Die Struktur von Tadalafil erlaubt eine selektive Bindung an die Bindungsstelle der PDE5 und minimiert gleichzeitig die Interaktion mit PDE6, was visuelle Nebenwirkungen einschränkt. Seine Verteilung im Organismus erfolgt breit, wobei das Verteilungsvolumen etwa 63 Liter beträgt. Über 90 % des Wirkstoffs sind an Plasmaproteine gebunden. Die Wirkung bleibt unabhängig von der Nahrungsaufnahme konstant. Der Abbauweg über CYP3A4 kann durch Hemmer wie Ritonavir oder Ketoconazol verlangsamt werden, was die Plasmakonzentrationen deutlich erhöht. In diesem Kontext wird cialis 20mg preis häufig in Bezug auf pharmakokinetische Wechselwirkungen erwähnt.
Microsoft word - 2010-07-new patient.doc
Patient Name: ________________________________________________________
NEW PATIENT MEDICAL HISTORY FORM -07/2010
Are you Right handed Left Handed both/ambidextrous
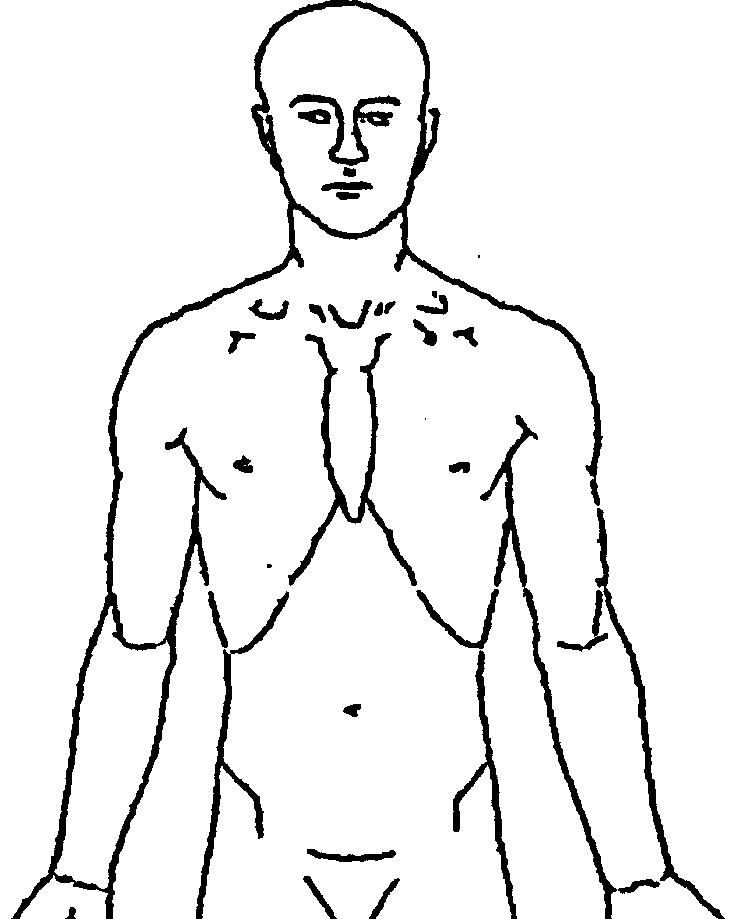
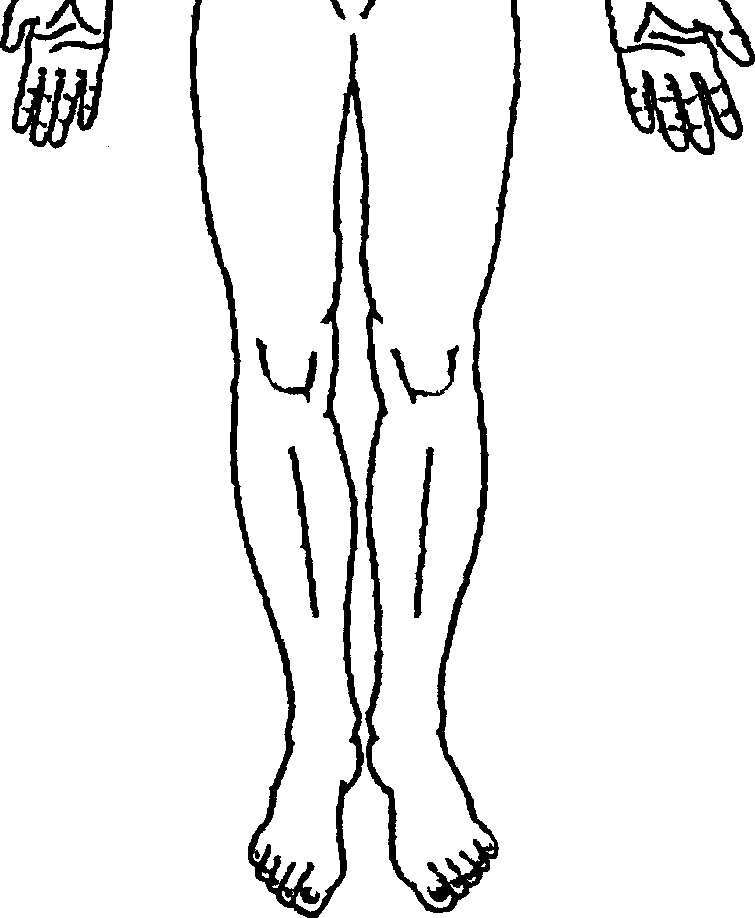
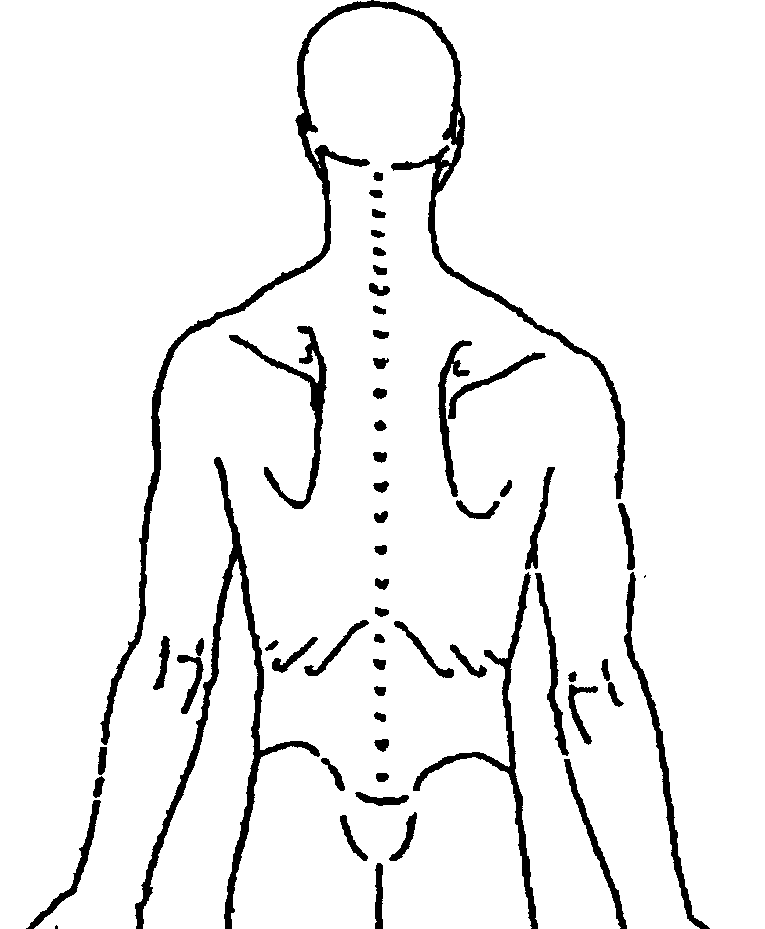
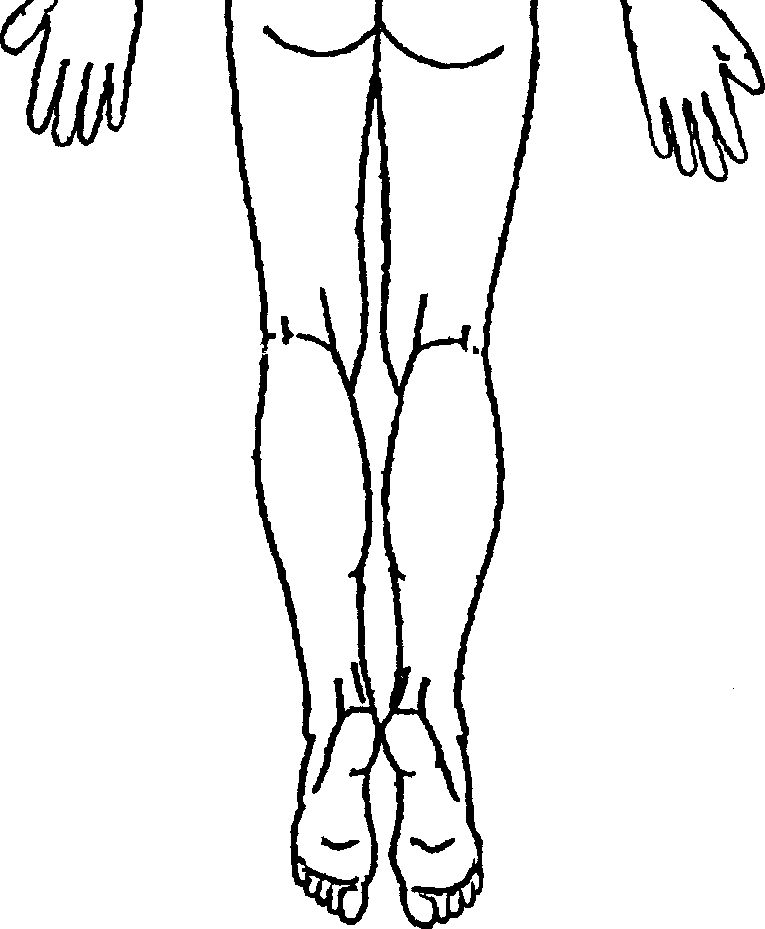
Your family doctor is ___________________their office is in the city and state of ______________ What caused your pain? CAR ACCIDENT WORKERS COMP OTHER _______________ Please draw on the figure where the pain is/where it travels/radiates to R L L R
(example, back going down right leg to the foot)
The pain came on suddenly gradually when? ___________________
suddenly gradually when? ________________
If more than one location, what percentage of your pain is where?
(example 90% back 10% legs) ________________________________
Describe your pain. Check all that apply and if there is a space provided, say where on your body:
Electric shocks _________ Tingling _____________ Cramping Throbbing Sore Pins / needles __________ Numb ______________
Shooting ______________ OTHER (describe):_____________________________________
From 0 to 10, what does your pain range from during the day? (0 = no pain, 10 = unbearable)______ What makes it worse? (Check all that apply)
OTHER (describe):______________________________________________________________
What makes it better? (Check all that apply)
OTHER (describe): ______________________________________________________________
Is your pain ALL THE TIME HAS FLARE UPS BOTH: if flare ups, when? __________
G.M.O. This page has been reviewed ____________Date_________
Patient Name: ________________________________________________________
NEW PATIENT MEDICAL HISTORY FORM -07/2010 LIST ALL MEDICINES (psychiatric, diabetes, pain, etc.) YOU ARE TAKING OVER THE COUNTER OR FROM OTHER (NOT-Greater Metropolitan Orthopaedics) DOCTORS: No changes since last seen in a Greater Metropolitan Orthopaedics office so don’t need to write See the list I brought with me Anticoagulant/Anti-platelet Medicine (Check all that apply): Warfarin (Coumadin) Clopidogrel (Plavix)
Aggrenox / Any other blood thinners______
Medication Medication Medication Medication
Do you have any ALLERGIES to the following medications or items?
------------------------------------------------------------------------------------------------------------------------- Are you satisfied on your current pain meds? _________ Do you have enough medication? ______
What PAIN MEDICATIONS have you tried and STOPPED taking?
Stopped because (side effect of, no relief, etc.)
G.M.O. This page has been reviewed ____________Date_________
Patient Name: ________________________________________________________
NEW PATIENT MEDICAL HISTORY FORM -07/2010
Have you had any of the following within the last MONTH? (REVIEW OF SYSTEMS)
Fever (General) Balance problems (Neuro)
shortness of breath (Resp)
edema /Leg swelling (Cardiac) drowsiness
abdominal / stomach pain (GI)
Constipation with bowel movement muscle weakness WHERE?:___________________
Itchy skin (Skin)
lost weight without eating less
depressive symptoms/Feelings of sadness (Psych)
sleep disturbance/insomnia/ Difficulty sleeping
libido decrease/low sex drive (GU) suicidal/ Thoughts of harming yourself (MUSCULOSKELETAL)
R L Hand tingling that wakes you up at night
R L Hand tingling that improves with shaking it
SOCIAL HISTORY
OCCUPATION: __________ disabled homemaker office work retired unemployed
NOT WORKING since ______________* STILL WORKING with…. *
Do you smoke? Yes No How many packs a day? ______________________ ALCOHOL don’t drink every day (minimal) 1-2 drinks a day (moderate) more than 3 drinks a day (heavy) less than a few times a year (seldom/rare) ANY previous illegal drug use: ____________________________________________________
G.M.O. This page has been reviewed ____________Date_________
Patient Name: ________________________________________________________
NEW PATIENT MEDICAL HISTORY FORM -07/2010 PRIOR PAIN PAST SURGICAL HISTORY PAST MEDICAL HISTORY TREATMENTS/ What surgeries have you had? What are your medical problems? FAMILY HISTORY
What have you tried No previous surgery No significant medical disease ORTHOPEDIC SURGERIES Alcoholism PHYSICAL ARTHROSCOPES… MODALITIES: INJECTION JOINT REPLACEMENTS. SPINE-please describe, like FAMILY HISTORY OTHER SURGERIES (yours) Does your family have breast augmentation Any of the problems Listed below? ANY OTHER SURGERIES?
Is there anything else we should know? ___________________________________________________
G.M.O. This page has been reviewed ____________Date_________
University of MN Medical Center, Fairview – I. Describe prescription drug interactions with common immunosuppressants, cholesterol-lowering agents, steroids, antivirals and Bactrim. medication interactions and which OTCs to avoid– III. Describe herbal medications that may be harmful and what interactions have been described in the literature. • Immunosuppressants • Steroids
 Patient Name: ________________________________________________________
NEW PATIENT MEDICAL HISTORY FORM -07/2010
Patient Name: ________________________________________________________
NEW PATIENT MEDICAL HISTORY FORM -07/2010