peer A, Ikonomakis M, Gasparini R, Heykants
J. Pharmacokinetics of droperidol in surgical patients under differ-
clinical outcomes in unstable angina patients. Cardiovasc Drugs
ent conditions of anaesthesia. Br J Anaesth 1988;61:297–301.
19. Soudijn W, Van Wijngaarden I, Allewijn F. Distribution, excretion
43. Wajima Z, Shitara T, Inoue T, Ogawa R. Severe lightning pain
and metabolism of neuroleptics of the butyrophenone type. I. Excre-
after subarachnoid block in a patient with neuropathic pain of central
tion and metabolism of haloperidol and nine related butyrophenone-
origin: which drug is best to treat the pain? Clin J Pain 2000;16:265–9.
derivatives in the Wistar rat. Eur J Pharmacol 1967;1:47–57.
44. Kotake Y, Matsumoto M, Ai K, Morisaki H, Takeda J. Additional
20. Cure S, Carpenter S. Droperidol for acute psychosis. Cochrane
droperidol, not butorphanol, augments epidural fentanyl analgesia
Database Syst Rev 2001;(2).CD002830.
following anorectal surgery. J Clin Anesth 2000;12:9 –13.
21. Eberhart LH, Morin AM, Bothner U, Georgieff M. Droperidol and
45. Olschewski A, Brau ME, Hempelmann G, Vogel W, Safronov BV.
5-HT3-receptor antagonists, alone or in combination, for prophy-
Differential block of fast and slow inactivating tetrodotoxin-sen-
laxis of postoperative nausea and vomiting. A meta-analysis of ran-
sitive sodium channels by droperidol in spinal dorsal horn neurons.
domised controlled trials. Acta Anaesthesiol Scand 2000;44:1252–7.
22. Macario A, Chung A, Weinger MB. Variation in practice patterns
46. Baldwin RL. Droperidol in the treatment of vertigo. South Med J
of anesthesiologists in California for prophylaxis of postoperative
nausea and vomiting. J Clin Anesth 2001;13:353– 60.
47. Johnson WH, Fenton RS, Evans A. Effects of droperidol in man-
23. Rizzo J, Bernstein D, Gress F. A randomized double-blind placebo-
agement of vestibular disorders. Laryngoscope 1976;86:946 –54.
controlled trial evaluating the cost-effectiveness of droperidol as a
48. Irving C, Richman PB, Kaiafas C, Eskin B, Ritter A, Allegra J.
sedative premedication for EUS. Gastrointest Endosc 1999;50:
Droperidol for the treatment of acute peripheral vertigo. Am J
24. Hill RP, Lubarsky DA, Phillips-Bute B, et al. Cost-effectiveness of
49. Yotsui H, Matsunaga M, Katori K, Kohno S, Higa K. Extrapyra-
prophylactic antiemetic therapy with ondansetron, droperidol, or
midal reactions after epidural droperidol. Masui 2000;49:1152– 4.
placebo. Anesthesiology 2000;92:958 – 67.
50. Hung YC, Ho YY, Shen CL. Delayed akathisia and suicidal
25. Lim BS, Pavy TJ, Lumsden G. The antiemetic and dysphoric
attempts following epidural droperidol infusion—a case report.
effects of droperidol in the day surgery patient. Anaesth Intensive
Acta Anaesthesiol Sin 1999;37:151– 4.
51. Gelenberg AJ. Major complications of neuroleptic drug use. West
26. Kreisler NS, Spiekermann BF, Ascari CM, et al. Small-dose
droperidol effectively reduces nausea in a general surgical adult
52. Bamrah JS. Neuroleptic-induced pyrexia. A benign variant. J Nerv
patient population. Anesth Analg 2000;91:1256 – 61.
27. Fukushima Y, Satoh M, Yasuda S, Zenfuku M, Shigematsu T.
53. Ratan DA, Smith AH. Neuroleptic malignant syndrome secondary
to droperidol. Biol Psychiatry 1993;34:421–2.
Continuous epidural administration of droperidol for the preven-
54. Edgar J. Droperidol-induced neuroleptic malignant syndrome.
tion of postoperative nausea. Masui 2001;50:1004 – 8.
28. Kelley SL, Braun TJ, Meyer TJ, Rempel P, Pearlman NW. Trial of
55. So PC. Neuroleptic malignant syndrome induced by droperidol.
droperidol as an antiemetic in cisplatin chemotherapy. Cancer
56. Hashem A, Frey HH. The effect of neuroleptics and neuroleptic/
29. Nageotte MP, Briggs GG, Towers CV, Asrat T. Droperidol and
analgesic combinations on the sensitivity to seizures in mice.
diphenhydramine in the management of hyperemesis gravidarum.
Am J Obstet Gynecol 1996;174:1801–5.
57. Rodin GD. Convulsion syndrome, simulating tetanus, during treat-
30. Richards JR, Derlet RW, Duncan DR. Chemical restraint for the
ment with droperidol and haloperidol. Sov Med 1974;11:149 –50.
agitated patient in the emergency department: lorazepam versus
58. Prokocimer P, Delavault E, Rey F, Lefevre P, Mazze RI, Desmonts
droperidol. J Emerg Med 1998;16:567–73.
JM. Effects of droperidol on respiratory drive in humans. Anes-
31. Thomas H Jr, Schwartz E, Petrilli R. Droperidol versus haloperidol
for chemical restraint of agitated and combative patients. Ann
59. Heard K, Daly FF, O’Malley G, Rosen N. Respiratory distress after
use of droperidol for agitation. Ann Emerg Med 1999;34:410 –1.
32. Chambers RA, Druss BG. Droperidol: efficacy and side effects in
60. Corke P, Murray G. Angioedema with droperidol. Anaesth Inten-
psychiatric emergencies. J Clin Psychiatry 1999;60:664 –7.
33. Brown ES, Dilsaver SC, Bowers TC, Swann AC. Droperidol in the
61. Palombaro JF, Klingelberger CE. Angioedema associated with
interim management of severe mania: case reports and literature
droperidol administration. Ann Emerg Med 1996;27:379 – 81.
review. Clin Neuropharmacol 1998;21:316 – 8.
62. Young A, Kehoe R. Two cases of agranulocytosis on addition of a
34. Hick JL, Mahoney BD, Lappe M. Prehospital sedation with intramus-
butyrophenone to a long-standing course of phenothiazine treat-
cular droperidol: a one-year pilot. Prehosp Emerg Care 2001;5:391– 4.
ment. Br J Psychiatry 1989;154:710 –2.
35. Hameer O, Collin K, Ensom MH, Lomax S. Evaluation of droperi-
63. van Nueten JM, Reneman RS, Janssen PA. Specific alpha-adreno-
dol in the acutely agitated child or adolescent. Can J Psychiatry
ceptor blocking effect of droperidol on isolated smooth muscles.
36. Joshi PT, Hamel L, Joshi ART, Capozzoli JA. Use of droperidol in
64. Bustamante R, Valverde A. Determination of a sedative dose and
hospitalized children. J Am Acad Child Adolesc Psychiatry 1998;
influence of droperidol and midazolam on cardiovascular function
in pigs. Can J Vet Res 1997;61:246 –50.
37. Stanislav SW, Childs A. Evaluating the usage of droperidol in
65. Aminoff MJ, Jaffe RA, Sampson SR, Vidruk EH. Effects of
acutely agitated persons with brain injury. Brain Inj 2000;14:261–5.
droperidol on activity of carotid body chemoreceptors in cat. Br J
38. Vinson DR. Treatment patterns of isolated benign headache in US
emergency departments. Ann Emerg Med 2002;39:215–22.
66. Marty J, Nitenberg A, Blanchet F, Laffay N, Mazze RI, Desmonts
39. Miner JR, Fish SJ, Smith SW, Biros MH. Droperidol vs. prochlor-
JM. Effects of droperidol on left ventricular performance in hu-
perazine for benign headaches in the emergency department. Acad
mans. Anesthesiology 1982;57:22–5.
67. Hauswirth O. Effects of dehydrobenzperidol (Droperidol) on elec-
40. Richman PB, Allegra J, Eskin B, et al. A randomized clinical trial
tric processes in the sheep Purkinje fibers. Helv Physiol Pharmacol
to assess the efficacy of intramuscular droperidol for the treatment
of acute migraine headache. Am J Emerg Med 2002;20:39 – 42.
68. Kern R, Einwachter HM, Haas HG, Lack EG. Cardiac membrane
41. Graf J, Janssens U. Therapy of angina pectoris: morphine or
currents as affected by an neuroleptic agent: Droperidol. Pflu¨gers
thalamonal? Dtsch Med Wochenschr 2001;126:572–3.
42. Burduk P, Guzik P, Piechocka M, et al. Comparison of fentanyl
69. Greene MJ. Some aspects of the pharmacology of droperidol. Br J
and droperidol mixture (neuroleptanalgesia II) with morphine on
70. Den Hertog A, Kleine JW. The effect of droperidol on mammalian
Derlet RW. Methamphetamine abuse and emergency department
non-myelinated nerve fibres. Eur J Pharmacol 1973;21:1–5.
utilization. West J Med 1999;170:198 –202.
71. Mironneau C, Mironneau J, Grosset A. Action of droperidol on the
95. Hunt N, Stern TA. The association between intravenous haldol and
ionic currents and the contraction of the sino-auricular fiber of frogs.
torsade de pointes. Psychosomatics 1995;36:541–9.
Study of its anti-arrhythmic properties. J Physiol Paris 1975;70:27–39.
96. FDA Briefing Document for Zeldox Capsules (Ziprasidone). New
72. Carmeliet E, Xhonneux R, Van-Glabbeek A, Reneman R. Electro-
York, Pfizer Inc., July 18, 2000, p.22.
physiological effects of droperidol in different cardiac tissues.
97. Kantor GS. Arrhythmia risk of antiemetic agents. Anesthesiology
Naunyn Schmiedebergs Arch Pharmacol 1976;293:57– 66.
73. Dorticos FR, Garcia-Barreto D. Electrophysiological effects of
droperidol on sinoatrial nodal fibers. Arch Int Pharmacodyn Ther1979;240:137– 42. APPENDIX
74. Gomez-Arnau J, Marquez-Montes J, Avello F. Fentanyl and droperi-
dol effects on the refractoriness of the accessory pathway in the
FDA black box warning for use of Droperidol
Wolff-Parkinson-White syndrome. Anesthesiology 1983;58:307–13.
75. Nashan B, Inoue K, Arndt JO. Droperidol inhibits cardiac vagal
efferents in dogs. Br J Anaesth 1984;56:1259 – 66.
76. Adamantidis MM, Kerram P, Caron JF, Dupuis BA. Droperidol
exerts dual effects on repolarization and induces early afterdepo-
Cases of QT prolongation and/or torsades de
larizations and triggered activity in rabbit Purkinje fibers. J Phar-
pointes have been reported in patients receiving INAPSINE at doses at or below recommended doses.
77. Drolet B, Zhang S, Deschenes D, et al. Droperidol lengthens
cardiac repolarization due to block of the rapid component of the
Some cases have occurred in patients with no known
delayed rectifier potassium current. J Cardiovasc Electrophysiol
risk factors for QT prolongation and some cases have been fatal.
78. Buckley NA, Sanders P. Cardiovascular adverse effects of anti-
psychotic drugs. Drug Saf 2000;23:215–28.
Due to its potential for serious proarrhythmic effects
79. Witchel HJ, Hancox JC. Familial and acquired long qt syndrome
and death, INAPSINE should be reserved for use in the
and the cardiac rapid delayed rectifier potassium current. Clin Exp
treatment of patients who fail to show an acceptable
Pharmacol Physiol 2000;27:753– 66.
80. Khan IA. Long QT syndrome: diagnosis and management. Am
response to other adequate treatments, either because of
insufficient effectiveness or the inability to achieve an
81. Gury C, Canceil O, Iaria P. Antipsychotic drugs and cardiovascular
effective dose due to intolerable adverse effects from
safety: current studies of prolonged QT interval and risk of ven-
those drugs (see Warnings, Adverse Reactions, Contra-
tricular arrhythmia. Encephale 2000;26:62–72.
82. Lawrence KR, Nasraway SA. Conduction disturbances associated
with administration of butyrophenone antipsychotics in the critically
Cases of QT prolongation and serious arrhythmias
ill: a review of the literature. Pharmacotherapy 1997;17:531–7.
(e.g., torsades de pointes) have been reported in patients
83. Guy JM, Andre-Fouet X, Porte J, Bertrand M, Lamaud M, Ver-
neyre H. Torsades de pointes and prolongation of the duration of
treated with INAPSINE. Based on these reports, all pa-
QT interval after injection of droperidol. Ann Cardiol Angeiol
tients should undergo a 12-lead ECG prior to adminis-
tration of INAPSINE to determine if a prolonged QT
84. Reilly JG, Ayis SA, Ferrier IN, Jones SJ, Thomas SH. QTc-
interval abnormalities and psychotropic drug therapy in psychiatric
interval (i.e., QTc greater than 440 msec for males or 450
patients. Lancet 2000;355:1048 –52.
msec for females) is present. If there is a prolonged QT
85. Lischke V, Behne M, Doelken P, Schledt U, Probst S, Vettermann
interval, INAPSINE should NOT be administered. For
J. Droperidol causes a dose-dependent prolongation of the QT
patients in whom the potential benefit of INAPSINE
interval. Anesth Analg 1994;79:983– 6.
86. Ray WA, Meredith S, Thapa PB, Meador KG, Hall K, Murray KT.
treatment is felt to outweigh the risks of potentially
Antipsychotics and the risk of sudden cardiac death. Arch Gen
serious arrhythmias, ECG monitoring should be per-
formed prior to treatment and continued for 2–3 hours
87. Neergaard L. FDA issues strong warning for anesthesia drug.
after completing treatment to monitor for arrhythmias.
88. Hauben M. Sudden death in a patient taking antipsychotic drugs.
INAPSINE is contraindicated in patients with known
or suspected QT prolongation, including patients with
89. Shigeyama T, Yanagidani T. Droperidol causes multifocal ventric-
ular dysrhythmias. Masui 2002;51:53–5.
90. Faigel DO, Metz DC, Kochman ML. Torsade de pointes compli-
INAPSINE should be administered with extreme cau-
cating the treatment of bleeding esophageal varices: association
tion to patients who may be at risk for development of
with neuroleptics, vasopressin, and electrolyte imbalance. Am J
prolonged QT syndrome (e.g., congestive heart failure,
91. Hochwarter J, Spiegl F, Karausz A, Ekhart W. 2 cases of brief
bradycardia, use of a diuretic, cardiac hypertrophy, hy-
asystole following premedication—a possible connection with
pokalemia, hypomagnesemia, or administration of other
Thalamonal? Anaesthesist 1989;38:629 –30.
drugs known to increase the QT interval). Other risk
92. Whalley DG, Tidnam PF, Tyrrell MF, Thompson DS. A compar-
ison of the incidence of cardiac arrhythmia during two methods of
factors may include age over 65 years, alcohol abuse,
anaesthesia for dental extractions. Br J Anaesth 1976;48:1207–10.
and use of agents such as benzodiazepines, volatile an-
93. Smith DC, O’Connell P. Cardiac dysrhythmias during oral surgery.
esthetics, and IV opiates. Droperidol should be initiated
Comparison of hyoscine and droperidol premedication. Anaesthe-sia 1986;41:745– 8.
at a low dose and adjusted upward, with caution, as
94. Richards JR, Bretz SW, Johnson EB, Turnipseed SD, Brofeldt BT,
needed to achieve the desired effect.
Hugo Pena Brandão e Carla Patricia Bahry Gestão por competências: métodos e técnicas para mapeamento de competências Hugo Pena Brandão e Carla Patricia Bahry Introdução A gestão por competências tem sido apontada como modelo gerencialalternativo aos instrumentos tradicionalmente utilizados pelas organizações. Baseando-se no pressuposto de que o domínio de certos
MATERIAL SAFETY DATA SHEET HOLDIT S57 SECTION 1. IDENTIFICATION OF THE MATERIAL AND SUPPLIER Product Name : HOLDIT S57 Other Names: Instant Pipe Seal with Teflon Part Number: S57-50 (50ml), S57-250 (250ml) Supplier: Address : Emergency Tel: Telephone: Emergency Contact Address: Other Information : The information below is belie
 The Journal of Emergency Medicine, Vol. 24, No. 4, pp. 441– 447, 2003
doi:10.1016/S0736-4679(03)00044-1
The Journal of Emergency Medicine, Vol. 24, No. 4, pp. 441– 447, 2003
doi:10.1016/S0736-4679(03)00044-1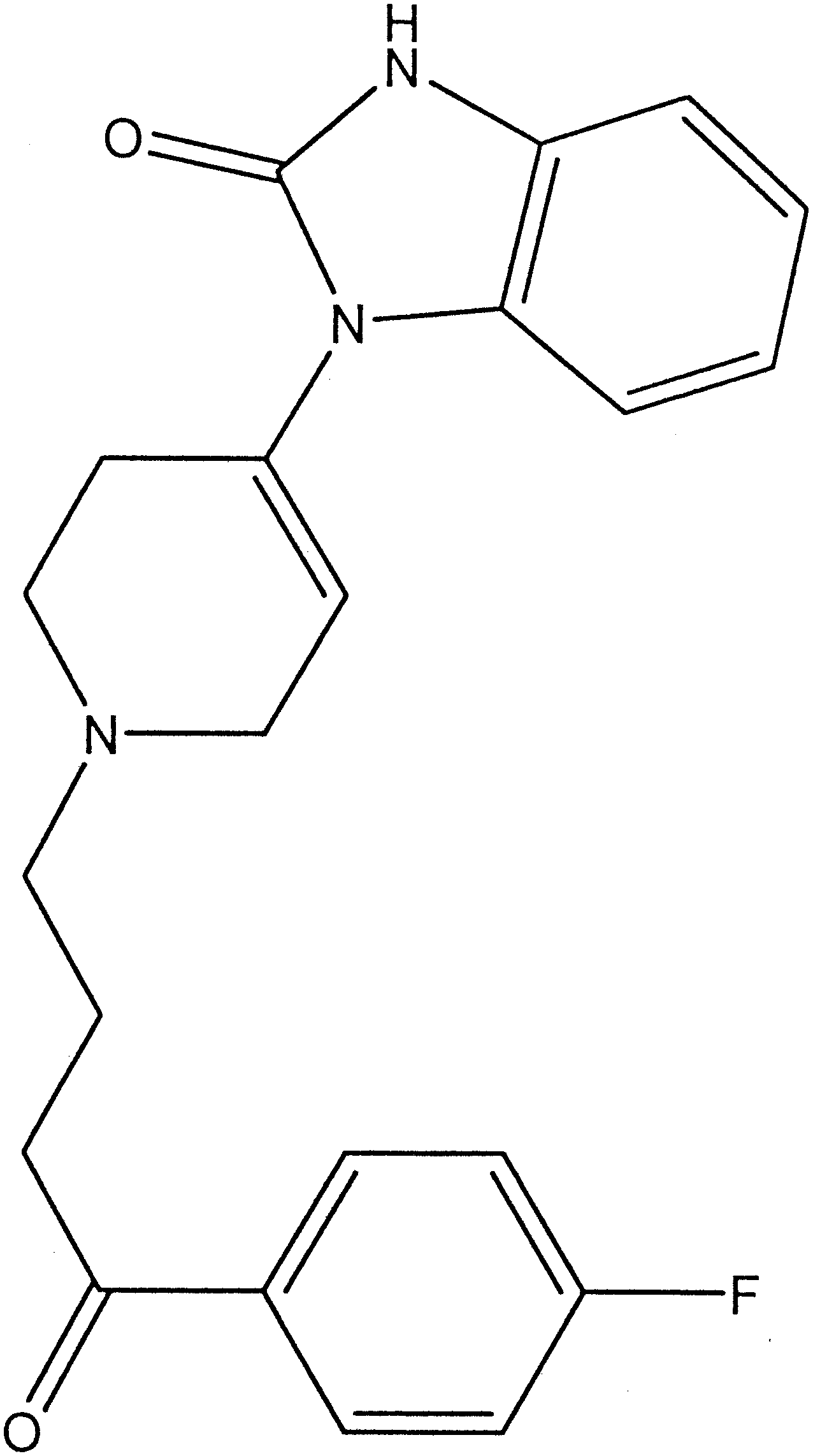 erate doses During this sedation, the patient isresponsive to commands and is usually indifferent to hisor her surroundings. There is evidence Droperidol inhib-its specific GABA and nicotinic receptors in high doses,which may explain the anxiety, dysphoria, and akathisiathat accompanies high doses in certain patients
Droperidol is the shortest acting of the butyrophe-
nones, with a half-life of 2 h Peak serum levelsoccur 1 h after intramuscular (i.m.) and intravenous (i.v.)injection, and it is widely protein bound with a volume ofdistribution of 2 L/kg. Droperidol may be administeredorally, i.m., and i.v. Typical antiemetic doses range from0.625 to 2.5 mg i.v./i.m., and doses for chemical restraintbegin at 5 mg i.v./i.m. and higher. It readily crosses theblood-brain barrier and is distributed into the cerebrospi-nal fluid It slowly traverses the placenta, and it isunclear if it is present in breast milk It is exten-sively metabolized in the liver, and excretion is primarilyrenal (75%) with the remainder excreted in the feces. Itsmetabolites, benzimidazolone, p-fluorophenylacetic acid,and p-hydroxypiperidine, are inactive. Roughly 10% isexcreted in the urine unmetabolized
Figure 1. Chemical structure of Droperidol.
erate doses During this sedation, the patient isresponsive to commands and is usually indifferent to hisor her surroundings. There is evidence Droperidol inhib-its specific GABA and nicotinic receptors in high doses,which may explain the anxiety, dysphoria, and akathisiathat accompanies high doses in certain patients
Droperidol is the shortest acting of the butyrophe-
nones, with a half-life of 2 h Peak serum levelsoccur 1 h after intramuscular (i.m.) and intravenous (i.v.)injection, and it is widely protein bound with a volume ofdistribution of 2 L/kg. Droperidol may be administeredorally, i.m., and i.v. Typical antiemetic doses range from0.625 to 2.5 mg i.v./i.m., and doses for chemical restraintbegin at 5 mg i.v./i.m. and higher. It readily crosses theblood-brain barrier and is distributed into the cerebrospi-nal fluid It slowly traverses the placenta, and it isunclear if it is present in breast milk It is exten-sively metabolized in the liver, and excretion is primarilyrenal (75%) with the remainder excreted in the feces. Itsmetabolites, benzimidazolone, p-fluorophenylacetic acid,and p-hydroxypiperidine, are inactive. Roughly 10% isexcreted in the urine unmetabolized
Figure 1. Chemical structure of Droperidol.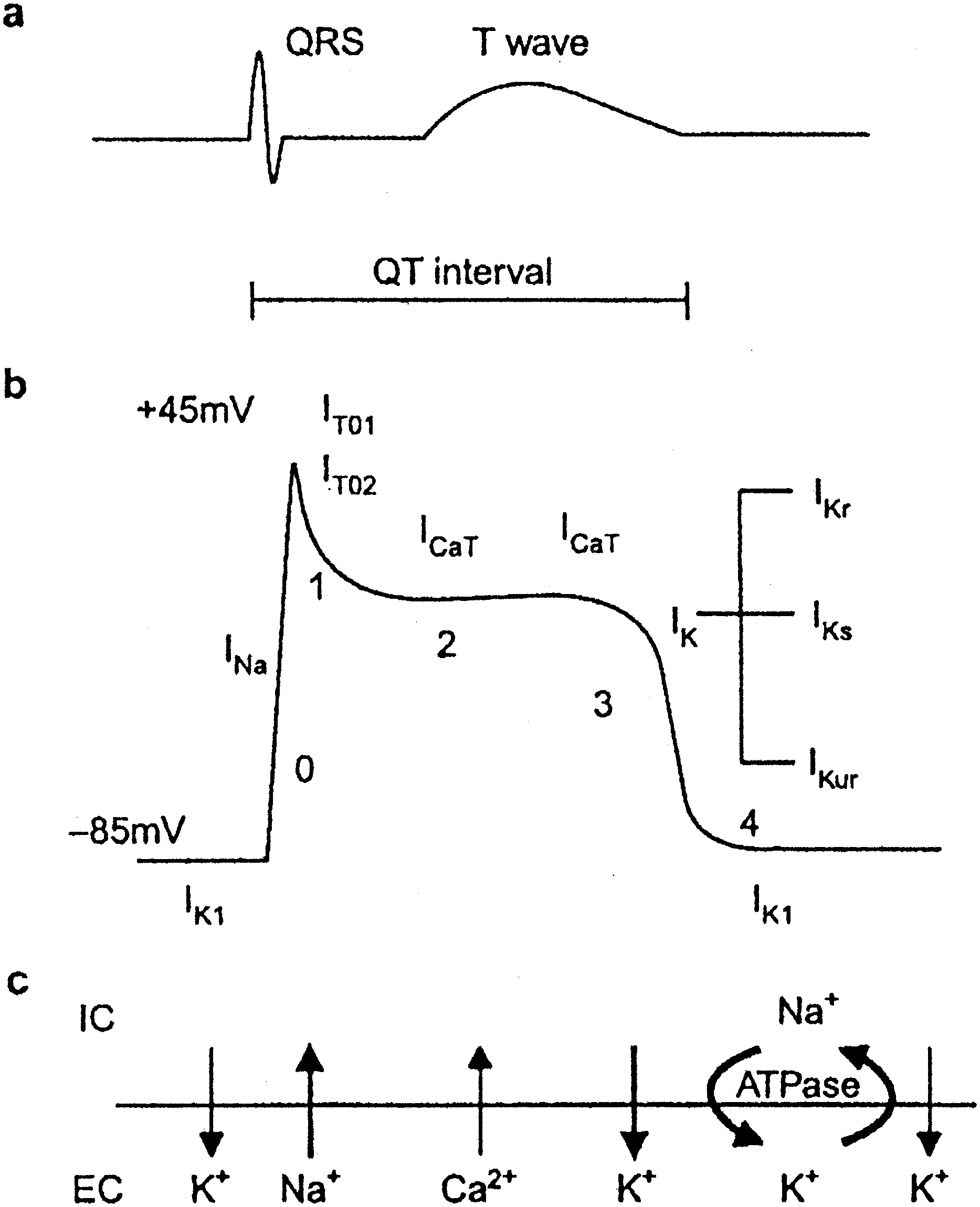 Table 1. Drugs That Prolong QT Interval or Induce Torsade
Table 1. Drugs That Prolong QT Interval or Induce Torsade