Comparison of the effect of valsartan and lisinopril on autonomic nervous system activity in chronic heart failure Elisabetta De Tommasi, MD,a,b Massimo Iacoviello, MD,a,b Roberta Romito, MD,c Claudio Ceconi, MD,d Pietro Guida, MS,a,b Francesco Massari, MD,c Gloria Francolini, BSc,d Federico Bertocchi, MD,e Roberto Ferrari, MD,f Paolo Rizzon, MD,a,b and Maria Vittoria Pitzalis, MD, PhDa,b Bari, Italy Background In chronic heart failure (CHF), the derangement of autonomic nervous system activity has a deep im- pact on the progression of the disease. It has been demonstrated that modulation of the renin-angiotensin aldosterone sys- tem (RAAS) increases autonomic control of heart rate and reduces adrenergic activity. We sought to evaluate, in CHF, the different effects of an ACE inhibitor (lisinopril) and of an AT1 receptor antagonist (valsartan) on heart rate variability, baroreflex sensitivity and norepinephrine plasma levels. Methods Ninety patients (61 Ϯ 10 years, 2.3 Ϯ 0.5, New York Heart Association class) with CHF and left ventricu- lar ejection fraction Ͻ40% were randomly assigned in a double-blind fashion to receive lisinopril (uptitrated to 20 mg/d) or valsartan (uptitrated to 160 mg/d) therapy for 16 weeks. Heart rate variability (evaluated by measuring standard devi- ation of normal R-R intervals on 24-hour ECG recordings), spontaneous baroreflex sensitivity and aldosterone and norepi- nephrine plasma levels were assessed before and after drug therapy. Results There were no significant differences between valsartan and lisinopril in their effects on left ventricular func- tion, arterial pressure, aldosterone plasma levels and autonomic control of heart rate. Both lisinopril and valsartan signifi- cantly reduced plasma norepinephrine levels, but the reduction induced by valsartan was significantly greater than that observed for lisinopril (27% vs 6%, P Ͻ .05). Conclusions This study shows a comparable effect of ACE inhibition (lisinopril) and of AT1 receptor antagonism (valsartan) on cardiac vagal control of heart rate, whereas valsartan has shown a more effective modulation of sympa- thetic activity measured by plasma norepinephrine levels. (Am Heart J 2003;146:e17.)
Autonomic nervous system activity plays a pivotal
derangement occurring in the setting of CHF pro-
pathophysiologic role in the progression of chronic
In particular, the renin-angiotensin-aldo-
heart failure (CHF), and impairments in the parameters
sterone system (RAAS), which plays a key role in
reflecting its function have been shown to predict a
CHF pathophysiology, has been demonstrated to in-
fluence largely autonomic nervous system
evident with regard to heart rate barore-
Angiotensin II (ATII) and aldosterone are able to en-
Autonomic nervous system abnormality is, at least
and RAAS blunting is able to modulate the auto-
in part, the result of the complex neurohormonal
nomic nervous system balance In pa-tients with CHF, the level of RAAS modulation, thatis, ACE inhibition or AT1 receptor antagonism, is
From aInstitute of Cardiology, University of Bari, Bari, bInnovative Technologies for Sig-nal Detection and Processing Center, University of Bari, cCardiology, “SalvatoreMaugeri” Foundation, IRCCS, Cassano, dFondazione Salvatore Maugeri, Clinica del
ever, the administration of an AT1 receptor antago-
Lavoro e della Riabilitazione, IRCCS, Cardiovascular Pathophysiology Research Cen-
nist in addition to prescribed CHF therapy, includ-
ter, Gussago, Brescia, eNovartis Pharma, Origgio, Varese, and fUniversity of Ferrara,Cardiology and Intensive Cardiology Care Unit, S. Anna Hospital, Ferrara.Submitted December 10, 2002; accepted March 10, 2003.
of a different autonomic effect but synergistic activ-
Reprint requests: Maria Vittoria Pitzalis, MD, PhD, FESC, Institute of Cardiology-Univer-sity of Bari, Piazza Giulio Cesare 11, 70124 Bari, Italy.
ity of these interventions. However, up to now it
E-mail: [email protected]
has not been convincingly demonstrated that the
2003, Mosby, Inc. All rights reserved.
two classes of drugs have a different effect on auto-
0002-8703/2003/$30.00 ϩ 0doi:10.1067/S0002-8703(03)00366-12 De Tommasi et al
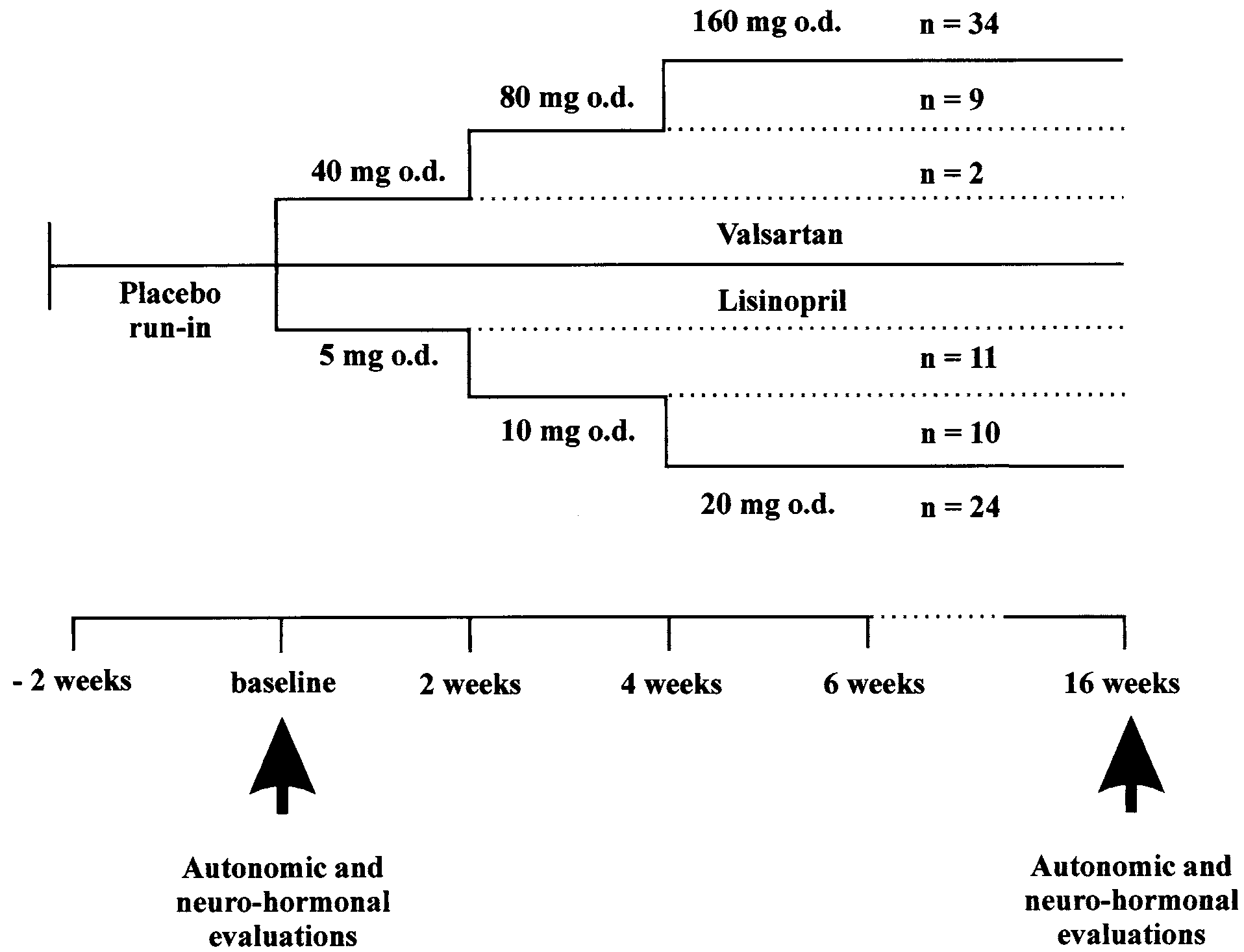
After the first visit, eligible patients entered a single-blind
placebo run-in period and received placebo, 1 capsule dailyfor 2 weeks. At the second visit, patients were randomly as-signed to receive valsartan or lisinopril, both orally adminis-tered with forced titration for 6 weeks, in a double-blindfashion. During the first 6 weeks, the dose was increased ev-ery 2 weeks for valsartan (40 mg/d, 80 mg/d, and 160 mg/d)as well as for lisinopril (5 mg/d, 10 mg/d, and 20 The maximum tolerated dose was administered for a further10 weeks.
Once-daily dosing of valsartan and forced titration was cho-
sen on the basis of the safety demonstrated in phase II trials,because the study design was planned before phase III stud-ies. Lisinopril has been chosen as one of the most used drugsin the indication CHF, with a dose-titration similar to thatadopted in the Multicentre Lisinopril-Captopril CongestiveHeart Failure Study Group
At the second and final visits, heart rate variability, barore-
flex sensitivity (BRS), and aldosterone and norepinephrineplasma values were assessed
Study design and patient dosage details according to studyprogress. Heart rate variability. The measurements were obtained
by means of 24-hour ECG recordings (Del Mar AvionicsModel 445A, Irvine, Calif), which were analyzed by using an
Therefore, the aim of the current study was to evalu-
ELA Medical system (Elatec System, Montrouge, France) to
ate whether in patients with stable CHF, AT1 receptor
measure the mean normal R-R cycle length (NN) and the
antagonism and ACE inhibition lead to a differential
standard deviation of normal R-R intervals (SDNN). The ECG
modulation of the autonomic control of heart rate and
recordings Ͻ16 hours in duration or with Ͻ90% of the re-cording suitable for analysis were
Arterial baroreflex sensitivity. Spontaneous BRS was as-
sessed by using sequence (BRS-Seq; ms/mm Hg) and spectral
(BRS-Spec; ms/mm Hg) Time series of fingerarterial blood pressure and heart rate signals recorded during
10 minutes of metronome-guided respiration at 0.25 Hz were
The study was conducted in accordance with good clinical
analyzed. The BRS-Seq was calculated by the slope of the re-
practice and the Declaration of Helsinky. The study was ap-
gression line (if r Ն0.80) between systolic pressure and R-R
proved by the local Committee on Medical Ethics, and all
interval changes (ie, either a progressive rise in systolic pres-
patients gave their written informed consent.
sure and lengthening in R-R interval or a decrease in systolicpressure and shortening in R-R interval). The BRS-Spec was
calculated as the square root ratio of the R-R interval and sys-tolic pressure in the respiratory band, when squared coher-
This study was a randomized, double-blind, forced-titration,
ence function between the two signals was Ͼ0.5.
parallel-group, active-controlled trial. Eligible patients were18 to 80 years of age, with CHF (New York Heart Associationclass II-IV) beginning at least 3 months before the first visit.
Other inclusion criteria were sinus rhythm and left ventricu-
Venous blood samples were drawn after 30 minutes of su-
lar ejection fraction Ͻ40% by 2-dimensional echocardiogra-
phy within 2 weeks before the first visit. The patients should
Plasma aldosterone measurement. Samples (2.5 mL) were
have not received an ACE inhibitor or an ATII receptor antag-
collected in plastic tubes without anticoagulant. They were
onist or a -blocker during the last month before the first
left to coagulate at room temperature for approximately 1
visit. During the 2 weeks of placebo run-in period, CHF med-
hour and then centrifuged at room temperature for 15 min-
ications were at a stable dosage regimen and patients were in
utes at 1700g. The serum was stored at Ϫ20°C. Plasma aldo-
stable clinical condition. Exclusion criteria were history of
sterone levels were measured by competitive radioimmunoas-
heart transplantation, myocardial infarction or cardiac surgery
say (RADIM cod KS17CT Spa Pomezia-RO-Italy). Intra-assay
within the past 3 months, unstable angina, need of revascu-
coefficient of variation was: 6.6% to 8.6%; interassay coeffi-
larization procedures, syncopal episodes, sustained ventricu-
cient of variation was: 8.4% to 9.4%.
lar arrhythmia within the past 3 months, and hypersensitivity
Plasma norepinephrine measurement. Samples (5 mL)
or contraindication to ATII receptor antagonists or ACE inhib-
were collected in prerefrigerated tubes containing 125 L
EDTA bisodium (5%) and 75 L of sodium metabisulphite
De Tommasi et al 3
(Na S O 10 mM), immediately placed on ice, and then cen-
Table I. Clinical characteristics of randomized population
trifuged at 4°C for 15 minutes at 1700g. Plasma was stored atϪ70°C. Norepinephrine measurements were performed by
Lisinopril Valsartan
high-performance liquid chromatography.
Data are related to intention-to-treat population. The effect
of the two drugs on the studied variables was assessed by
using the Student t test for dependent samples or Wilcoxon
test when appropriated. Demonstration of a difference be-
tween valsartan and lisinopril on variables with normal distri-
bution was assessed by means of analysis of covariance on
the last measured parameters, considering the study treat-
ment as factor and baseline values as covariate. Demonstra-
tion of a different effect on non-normal variables was as-
sessed through comparison of percentage variations between
final and baseline values. Continuous variables were ex-
pressed as mean and standard deviation. The tests were con-
sidered significant for P Ͻ .05. All statistical tests were per-
Among the 95 eligible patients, 90 were randomly
assigned, 45 for each group. Baseline characteristics of
patients and the causes of discontinuation are shown
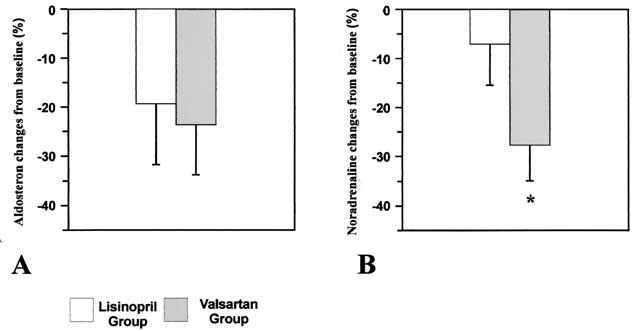
percentage reduction in norepinephrine levels caused
by valsartan was significantly greater than that caused
two groups in terms of baseline clinical characteristics.
Baseline BRS-spec and baseline BRS-seq were analyz-able in 53 of 90 and 85 of 90 patients, respectively (PDiscussion
The renin-angiotensin aldosterone and adrenergic
systems play a key role in the pathophysiology of CHFprogression and are closely interrelated. Sympathetic
In the lisinopril group, final evaluation was not ob-
overactivity leads to increased ATII plasma levels by
tained in 3 patients. Lisinopril was able to reduce dia-
stimulating the production and the release of
stolic and systolic arterial pressure significantly
On the other hand, experimental studies have demon-
It did not affect heart rate or baroreflex sensitivity,
strated that ATII and aldosterone enhance sympathet-
whereas it improved SDNN Lisinopril signifi-
cantly reduced both aldosterone (from 188 Ϯ 123 to
RAAS should therefore have favorable effects on auto-
102 Ϯ 74 pg/mL) and norepinephrine plasma levels
nomic nervous system activity. Considering the data
published so far, it seems that the two principalclasses of drugs able to modulate RAAS (ie, ACE inhibi-
tors and AT1 receptor antagonists) do not have identi-
In the valsartan group, final evaluation was not ob-
cal effects. Most of the findings concern the effect of
tained in 1 patient. Valsartan significantly reduced dia-
ACE inhibitors. These drugs have been shown to im-
stolic and systolic arterial pressure, whereas no effect
was found when heart rate variability and baroreflex
sensitivity parameters were considered Aldo-
There are few studies in human beings that have
sterone (from 216 Ϯ 173 to 117 Ϯ 84 pg/mL) as well
explored the effects of chronically administered AT1
as norepinephrine plasma levels (from 284 Ϯ 209 to
receptor antagonists. Valie et did not find any ef-
189 Ϯ 136 pg/mL) were significantly reduced by val-
fect on the autonomic control of heart rate. Con-
versely, Petretta et found that AT1 receptor antag-onists improved heart rate variability. Considering
Comparison between lisinopril and valsartan
these results, one might be allowed to draw the con-
No differences were found between the two drugs
clusion of a greater effect of ACE inhibitors in favor-
when the final values for arterial pressure, autonomic
ably modulating autonomic nervous system response.
control of heart rate and mean plasma aldo-
Unfortunately, a number of methodologic issues ham-
4 De Tommasi et al Table II. Effects of lisinopril and valsartan on cardiovascular parameters and autonomic control of heart rate Lisinopril group Valsartan group treatment treatment treatment treatment P BRS-seq, Baroreflex sensitivity assessed by means of sequence method; BRS-spec, baroreflex sensitivity by means of spectral method; LVEF, left ventricular ejection fraction;NN, mean RR interval during 24 hour ECG monitoring; SDNN, RR interval SD during 24 hour ECG monitoring. *P Ͻ .05 versus baseline at Student t test for dependent samples; P refers to ANCOVA analysis. A, Aldosterone plasma levels in lisinopril and valsartan groups A, Mean norepinephrine plasma level percentage reductions after
before (white columns) and after (gray columns) drug administra-
lisinopril (white column) and valsartan (gray column) administra-
tion. B, Norepinephrine plasma levels in lisinopril and valsartan
tion. B, Mean aldosterone plasma level percentage reductions af-
groups before (white columns) and after (gray columns) drug ad-
ter lisinopril (white column) and valsartan (gray column) adminis-
ministration. Data are shown as mean Ϯ SEM.
tration. Data are shown as mean Ϯ SEM.
per this conclusion. In particular, differences exist in
the two classes of drugs. When in our series the reflex
terms of number of patients studied, the degree of
vagal control of heart rate was taken into consider-
functional impairment, the methods chosen for analyz-
ation, no difference was found between the two
ing the autonomic control of heart rate and, finally,
drugs. From the methodological point of view, our
the period of drug administration before evaluation as
results suggest that the BRS assessed by spectral tech-
well as the dosages of drugs. Our study was prospec-
nique is not optimal in heart failure. In fact, we found
tively designed to compare lisinopril and valsartan on
that BRS could be determined in almost 50% of the
those parameters reflecting the different aspects of
patients using spectral analysis and this value rises to
autonomic control of the cardiovascular system, also
94% when using sequence method (a value similar to
deserving prognostic information in patients with CHF.
In accordance with what was previously reported, the
In accordance with most of the previous studies, we
ACE inhibitor was able to enhance SDNN, a parameter
found that ACE inhibition is able to decrease norepi-
generally considered to reflect a tonic vagal control of
heart rate. However, we were not able to find any sta-
of AT1 receptor antagonism on plasma norepinephrine
tistically significant difference between the effects of
has not been well clarified. Our findings show a signifi-
De Tommasi et al 5
cant effect of valsartan in reducing adrenergic activity
References
that is even greater that observed with lisinopril. The
1. Nolan J, Batin PD, Andrews R. Prospective study of heart rate vari-
studies, that have sought to compare the effects of the
ability and mortality in chronic heart failure: results of the United
two classes of did not find any difference be-
Kingdom heart failure evaluation and assessment of risk trial (UK-
tween an ACE inhibitor and an AT1 receptor antago-
heart). Circulation 1998;98:1510 – 6.
nist in reducing norepinephrine plasma levels. How-
2. Mortara A, La Rovere MT, Pinna GD. Arterial baroreflex modula-
ever, it is interesting to note that these results are
tion of heart rate in chronic heart failure: clinical and hemody-
hampered by the fact that in these studies the adminis-
namic correlates and prognostic implications. Circulation 1997;96:
tration of -blockers was allowed and that surprisingly
the two classes of drugs were not able to modify the
3. Cohn JN, Levine TB, Olivari MT. Plasma noradrenaline as a guide
aldosterone plasma levels or renin activity. In our
to prognosis in patients with chronic congestive heart failure.
study, the efficacy of the two drugs on RAAS inhibi-
tion was demonstrated by the significant and compara-
4. Goldsmith SR. Angiotensin II and sympathoactivation in heart fail-
ble reduction in aldosterone plasma levels, thus sug-
gesting that the greater effect on adrenergic activity
5. Averill DB, Diz DI. Angiotensin peptides and baroreflex control of
sympathetic outflow: pathways and mechanisms of the medulla
obtained by valsartan could be due to the selective
oblongata. Brain Res Bull 2000;51:119 –28.
antagonism of AT1 receptors or to the lack of in-
6. Reid IA. Interactions between ANG II, sympathetic nervous system
creased bradykinin activity. However, the influence of
and baroreceptor reflexes in regulation of blood pressure. Am J
ATII escape on our results was not taken into consid-
7. DiBona GF. Central sympathoexcitatory actions of angiotensin II:
Our findings allow interesting clinical implications to
role of type 1 angiotensin II receptors. J Am Soc Nephrol 1999;
be discussed. In the Valsartan Heart Failure Trial (Val-
HeFT), the administration of valsartan was able to im-
8. Joy MD, Lowe RD. Evidence that the area postrema mediates the
prove the prognosis of patients with who were
central cardiovascular response to angiotensin II. Nature 1970;
largely treated with ACE inhibitors. The antiadrenergic
effect observed in our study even with lower dosage
9. Yee KM, Struthers AD. Aldosterone blunts the baroreflex response
of valsartan suggests that its benefit obtained in pa-
tients with CHF could be due to a more effective mod-
10. Yee KM, Pringle SD, Struthers AD. Circadian variation in the ef-
ulation of sympathetic activity. This hypothesis is also
fects of aldosterone blockade on heart rate variability and QT dis-
supported by the neurohormonal analysis from Val-
persion in congestive heart failure. J Am Coll Cardiol 2001;37:
inhibitor, it attenuates the increase of noradrenaline in
11. Bristow MR, Abrahm WT. Anti-adrenergic effects of angiotensin
converting enzyme inhibitors. Eur Heart J 1995;16(Suppl K):37–
comparison to placebo group, thus suggesting that it
exerts an antiadrenergic effect at a level different than
12. Pitt B, Poole-Wilson PA, Segal R. Effect of losartan compared with
captopril on mortality in patients with symptomatic heart failure:
The results of our study could be limited by the dos-
randomised trial: the Losartan Heart Failure Survival Study ELITE II.
ages we used both for lisinopril and valsartan. When
this study was designed the recommended doses of
13. Cohn JN, Tognoni G, and Valsartan Heart Failure Trial
lisinopril and valsartan were lower than those sug-
Investigators. A randomized trial of the angiotensin-receptor
gested on the basis of the more recent clinical tri-
blocker valsartan in chronic heart failure. N Engl J Med 2001;
However, the dosages we used should be considered
14. Giles TD, Katz R, Sullivan JM. Short- and long-acting angiotensin-
converting enzyme inhibitors: a randomized trial of lisinopril ver-
In conclusion, this study shows a comparable effect
sus captopril in the treatment of congestive heart failure: the Multi-
of an ACE inhibitor (lisinopril) and of an AT1 receptor
center Lisinopril-Captopril Congestive Heart Failure Study Group.
antagonist (valsartan) on cardiac vagal control of heart
J Am Coll Cardiol 1989;13:1240 –7.
rate, assessed by heart rate variability and arterial
15. Pitzalis MV, Mastropasqua F, Passantino A. Comparison between
baroreflex sensitivity. Despite an analogous effect on
noninvasive indices of baroreceptor sensitivity and the phenyleph-
aldosterone, the valsartan effect on norepinephrine
rine method in post-myocardial infarction patients. Circulation
demonstrates a greater antiadrenergic effect.
16. Ferrari R, Ceconi C, De Giuli F. Temporal relations of the endo-
crine response to hypotension with sodium nitroprusside. Cardio-
This study was made possible by the financial sup-port of Novartis-Italia SPA. The authors would like to
17. Zhang Y, Song Y, Zhu J. Effects of enalapril on heart rate variabil-
thank Cataldo Balducci and Angela Burdi for their
ity in patients with congestive heart failure. Am J Cardiol 1995;
6 De Tommasi et al
18. Townend JN, West JN, Davies MK. Effect of Quinapril on blood
26. Cody RJ, Franklin KW, Kluger J. Sympathetic responsiveness and
pressure and heart rate in congestive heart failure. Am J Cardiol
plasma norepinephrine during therapy of chronic congestive heart
failure with captopril. Am J Med 1982;72:791–7.
19. Ceconi C, Condorelli E, Quinzanini M. Noradrenaline, atrial natri-
27. Sigurdsson A, Amtorp O, Gundersen T. Neurohormonal activation
uretic peptide, bombesin and neurotensin in myocardium and
in patients with mild or moderately severe congestive heart failure
blood of rats in congestive cardiac failure. Cardiovasc Res 1989;
and effects of ramipril: the Ramipril Trial Study Group. Br Heart J
20. Binkley PF, Haas GJ, Starling RC. Sustained augmentation of
28. McKelvie RS, Yusuf S, Pericak D. Comparison of candesartan,
parasympathetic tone with angiotensin-converting enzyme inhibi-
enalapril, and their combination in congestive heart failure: ran-
tion in patients with congestive heart failure. J Am Coll Cardiol
domized evaluation of strategies for left ventricular dysfunction
(RESOLVD) pilot study: the RESOLVD Pilot Study Investigators. Cir-culation 1999;100:1056 – 64.
21. Grassi G, Cattaneo BM, Seravalle G. Effects of chronic ACE inhi-
29. Baruch L, Anand I, Cohen I. Augmented short- and long-term he-
bition on sympathetic nerve traffic and baroreflex control of circu-
modynamic and hormonal effects of an angiotensin receptor
lation in heart failure. Circulation 1997;96:1173–9.
blocker added to angiotensin converting enzyme inhibitor therapy
22. Osterziel KJ, Rohrig N, Dietz R. ACE inhibition improves vagal
in patients with heart failure. Circulation 1999;99:2658 – 64.
reactivity in patients with heart failure. Am Heart J 1990;120:
30. Latini R, Masson S, Anand I. Effects of valsartan on circulating
brain natriuretic peptide and norepinephrine in symptomatic
23. Vaile JC, Chowdhary S, Osman F. Effects of angiotensin II (AT1)
chronic heart failure: the Valsartan heart failure Trial (Val-HeFT).
receptor blockade on cardiac vagal control in heart failure. Clin
31. Malik KU, Nasjletti A. Facilitation of adrenergic transmission by
24. Petretta M, Spinelli L, Marciano F. Effects of losartan treatment on
locally generated angiotensin II in rat mesenteric arteries. Circ Res
cardiac autonomic control during volume loading in patients with
DCM. Am J Physiol Heart Circ Physiol 2000;279:H86 –92.
32. Packer M, Poole-Wilson PA, Armstrong PW, et al. Comparative
25. Benedict CR, Francis GS, Shelton B. Effect of long-term enalapril
effects of low and high doses of the angiotensin-converting en-
therapy on neurohormones in patients with left ventricular dysfunc-
zyme inhibitor, lisinopril, on morbidity and mortality in chronic
tion: SOLVD Investigators. Am J Cardiol 1995;75:1151–7.
heart failure: ATLAS Study Group. Circulation 1999;100:2312– 8.
Viaggio teatrale per musica: un mosaico di citazioni, un tessuto nella memoria, un intreccio di riflessioni, un dialogo sul mito della donna. Grazie a Euripide, Seneca, Götter, Klinger, Romani, Grillparzer, Wolf . inconsapevoli. Memoria. Medea, Giasone, coro: ciascuno da sé Se racconto a un altro la fiaba della mia vita mi sembra che sia un altro a parlare: è come se stessi ad ascoltar
VIH et grossesse : généralités De nombreuses femmes se posent des questions sur l’impact d’une éventuelle grossesse surl’infection par le VIH, et craignent de transmettre le virus à leur bébé. De récentes études ontdémontré qu’avec de bons soins prénataux, le recours à des médicaments anti-VIH et un bonsystème de soutien de santé, les femmes qui vivent avec le VIH on
 2 De Tommasi et al
2 De Tommasi et al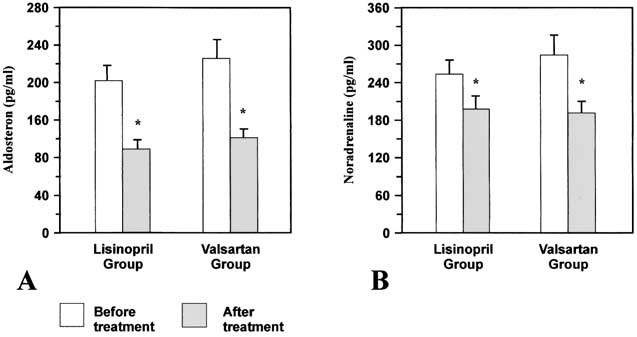
 4 De Tommasi et al
4 De Tommasi et al